Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Association of Bariatric Surgery Using Laparoscopic Banding, Roux-en-Y Gastric Bypass, or Laparoscopic Sleeve Gastrectomy vs Usual Care Obesity Management With All-Cause Mortality
JAMA ( IF 63.1 ) Pub Date : 2018-01-16 , DOI: 10.1001/jama.2017.20513 Orna Reges 1, 2 , Philip Greenland 3, 4 , Dror Dicker 5, 6, 7 , Morton Leibowitz 1, 8 , Moshe Hoshen 1 , Ilan Gofer 1 , Laura J. Rasmussen-Torvik 3 , Ran D. Balicer 1, 9
JAMA ( IF 63.1 ) Pub Date : 2018-01-16 , DOI: 10.1001/jama.2017.20513 Orna Reges 1, 2 , Philip Greenland 3, 4 , Dror Dicker 5, 6, 7 , Morton Leibowitz 1, 8 , Moshe Hoshen 1 , Ilan Gofer 1 , Laura J. Rasmussen-Torvik 3 , Ran D. Balicer 1, 9
Affiliation
|
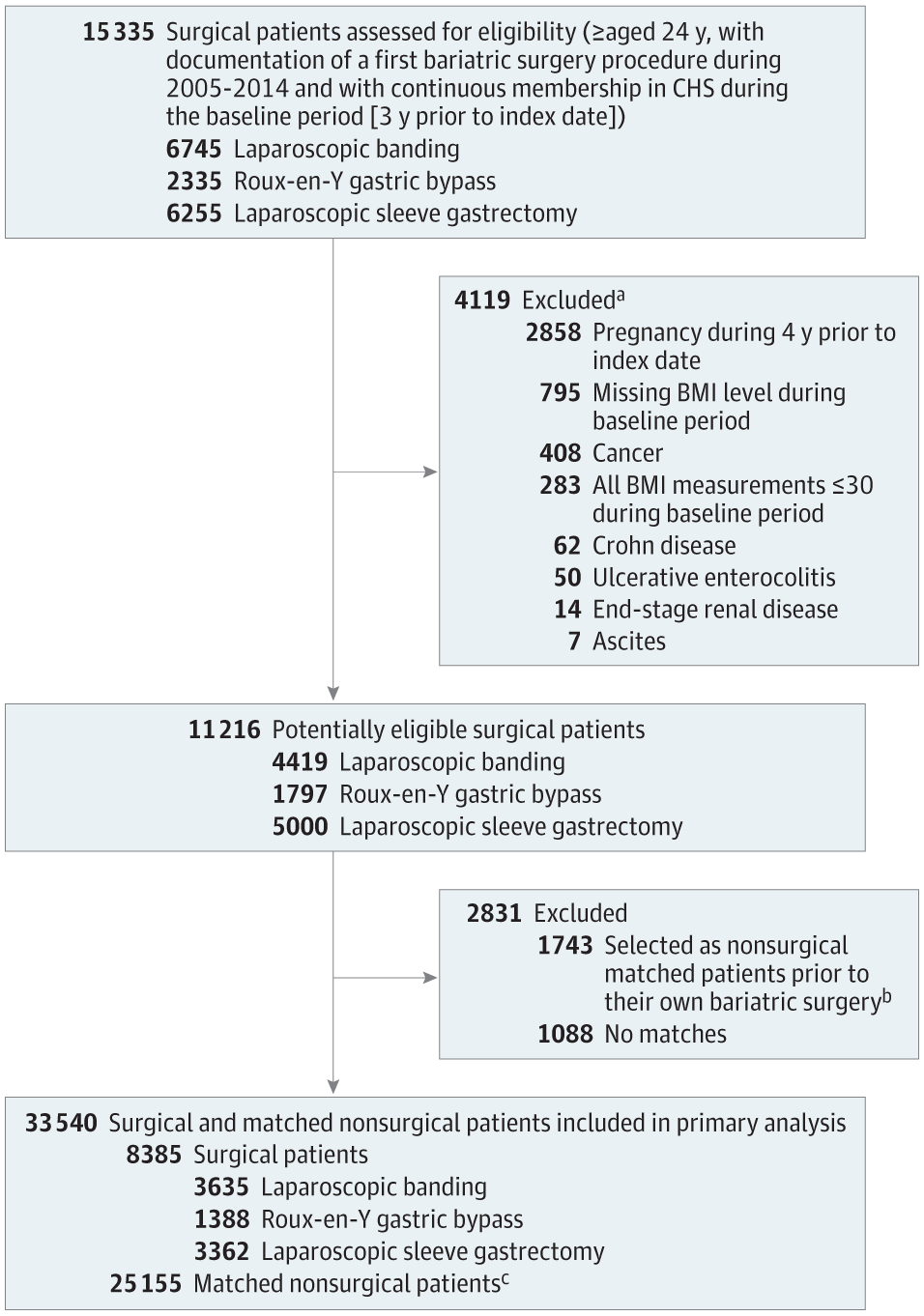
Importance Bariatric surgery is an effective and safe approach for weight loss and short-term improvement in metabolic disorders such as diabetes. However, studies have been limited in most settings by lack of a nonsurgical group, losses to follow-up, missing data, and small sample sizes in clinical trials and observational studies. Objective To assess the association of 3 common types of bariatric surgery compared with nonsurgical treatment with mortality and other clinical outcomes among obese patients. Design, Setting, and Participants Retrospective cohort study in a large Israeli integrated health fund covering 54% of Israeli citizens with less than 1% turnover of members annually. Obese adult patients who underwent bariatric surgery between January 1, 2005, and December 31, 2014, were selected and compared with obese nonsurgical patients matched on age, sex, body mass index (BMI), and diabetes, with a final follow-up date of December 31, 2015. A total of 33 540 patients were included in this study. Exposures Bariatric surgery (laparoscopic banding, Roux-en-Y gastric bypass, or laparoscopic sleeve gastrectomy) or usual care obesity management only (provided by a primary care physician and which may include dietary counseling and behavior modification). Main Outcomes and Measures The primary outcome, all-cause mortality, matched and adjusted for BMI prior to surgery, age, sex, socioeconomic status, diabetes, hyperlipidemia, hypertension, cardiovascular