Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Association of Race and Ethnicity With Live Donor Kidney Transplantation in the United States From 1995 to 2014
JAMA ( IF 120.7 ) Pub Date : 2018-01-02 , DOI: 10.1001/jama.2017.19152 Tanjala S Purnell 1, 2, 3, 4 , Xun Luo 1 , Lisa A Cooper 2, 3, 4, 5 , Allan B Massie 1, 2 , Lauren M Kucirka 1, 2 , Macey L Henderson 1 , Elisa J Gordon 6 , Deidra C Crews 4, 7 , L Ebony Boulware 8 , Dorry L Segev 1, 2
JAMA ( IF 120.7 ) Pub Date : 2018-01-02 , DOI: 10.1001/jama.2017.19152 Tanjala S Purnell 1, 2, 3, 4 , Xun Luo 1 , Lisa A Cooper 2, 3, 4, 5 , Allan B Massie 1, 2 , Lauren M Kucirka 1, 2 , Macey L Henderson 1 , Elisa J Gordon 6 , Deidra C Crews 4, 7 , L Ebony Boulware 8 , Dorry L Segev 1, 2
Affiliation
|
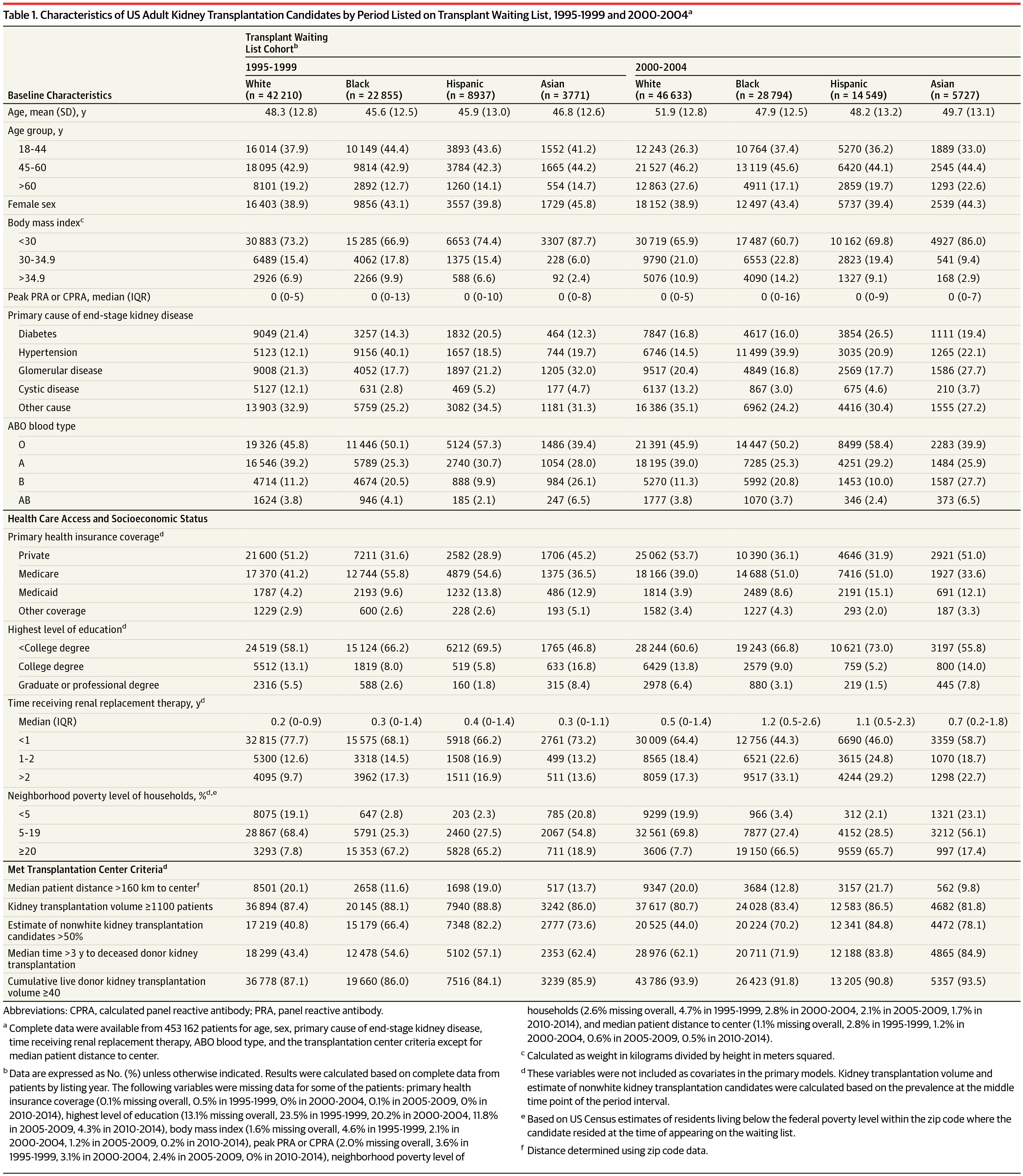
Importance Over the past 2 decades, there has been increased attention and effort to reduce disparities in live donor kidney transplantation (LDKT) for black, Hispanic, and Asian patients with end-stage kidney disease. The goal of this study was to investigate whether these efforts have been successful. Objective To estimate changes over time in racial/ethnic disparities in LDKT in the United States, accounting for differences in death and deceased donor kidney transplantation. Design, Setting, and Participants A secondary analysis of a prospectively maintained cohort study conducted in the United States of 453 162 adult first-time kidney transplantation candidates included in the Scientific Registry of Transplant Recipients between January 1, 1995, and December 31, 2014, with follow-up through December 31, 2016. Exposures Race/ethnicity. Main Outcomes and Measures The primary study outcome was time to LDKT. Multivariable Cox proportional hazards and competing risk models were constructed to assess changes in racial/ethnic disparities in LDKT among adults on the deceased donor kidney transplantation waiting list and interaction terms were used to test the statistical significance of temporal changes in racial/ethnic differences in receipt of LDKT. The adjusted subhazard ratios