Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Association of Bariatric Surgery vs Medical Obesity Treatment With Long-term Medical Complications and Obesity-Related Comorbidities
JAMA ( IF 63.1 ) Pub Date : 2018-01-16 , DOI: 10.1001/jama.2017.21055 Gunn Signe Jakobsen 1 , Milada Cvancarova Småstuen 1 , Rune Sandbu 1, 2 , Njord Nordstrand 1 , Dag Hofsø 1 , Morten Lindberg 3 , Jens Kristoffer Hertel 1 , Jøran Hjelmesæth 1, 4
JAMA ( IF 63.1 ) Pub Date : 2018-01-16 , DOI: 10.1001/jama.2017.21055 Gunn Signe Jakobsen 1 , Milada Cvancarova Småstuen 1 , Rune Sandbu 1, 2 , Njord Nordstrand 1 , Dag Hofsø 1 , Morten Lindberg 3 , Jens Kristoffer Hertel 1 , Jøran Hjelmesæth 1, 4
Affiliation
|
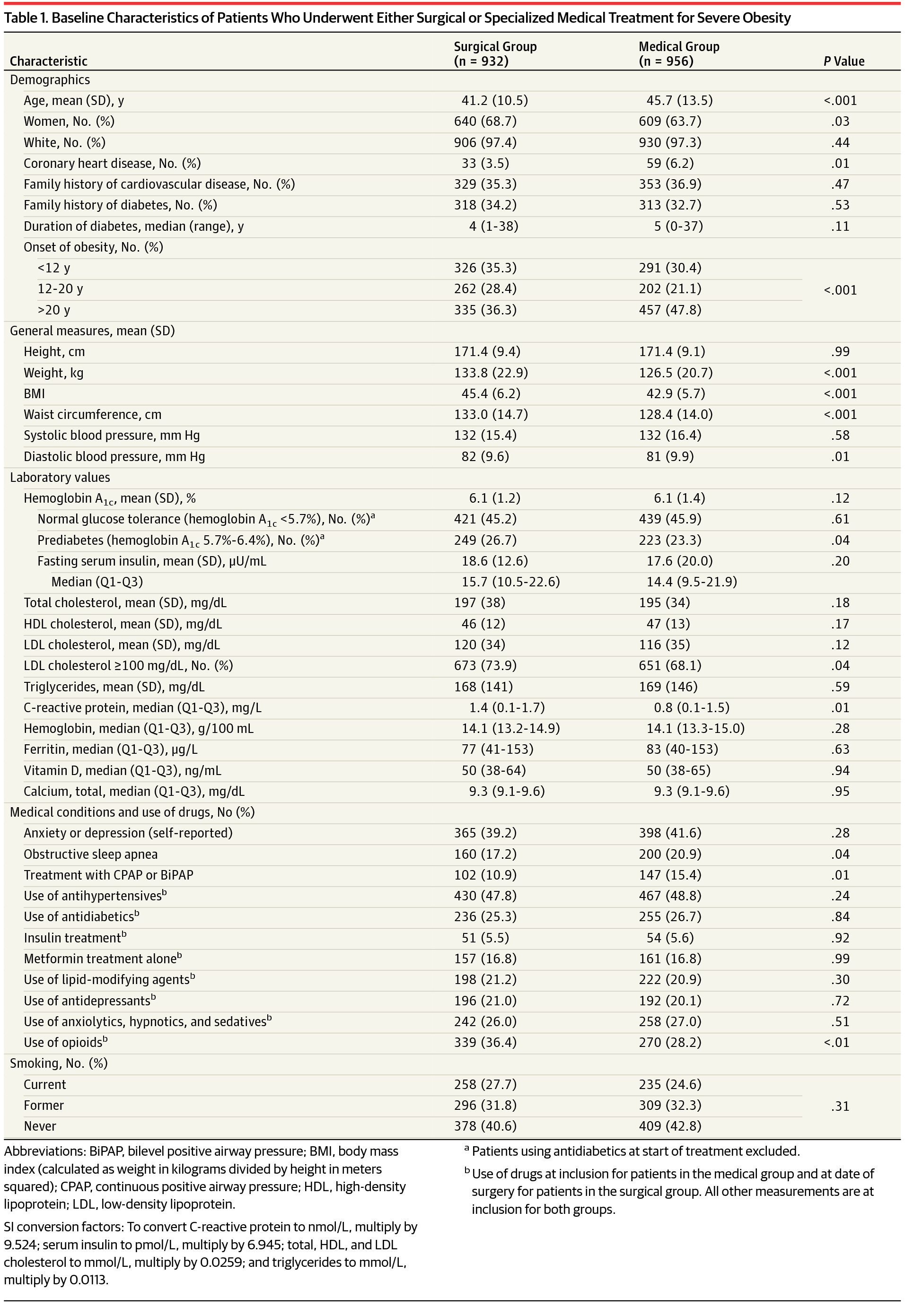
Importance The association of bariatric surgery and specialized medical obesity treatment with beneficial and detrimental outcomes remains uncertain. Objective To compare changes in obesity-related comorbidities in patients with severe obesity (body mass index ≥40 or ≥35 and at least 1 comorbidity) undergoing bariatric surgery or specialized medical treatment. Design, Setting, and Participants Cohort study with baseline data of exposures from November 2005 through July 2010 and follow-up data from 2006 until death or through December 2015 at a tertiary care outpatient center, Vestfold Hospital Trust, Norway. Consecutive treatment-seeking adult patients (n = 2109) with severe obesity assessed (221 patients excluded and 1888 patients included). Exposures Bariatric surgery (n = 932, 92% gastric bypass) or specialized medical treatment (n = 956) including individual or group-based lifestyle intervention programs. Main Outcomes and Measures Primary outcomes included remission and new onset of hypertension based on drugs dispensed according to the Norwegian Prescription Database. Prespecified secondary outcomes included changes in comorbidities. Adverse events included complications retrieved from the Norwegian Patient Registry and a local laboratory database. Results Among 1888 patients included in the