disease, and smoking. Results The study population included 8385 patients who underwent bariatric surgery (median age, 46 [IQR, 37-54] years; 5490 [65.5%] women; baseline median BMI, 40.6 [IQR, 38.5-43.7]; laparoscopic banding [n = 3635], gastric bypass [n = 1388], laparoscopic sleeve gastrectomy [n = 3362], and 25 155 nonsurgical matched patients (median age, 46 [IQR, 37-54] years; 16 470 [65.5%] women; baseline median BMI, 40.5 [IQR, 37.0-43.5]). The availability of follow-up data was 100% for all-cause mortality. There were 105 deaths (1.3%) among surgical patients during a median follow-up of 4.3 (IQR, 2.8-6.6) years (including 61 [1.7%] who underwent laparoscopic banding, 18 [1.3%] gastric bypass, and 26 [0.8%] sleeve gastrectomy), and 583 deaths (2.3%) among nonsurgical patients during a median follow-up of 4.0 (IQR, 2.6-6.2) years. The absolute difference was 2.51 (95% CI, 1.86-3.15) fewer deaths/1000 person-years in the surgical vs nonsurgical group. Adjusted hazard ratios (HRs) for mortality among nonsurgical vs surgical patients were 2.02 (95% CI, 1.63-2.52) for the entire study population; by surgical type, HRs were 2.01 (95% CI, 1.50-2.69) for laparoscopic banding, 2.65 (95% CI, 1.55-4.52) for gastric bypass, and 1.60 (95% CI, 1.02-2.51) for laparoscopic sleeve gastrectomy. Conclusions and Relevance Among obese patients in a large integrated health fund in Israel, bariatric surgery using laparoscopic banding, gastric bypass, or laparoscopic sleeve gastrectomy, compared with usual care nonsurgical obesity management, was associated with lower all-cause mortality over a median follow-up of approximately 4.5 years. The evidence of this association adds to the limited literature describing beneficial outcomes of these 3 types of bariatric surgery compared with usual care obesity management alone.
中文翻译:

使用腹腔镜束带、Roux-en-Y 胃旁路术或腹腔镜袖状胃切除术的减肥手术与具有全因死亡率的常规护理肥胖管理的关联
