Journal of Allergy and Clinical Immunology ( IF 11.4 ) Pub Date : 2018-01-31 , DOI: 10.1016/j.jaci.2017.10.052 Cristina Longo , Gillian Bartlett , Tibor Schuster , Francine M. Ducharme , Brenda MacGibbon , Tracie A. Barnett
|
Background
Current evidence regarding the relationship between childhood obesity, decreased response to inhaled corticosteroids (ICSs), and poor asthma control is conflicting.
Objectives
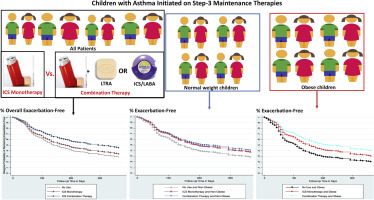
We assessed whether obesity (1) is associated with time to first exacerbation among children with asthma initiating step 3 maintenance therapies and (2) modifies the effectiveness of step 3 therapies.
Methods
A retrospective cohort study was conducted from clinical data linked to health and drug administrative databases. The cohort consisted of children aged 2 to 18 years with specialist-confirmed asthma who initiated medium/high-dose ICS monotherapy or low/medium-dose ICS with leukotriene receptor antagonist/long-acting β-agonist (combination therapy) at the Montreal Children's Hospital Asthma Center from 2000 to 2007. Children were classified as exposed to step 3 therapies when they were dispensed a corresponding drug claim during follow-up, whereas those without claims were classified as nonadherers. Marginal structural Cox models were used to estimate the effect of obesity (body mass index > 97th percentile) and treatment on time to exacerbation, which was defined as any emergency department visit, hospitalization, or use of oral corticosteroids for asthma.
Results
Of the 4621 cohort patients, 231 initiated ICS monotherapy, and 97 initiated combination therapy. The hazard ratio (HR) for obesity was 1.67 (95% CI, 1.41-1.98). Compared with nonobese nonadherers, the HR for obese nonadherers was 1.54 (95% CI, 0.97-2.45); the HR for ICS monotherapy in obese and nonobese children was 0.85 (95% CI, 0.47-1.52) and 0.58 (95% CI, 0.37-0.91), respectively; and the HR for combination therapy in obese and nonobese children was 0.50 (95% CI, 0.13-1.89) and 0.46 (95% CI, 0.23-0.92), respectively.
Conclusion
Obesity might be a determinant of shorter exacerbation-free time in children with asthma; however, we could not rule out a differential response to step 3 therapies by obesity status, potentially because of a lack of precision.
中文翻译:
儿童肥胖-哮喘表型:情况恶化吗?
背景
有关儿童肥胖,对吸入皮质类固醇激素(ICSs)的反应降低以及哮喘控制不良之间的关系的最新证据相互矛盾。
目标
我们评估了肥胖(1)是否与哮喘发作儿童开始第3步维持疗法的时间和首次加重时间有关,以及(2)修改了第3步疗法的有效性。
方法
一项回顾性队列研究是根据与健康和药物管理数据库相关的临床数据进行的。该队列包括2到18岁患有哮喘病的专家确认的儿童,他们在蒙特利尔儿童医院启动了中/高剂量ICS单药治疗或采用白三烯受体拮抗剂/长效β激动剂的低/中剂量ICS联合治疗。从2000年到2007年,是医院哮喘中心。在随访期间为儿童分配了相应的药物索赔时,他们被分类为接受第3步疗法的治疗,而没有索赔的孩子则被分类为非依从性的治疗。边缘结构Cox模型用于评估肥胖(体重指数> 97%)和治疗对恶化时间的影响,定义为任何急诊就诊,住院,
结果
在4621例队列患者中,231例开始了ICS单药治疗,97例开始了联合治疗。肥胖的风险比(HR)为1.67(95%CI,1.41-1.98)。与非肥胖非粘附者相比,肥胖非粘附者的HR为1.54(95%CI,0.97-2.45);肥胖和非肥胖儿童ICS单一疗法的HR分别为0.85(95%CI,0.47-1.52)和0.58(95%CI,0.37-0.91);肥胖和非肥胖儿童联合治疗的HR分别为0.50(95%CI,0.13-1.89)和0.46(95%CI,0.23-0.92)。
结论
肥胖可能是哮喘患儿无急性发作时间缩短的决定因素。但是,我们不能排除肥胖状况对第3步疗法有不同的反应,这可能是由于缺乏精确性所致。










































 京公网安备 11010802027423号
京公网安备 11010802027423号