are estimates derived from the multivariable competing risk models. Data were categorized into 5-year increments (1995-1999, 2000-2004, 2005-2009, 2010-2014) to allow for an adequate sample size in each analytical cell. Results Among 453 162 adult kidney transplantation candidates (mean [SD] age, 50.9 [13.1] years; 39% were women; 48% were white; 30%, black; 16%, Hispanic; and 6%, Asian), 59 516 (13.1%) received LDKT. Overall, there were 39 509 LDKTs among white patients, 8926 among black patients, 8357 among Hispanic patients, and 2724 among Asian patients. In 1995, the cumulative incidence of LDKT at 2 years after appearing on the waiting list was 7.0% among white patients, 3.4% among black patients, 6.8% among Hispanic patients, and 5.1% among Asian patients. In 2014, the cumulative incidence of LDKT was 11.4% among white patients, 2.9% among black patients, 5.9% among Hispanic patients, and 5.6% among Asian patients. From 1995-1999 to 2010-2014, racial/ethnic disparities in the receipt of LDKT increased (P < .001 for all statistical interaction terms in adjusted models comparing white patients vs black, Hispanic, and Asian patients). In 1995-1999, compared with receipt of LDKT among white patients, the adjusted subhazard ratio was 0.45 (95% CI, 0.42-0.48) among black patients, 0.83 (95% CI, 0.77-0.88) among Hispanic patients, and 0.56 (95% CI, 0.50-0.63) among Asian patients. In 2010-2014, compared with receipt of LDKT among white patients, the adjusted subhazard ratio was 0.27 (95% CI, 0.26-0.28) among black patients, 0.52 (95% CI, 0.50-0.54) among Hispanic patients, and 0.42 (95% CI, 0.39-0.45) among Asian patients. Conclusions and Relevance Among adult first-time kidney transplantation candidates in the United States who were added to the deceased donor kidney transplantation waiting list between 1995 and 2014, disparities in the receipt of live donor kidney transplantation increased from 1995-1999 to 2010-2014. These findings suggest that national strategies for addressing disparities in receipt of live donor kidney transplantation should be revisited.
