JAMA Oncology ( IF 22.5 ) Pub Date : 2018-03-01 , DOI: 10.1001/jamaoncol.2017.4600 Binod Dhakal 1 , Aniko Szabo 2 , Saurabh Chhabra 1 , Mehdi Hamadani 1 , Anita D'Souza 1 , Saad Z Usmani 3 , Rita Sieracki 4 , Bishal Gyawali 5 , Jeffrey L Jackson 6 , Fotis Asimakopoulos 7 , Parameswaran N Hari 1
|
Importance The role of high-dose therapy with melphalan followed by autologous stem cell transplant (HDT/ASCT) in patients with multiple myeloma continues to be debated in the context of novel agent induction.
Objective To perform a systematic review, conventional meta-analysis, and network meta-analysis of all phase 3 randomized clinical trials (RCTs) evaluating the role of HDT/ASCT.
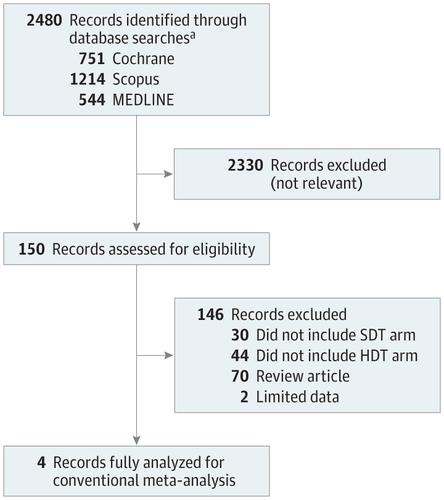
Data Sources We performed a systematic literature search of Cochrane Central, MEDLINE, and Scopus from January 2000 through April 2017 and relevant annual meeting abstracts from January 2014 to December 2016. The following search terms were used: “myeloma” combined with “autologous,” “transplant,” “myeloablative,” or “stem cell.”
Study Selection Phase 3 RCTs comparing HDT/ASCT with standard-dose therapy (SDT) using novel agents were assessed. Studies comparing single HDT/ASCT with bortezomib, lenalidomide, and dexamethasone consolidation and tandem transplantation were included for network meta-analysis.
Data Extraction And Synthesis For the random effects meta-analysis, we used hazard ratios (HRs) and corresponding 95% CIs.
Main Outcomes and Measures The primary outcome was progression-free survival (PFS). Overall survival (OS), complete response, and treatment-related mortality were secondary outcomes.
Results A total of 4 RCTs (2421 patients) for conventional meta-analysis and 5 RCTs (3171 patients) for network meta-analysis were selected. The combined odds for complete response were 1.27 (95% CI, 0.97-1.65; P = .07) with HDT/ASCT when compared with SDT. The combined HR for PFS was 0.55 (95% CI, 0.41-0.74; P < .001) and 0.76 for OS (95% CI, 0.42-1.36; P = .20) in favor of HDT. Meta-regression showed that longer follow-up was associated with superior PFS (HR/mo, 0.98; 95% CI, 0.96-0.99; P = .03) and OS (HR/mo, 0.90; 95% CI, 0.84-0.96; P = .002). For PFS, tandem HDT/ASCT had the most favorable HR (0.49; 95% CI, 0.37-0.65) followed by single HDT/ASCT with bortezomib, lenalidomide, and dexamethasone (HR, 0.53; 95% CI, 0.37-0.76) and single HDT/ASCT alone (HR, 0.68; 95% CI, 0.53-0.87) compared with SDT. For OS, none of the HDT/ASCT-based approaches had a significant effect on survival. Treatment-related mortality with HDT/ASCT was minimal (<1%).
Conclusions and Relevance The results of the conventional meta-analysis and network meta-analysis of all the phase 3 RCTs showed that HDT/ASCT was associated with superior PFS with minimal toxic effects compared with SDT. Both tandem HDT/ASCT and single HDT/ASCT with bortezomib, lenalidomide, and dexamethasone were superior to single HDT/ASCT alone and SDT for PFS, but OS was similar across the 4 approaches. Longer follow-up may better delineate any OS benefit; however, is likely to be affected by effective postrelapse therapy.
中文翻译:
新药诱导时代新诊断多发性骨髓瘤的自体移植系统评价和荟萃分析
重要性 在新型药物诱导的背景下,继续对多发性骨髓瘤患者进行高剂量美法仑治疗后自体干细胞移植 (HDT/ASCT) 的作用进行辩论。
目的 对评估 HDT/ASCT 作用的所有 3 期随机临床试验 (RCT) 进行系统评价、常规荟萃分析和网络荟萃分析。
数据来源 我们对 2000 年 1 月至 2017 年 4 月的 Cochrane Central、MEDLINE 和 Scopus 以及 2014 年 1 月至 2016 年 12 月的相关年会摘要进行了系统的文献检索。使用了以下检索词:“骨髓瘤”与“自体”相结合, “移植”、“清髓”或“干细胞”。
评估了比较 HDT/ASCT 与使用新型药物的标准剂量治疗 (SDT) 的研究选择阶段 3 RCT。网络荟萃分析纳入了比较单一 HDT/ASCT 与硼替佐米、来那度胺和地塞米松巩固和串联移植的研究。
数据提取和综合 对于随机效应荟萃分析,我们使用了风险比 (HR) 和相应的 95% CI。
主要结果和措施 主要结果是无进展生存期 (PFS)。总生存期(OS)、完全缓解和治疗相关死亡率是次要结局。
结果 共选择4篇RCTs(2421例患者)进行常规meta分析,5篇RCTs(3171例患者)进行网络meta分析。 与 SDT 相比,HDT/ASCT的完全缓解综合几率为 1.27(95% CI,0.97-1.65;P = .07)。PFS 的综合 HR 为 0.55(95% CI,0.41-0.74;P < .001),OS 为 0.76(95% CI,0.42-1.36;P = .20),有利于 HDT。Meta 回归显示,较长的随访时间与优越的 PFS(HR/mo,0.98;95% CI,0.96-0.99;P = .03)和 OS(HR/mo,0.90;95% CI,0.84-0.96)相关; P = .002)。对于 PFS,串联 HDT/ASCT 的 HR 最有利(0.49;95% CI,0.37-0.65),其次是单次 HDT/ASCT 联合硼替佐米、来那度胺和地塞米松(HR,0.53;95% CI,0.37-0.76)和单独的 HDT/ASCT (HR, 0.68; 95% CI, 0.53-0.87) 与 SDT 相比。对于 OS,没有一种基于 HDT/ASCT 的方法对生存率有显着影响。HDT/ASCT 治疗相关死亡率极低(<1%)。
结论和相关性 对所有 3 期 RCT 的常规荟萃分析和网络荟萃分析结果表明,与 SDT 相比,HDT/ASCT 与更高的 PFS 相关,且毒性作用最小。对于 PFS,串联 HDT/ASCT 和单次 HDT/ASCT 联合硼替佐米、来那度胺和地塞米松均优于单次 HDT/ASCT 和 SDT,但 4 种方法的 OS 相似。更长的随访时间可能更好地描述任何操作系统的好处;然而,可能会受到有效的复发后治疗的影响。










































 京公网安备 11010802027423号
京公网安备 11010802027423号