study, the mean (SD) age was 43.5 (12.3) years (1249 women [66%]; mean [SD] baseline BMI, 44.2 [6.1]; 100% completed follow-up at a median of 6.5 years [range, 0.2-10.1]). Surgically treated patients had a greater likelihood of remission and lesser likelihood for new onset of hypertension (remission: absolute risk [AR], 31.9% vs 12.4%); risk difference [RD], 19.5% [95% CI, 15.8%-23.2%], relative risk [RR], 2.1 [95% CI, 2.0-2.2]; new onset: AR, 3.5% vs 12.2%, RD, 8.7% [95% CI, 6.7%-10.7%], RR, 0.4 [95% CI, 0.3-0.5]; greater likelihood of diabetes remission: AR, 57.5% vs 14.8%; RD, 42.7% [95% CI, 35.8%-49.7%], RR, 3.9 [95% CI, 2.8-5.4]; greater risk of new-onset depression: AR, 8.9% vs 6.5%; RD, 2.4% [95% CI, 1.3%-3.5%], RR, 1.5 [95% CI, 1.4-1.7]; and treatment with opioids: AR, 19.4% vs 15.8%, RD, 3.6% [95% CI, 2.3%-4.9%], RR, 1.3 [95% CI, 1.2-1.4]). Surgical patients had a greater risk for undergoing at least 1 additional gastrointestinal surgical procedure (AR, 31.3% vs 15.5%; RD, 15.8% [95% CI, 13.1%-18.5%]; RR, 2.0 [95% CI, 1.7-2.4]). The proportion of patients with low ferritin levels was significantly greater in the surgical group (26% vs 12%, P < .001). Conclusions and Relevance Among patients with severe obesity followed up for a median of 6.5 years, bariatric surgery compared with medical treatment was associated with a clinically important increased risk for complications, as well as lower risks of obesity-related comorbidities. The risk for complications should be considered in the decision-making process.
中文翻译:

减肥手术与内科肥胖治疗与长期内科并发症和肥胖相关合并症的关联
重要性 减肥手术和专门的肥胖医学治疗与有益和有害结果的关联仍然不确定。目的 比较接受减肥手术或专科治疗的重度肥胖患者(体重指数≥40 或≥35 且至少有 1 种合并症)的肥胖相关合并症的变化。设计、设置和参与者 队列研究包含 2005 年 11 月至 2010 年 7 月的暴露基线数据和 2006 年至死亡或至 2015 年 12 月在挪威 Vestfold 医院信托的三级护理门诊中心的随访数据。对严重肥胖的连续寻求治疗的成年患者(n = 2109)进行评估(排除 221 名患者,包括 1888 名患者)。暴露减肥手术(n = 932,92% 的胃绕道手术)或专门的医疗(n = 956),包括个人或基于团体的生活方式干预计划。主要结果和措施 主要结果包括根据挪威处方数据库分配的药物缓解和新发高血压。预先指定的次要结果包括合并症的变化。不良事件包括从挪威患者登记处和当地实验室数据库中检索到的并发症。结果 在纳入研究的 1888 名患者中,平均 (SD) 年龄为 43.5 (12.3) 岁(1249 名女性 [66%];平均 [SD] 基线 BMI,44.2 [6.1];100% 完成中位随访) 6.5 年 [范围,0.2-10.1])。