中文翻译:

1995 年至 2014 年美国活体肾移植的种族和民族关联
重要性 在过去的 20 年中,人们越来越关注和努力减少黑人、西班牙裔和亚洲终末期肾病患者活体肾移植 (LDKT) 的差异。本研究的目的是调查这些努力是否成功。目的 估计美国 LDKT 中种族/民族差异随时间的变化,考虑到死亡和已故供体肾移植的差异。设计、设置和参与者 对 1995 年 1 月 1 日至 2014 年 12 月 31 日期间在美国进行的 453 162 名成人首次肾移植候选者进行的前瞻性队列研究的二次分析,该研究纳入移植受者科学登记处,随访至 2016 年 12 月 31 日。暴露种族/民族。主要结果和测量 主要研究结果是 LDKT 时间。构建多变量 Cox 比例风险和竞争风险模型以评估已故供体肾移植等候名单上成年人 LDKT 种族/民族差异的变化,并使用交互项来测试接收中种族/民族差异的时间变化的统计显着性LDKT。调整后的子风险比是从多变量竞争风险模型中得出的估计值。数据按 5 年增量分类(1995-1999、2000-2004、2005-2009、2010-2014),以允许每个分析单元中有足够的样本量。结果 在 453 162 名成人肾移植候选者中(平均 [SD] 年龄,50.9 [13.1] 岁;39% 为女性;48% 为白人;30% 为黑人;16% 为西班牙裔;6% 为亚洲人),59 516 (13. 1%) 接受了 LDKT。总体而言,白人患者中有 39 509 例 LDKT,黑人患者中有 8926 例,西班牙裔患者中有 8357 例,亚裔患者中有 2724 例。1995年,在等待名单上出现2年后LDKT的累积发生率为白人7.0%,黑人3.4%,西班牙裔6.8%,亚裔5.1%。2014年LDKT的累积发病率为白人11.4%,黑人2.9%,西班牙裔5.9%,亚裔5.6%。从 1995-1999 年到 2010-2014 年,接受 LDKT 的种族/民族差异增加(在比较白人患者与黑人、西班牙裔和亚洲患者的调整模型中,所有统计交互项的 P < .001)。1995-1999 年,与白人患者接受 LDKT 相比,调整后的亚风险比为 0。黑人患者为 45 (95% CI, 0.42-0.48),西班牙裔患者为 0.83 (95% CI, 0.77-0.88),亚洲患者为 0.56 (95% CI, 0.50-0.63)。2010-2014 年,与白人患者接受 LDKT 相比,调整后的亚风险比在黑人患者中为 0.27(95% CI,0.26-0.28),在西班牙裔患者中为 0.52(95% CI,0.50-0.54),在西班牙裔患者中为 0.42( 95% CI,0.39-0.45)在亚洲患者中。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。48) 在黑人患者中,在西班牙裔患者中为 0.83 (95% CI, 0.77-0.88),在亚洲患者中为 0.56 (95% CI, 0.50-0.63)。2010-2014 年,与白人患者接受 LDKT 相比,调整后的亚风险比在黑人患者中为 0.27(95% CI,0.26-0.28),在西班牙裔患者中为 0.52(95% CI,0.50-0.54),在西班牙裔患者中为 0.42( 95% CI,0.39-0.45)在亚洲患者中。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。48) 在黑人患者中,在西班牙裔患者中为 0.83 (95% CI, 0.77-0.88),在亚洲患者中为 0.56 (95% CI, 0.50-0.63)。2010-2014 年,与白人患者接受 LDKT 相比,调整后的亚风险比在黑人患者中为 0.27(95% CI,0.26-0.28),在西班牙裔患者中为 0.52(95% CI,0.50-0.54),在西班牙裔患者中为 0.42( 95% CI,0.39-0.45)在亚洲患者中。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。西班牙裔患者为 77-0.88),亚洲患者为 0.56(95% CI,0.50-0.63)。2010-2014 年,与白人患者接受 LDKT 相比,调整后的亚风险比在黑人患者中为 0.27(95% CI,0.26-0.28),在西班牙裔患者中为 0.52(95% CI,0.50-0.54),在西班牙裔患者中为 0.42( 95% CI,0.39-0.45)在亚洲患者中。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。