重要性 减肥手术是减轻体重和短期改善代谢紊乱(如糖尿病)的有效且安全的方法。然而,由于缺乏非手术组、失访、数据缺失以及临床试验和观察性研究的样本量小,在大多数情况下的研究受到限制。目的 评估 3 种常见类型的减肥手术与非手术治疗相比,肥胖患者的死亡率和其他临床结果之间的关联。设计、设置和参与者 一项大型以色列综合医疗基金的回顾性队列研究,覆盖 54% 的以色列公民,每年成员流动率低于 1%。2005年1月1日至2014年12月31日期间接受减肥手术的肥胖成年患者,选择并与年龄、性别、体重指数 (BMI) 和糖尿病相匹配的肥胖非手术患者进行比较,最终随访日期为 2015 年 12 月 31 日。本研究共纳入 33 540 名患者。暴露减肥手术(腹腔镜束带、Roux-en-Y 胃绕道术或腹腔镜袖状胃切除术)或仅常规护理肥胖管理(由初级保健医生提供,可能包括饮食咨询和行为矫正)。主要结果和测量主要结果,全因死亡率,匹配和调整术前 BMI、年龄、性别、社会经济状况、糖尿病、高脂血症、高血压、心血管疾病和吸烟。结果 研究人群包括 8385 名接受减肥手术的患者(中位年龄,46 [IQR,37-54] 岁;5490 [65.5%] 名女性;基线中位 BMI,40.6 [IQR,38.5-43.7];腹腔镜束带 [n = 3635]、胃旁路术 [n = 1388]、腹腔镜袖状胃切除术 [n = 3362] 和 25 155 名非手术匹配患者(中位年龄,46 [IQR,37-54] 岁;16 470 [65.5%] ] 女性;基线中位数 BMI,40.5 [IQR,37.0-43.5])。全因死亡率的随访数据的可用性为 100%。在中位随访 4.3 (IQR, 2.8-6.6) 年期间,手术患者中有 105 人 (1.3%) 死亡(其中 61 [1.7%] 接受了腹腔镜绑扎术,18 [1.3%] 0.8%] 袖状胃切除术),在 4.0(IQR,2.6-6.2)年的中位随访期间,非手术患者中有 583 人死亡(2.3%)。手术组与非手术组的绝对差异为 2.51(95% CI,1.86-3.15)死亡/1000 人年。对于整个研究人群,非手术与手术患者死亡率的调整风险比 (HR) 为 2.02(95% CI,1.63-2.52);按手术类型,腹腔镜套扎术的 HR 为 2.01(95% CI,1.50-2.69),胃旁路术的 HR 为 2.65(95% CI,1.55-4.52),腹腔镜袖状胃切除术的 HR 为 1.60(95% CI,1.02-2.51)。结论和相关性 在以色列大型综合医疗基金的肥胖患者中,与常规护理非手术肥胖管理相比,使用腹腔镜束带、胃绕道或腹腔镜袖状胃切除术的减肥手术与中位随访期间的全因死亡率较低相关。大约 4.5 年。
更新日期:2018-01-16
中文翻译:
使用腹腔镜束带、Roux-en-Y 胃旁路术或腹腔镜袖状胃切除术的减肥手术与具有全因死亡率的常规护理肥胖管理的关联
重要性 减肥手术是减轻体重和短期改善代谢紊乱(如糖尿病)的有效且安全的方法。然而,由于缺乏非手术组、失访、数据缺失以及临床试验和观察性研究的样本量小,在大多数情况下的研究受到限制。目的 评估 3 种常见类型的减肥手术与非手术治疗相比,肥胖患者的死亡率和其他临床结果之间的关联。设计、设置和参与者 一项大型以色列综合医疗基金的回顾性队列研究,覆盖 54% 的以色列公民,每年成员流动率低于 1%。2005年1月1日至2014年12月31日期间接受减肥手术的肥胖成年患者,选择并与年龄、性别、体重指数 (BMI) 和糖尿病相匹配的肥胖非手术患者进行比较,最终随访日期为 2015 年 12 月 31 日。本研究共纳入 33 540 名患者。暴露减肥手术(腹腔镜束带、Roux-en-Y 胃绕道术或腹腔镜袖状胃切除术)或仅常规护理肥胖管理(由初级保健医生提供,可能包括饮食咨询和行为矫正)。主要结果和测量主要结果,全因死亡率,匹配和调整术前 BMI、年龄、性别、社会经济状况、糖尿病、高脂血症、高血压、心血管疾病和吸烟。结果 研究人群包括 8385 名接受减肥手术的患者(中位年龄,46 [IQR,37-54] 岁;5490 [65.5%] 名女性;基线中位 BMI,40.6 [IQR,38.5-43.7];腹腔镜束带 [n = 3635]、胃旁路术 [n = 1388]、腹腔镜袖状胃切除术 [n = 3362] 和 25 155 名非手术匹配患者(中位年龄,46 [IQR,37-54] 岁;16 470 [65.5%] ] 女性;基线中位数 BMI,40.5 [IQR,37.0-43.5])。全因死亡率的随访数据的可用性为 100%。在中位随访 4.3 (IQR, 2.8-6.6) 年期间,手术患者中有 105 人 (1.3%) 死亡(其中 61 [1.7%] 接受了腹腔镜绑扎术,18 [1.3%] 0.8%] 袖状胃切除术),在 4.0(IQR,2.6-6.2)年的中位随访期间,非手术患者中有 583 人死亡(2.3%)。手术组与非手术组的绝对差异为 2.51(95% CI,1.86-3.15)死亡/1000 人年。对于整个研究人群,非手术与手术患者死亡率的调整风险比 (HR) 为 2.02(95% CI,1.63-2.52);按手术类型,腹腔镜套扎术的 HR 为 2.01(95% CI,1.50-2.69),胃旁路术的 HR 为 2.65(95% CI,1.55-4.52),腹腔镜袖状胃切除术的 HR 为 1.60(95% CI,1.02-2.51)。结论和相关性 在以色列大型综合医疗基金的肥胖患者中,与常规护理非手术肥胖管理相比,使用腹腔镜束带、胃绕道或腹腔镜袖状胃切除术的减肥手术与中位随访期间的全因死亡率较低相关。大约 4.5 年。








































 京公网安备 11010802027423号
京公网安备 11010802027423号