接受手术治疗的患者缓解的可能性更大,而新发高血压的可能性更小(缓解:绝对风险 [AR],31. 9% 对 12.4%);风险差异 [RD],19.5% [95% CI,15.8%-23.2%],相对风险 [RR],2.1 [95% CI,2.0-2.2];新发病:AR,3.5% vs 12.2%,RD,8.7% [95% CI,6.7%-10.7%],RR,0.4 [95% CI,0.3-0.5];糖尿病缓解的可能性更大:AR,57.5% vs 14.8%;RD,42.7% [95% CI,35.8%-49.7%],RR,3.9 [95% CI,2.8-5.4];新发抑郁症的风险更大:AR,8.9% vs 6.5%;RD,2.4% [95% CI,1.3%-3.5%],RR,1.5 [95% CI,1.4-1.7];和阿片类药物治疗:AR,19.4% vs 15.8%,RD,3.6% [95% CI,2.3%-4.9%],RR,1.3 [95% CI,1.2-1.4])。外科患者接受至少 1 次额外胃肠道外科手术的风险更高(AR,31.3% vs 15.5%;RD,15.8% [95% CI,13.1%-18.5%];RR,2.0 [95% CI,1.7- 2.4])。手术组中铁蛋白水平低的患者比例明显更高(26% vs 12%,P < .001)。结论和相关性 在中位随访 6.5 年的重度肥胖患者中,与药物治疗相比,减肥手术与临床上重要的并发症风险增加以及肥胖相关合并症的风险降低相关。在决策过程中应考虑并发症的风险。
更新日期:2018-01-16
中文翻译:
减肥手术与内科肥胖治疗与长期内科并发症和肥胖相关合并症的关联
重要性 减肥手术和专门的肥胖医学治疗与有益和有害结果的关联仍然不确定。目的 比较接受减肥手术或专科治疗的重度肥胖患者(体重指数≥40 或≥35 且至少有 1 种合并症)的肥胖相关合并症的变化。设计、设置和参与者 队列研究包含 2005 年 11 月至 2010 年 7 月的暴露基线数据和 2006 年至死亡或至 2015 年 12 月在挪威 Vestfold 医院信托的三级护理门诊中心的随访数据。对严重肥胖的连续寻求治疗的成年患者(n = 2109)进行评估(排除 221 名患者,包括 1888 名患者)。暴露减肥手术(n = 932,92% 的胃绕道手术)或专门的医疗(n = 956),包括个人或基于团体的生活方式干预计划。主要结果和措施 主要结果包括根据挪威处方数据库分配的药物缓解和新发高血压。预先指定的次要结果包括合并症的变化。不良事件包括从挪威患者登记处和当地实验室数据库中检索到的并发症。结果 在纳入研究的 1888 名患者中,平均 (SD) 年龄为 43.5 (12.3) 岁(1249 名女性 [66%];平均 [SD] 基线 BMI,44.2 [6.1];100% 完成中位随访) 6.5 年 [范围,0.2-10.1])。接受手术治疗的患者缓解的可能性更大,而新发高血压的可能性更小(缓解:绝对风险 [AR],31. 9% 对 12.4%);风险差异 [RD],19.5% [95% CI,15.8%-23.2%],相对风险 [RR],2.1 [95% CI,2.0-2.2];新发病:AR,3.5% vs 12.2%,RD,8.7% [95% CI,6.7%-10.7%],RR,0.4 [95% CI,0.3-0.5];糖尿病缓解的可能性更大:AR,57.5% vs 14.8%;RD,42.7% [95% CI,35.8%-49.7%],RR,3.9 [95% CI,2.8-5.4];新发抑郁症的风险更大:AR,8.9% vs 6.5%;RD,2.4% [95% CI,1.3%-3.5%],RR,1.5 [95% CI,1.4-1.7];和阿片类药物治疗:AR,19.4% vs 15.8%,RD,3.6% [95% CI,2.3%-4.9%],RR,1.3 [95% CI,1.2-1.4])。外科患者接受至少 1 次额外胃肠道外科手术的风险更高(AR,31.3% vs 15.5%;RD,15.8% [95% CI,13.1%-18.5%];RR,2.0 [95% CI,1.7- 2.4])。手术组中铁蛋白水平低的患者比例明显更高(26% vs 12%,P < .001)。结论和相关性 在中位随访 6.5 年的重度肥胖患者中,与药物治疗相比,减肥手术与临床上重要的并发症风险增加以及肥胖相关合并症的风险降低相关。在决策过程中应考虑并发症的风险。










































 京公网安备 11010802027423号
京公网安备 11010802027423号