西班牙裔患者为 77-0.88),亚洲患者为 0.56(95% CI,0.50-0.63)。2010-2014 年,与白人患者接受 LDKT 相比,调整后的亚风险比在黑人患者中为 0.27(95% CI,0.26-0.28),在西班牙裔患者中为 0.52(95% CI,0.50-0.54),在西班牙裔患者中为 0.42( 95% CI,0.39-0.45)在亚洲患者中。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。2010-2014 年,与白人患者接受 LDKT 相比,调整后的亚风险比在黑人患者中为 0.27(95% CI,0.26-0.28),在西班牙裔患者中为 0.52(95% CI,0.50-0.54),在西班牙裔患者中为 0.42( 95% CI,0.39-0.45)在亚洲患者中。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。2010-2014 年,与白人患者接受 LDKT 相比,调整后的亚风险比在黑人患者中为 0.27(95% CI,0.26-0.28),在西班牙裔患者中为 0.52(95% CI,0.50-0.54),在西班牙裔患者中为 0.42( 95% CI,0.39-0.45)在亚洲患者中。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。西班牙裔患者为 50-0.54),亚洲患者为 0.42(95% CI,0.39-0.45)。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。西班牙裔患者为 50-0.54),亚洲患者为 0.42(95% CI,0.39-0.45)。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。从 1995-1999 年到 2010-2014 年,接受活体肾移植的差异有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。从 1995-1999 年到 2010-2014 年,接受活体肾移植的差异有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。
更新日期:2018-01-02
中文翻译:
1995 年至 2014 年美国活体肾移植的种族和民族关联
重要性 在过去的 20 年中,人们越来越关注和努力减少黑人、西班牙裔和亚洲终末期肾病患者活体肾移植 (LDKT) 的差异。本研究的目的是调查这些努力是否成功。目的 估计美国 LDKT 中种族/民族差异随时间的变化,考虑到死亡和已故供体肾移植的差异。设计、设置和参与者 对 1995 年 1 月 1 日至 2014 年 12 月 31 日期间在美国进行的 453 162 名成人首次肾移植候选者进行的前瞻性队列研究的二次分析,该研究纳入移植受者科学登记处,随访至 2016 年 12 月 31 日。暴露种族/民族。主要结果和测量 主要研究结果是 LDKT 时间。构建多变量 Cox 比例风险和竞争风险模型以评估已故供体肾移植等候名单上成年人 LDKT 种族/民族差异的变化,并使用交互项来测试接收中种族/民族差异的时间变化的统计显着性LDKT。调整后的子风险比是从多变量竞争风险模型中得出的估计值。数据按 5 年增量分类(1995-1999、2000-2004、2005-2009、2010-2014),以允许每个分析单元中有足够的样本量。结果 在 453 162 名成人肾移植候选者中(平均 [SD] 年龄,50.9 [13.1] 岁;39% 为女性;48% 为白人;30% 为黑人;16% 为西班牙裔;6% 为亚洲人),59 516 (13. 1%) 接受了 LDKT。总体而言,白人患者中有 39 509 例 LDKT,黑人患者中有 8926 例,西班牙裔患者中有 8357 例,亚裔患者中有 2724 例。1995年,在等待名单上出现2年后LDKT的累积发生率为白人7.0%,黑人3.4%,西班牙裔6.8%,亚裔5.1%。2014年LDKT的累积发病率为白人11.4%,黑人2.9%,西班牙裔5.9%,亚裔5.6%。从 1995-1999 年到 2010-2014 年,接受 LDKT 的种族/民族差异增加(在比较白人患者与黑人、西班牙裔和亚洲患者的调整模型中,所有统计交互项的 P < .001)。1995-1999 年,与白人患者接受 LDKT 相比,调整后的亚风险比为 0。黑人患者为 45 (95% CI, 0.42-0.48),西班牙裔患者为 0.83 (95% CI, 0.77-0.88),亚洲患者为 0.56 (95% CI, 0.50-0.63)。2010-2014 年,与白人患者接受 LDKT 相比,调整后的亚风险比在黑人患者中为 0.27(95% CI,0.26-0.28),在西班牙裔患者中为 0.52(95% CI,0.50-0.54),在西班牙裔患者中为 0.42( 95% CI,0.39-0.45)在亚洲患者中。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。48) 在黑人患者中,在西班牙裔患者中为 0.83 (95% CI, 0.77-0.88),在亚洲患者中为 0.56 (95% CI, 0.50-0.63)。2010-2014 年,与白人患者接受 LDKT 相比,调整后的亚风险比在黑人患者中为 0.27(95% CI,0.26-0.28),在西班牙裔患者中为 0.52(95% CI,0.50-0.54),在西班牙裔患者中为 0.42( 95% CI,0.39-0.45)在亚洲患者中。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。48) 在黑人患者中,在西班牙裔患者中为 0.83 (95% CI, 0.77-0.88),在亚洲患者中为 0.56 (95% CI, 0.50-0.63)。2010-2014 年,与白人患者接受 LDKT 相比,调整后的亚风险比在黑人患者中为 0.27(95% CI,0.26-0.28),在西班牙裔患者中为 0.52(95% CI,0.50-0.54),在西班牙裔患者中为 0.42( 95% CI,0.39-0.45)在亚洲患者中。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。西班牙裔患者为 77-0.88),亚洲患者为 0.56(95% CI,0.50-0.63)。2010-2014 年,与白人患者接受 LDKT 相比,调整后的亚风险比在黑人患者中为 0.27(95% CI,0.26-0.28),在西班牙裔患者中为 0.52(95% CI,0.50-0.54),在西班牙裔患者中为 0.42( 95% CI,0.39-0.45)在亚洲患者中。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。西班牙裔患者为 77-0.88),亚洲患者为 0.56(95% CI,0.50-0.63)。2010-2014 年,与白人患者接受 LDKT 相比,调整后的亚风险比在黑人患者中为 0.27(95% CI,0.26-0.28),在西班牙裔患者中为 0.52(95% CI,0.50-0.54),在西班牙裔患者中为 0.42( 95% CI,0.39-0.45)在亚洲患者中。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。2010-2014 年,与白人患者接受 LDKT 相比,调整后的亚风险比在黑人患者中为 0.27(95% CI,0.26-0.28),在西班牙裔患者中为 0.52(95% CI,0.50-0.54),在西班牙裔患者中为 0.42( 95% CI,0.39-0.45)在亚洲患者中。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。2010-2014 年,与白人患者接受 LDKT 相比,调整后的亚风险比在黑人患者中为 0.27(95% CI,0.26-0.28),在西班牙裔患者中为 0.52(95% CI,0.50-0.54),在西班牙裔患者中为 0.42( 95% CI,0.39-0.45)在亚洲患者中。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。西班牙裔患者为 50-0.54),亚洲患者为 0.42(95% CI,0.39-0.45)。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。西班牙裔患者为 50-0.54),亚洲患者为 0.42(95% CI,0.39-0.45)。结论和相关性 在 1995 年至 2014 年间被列入已故供体肾移植等候名单的美国成年首次肾移植候选者中,接受活体肾移植的差异从 1995 年至 1999 年至 2010 年至 2014 年期间有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。从 1995-1999 年到 2010-2014 年,接受活体肾移植的差异有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。从 1995-1999 年到 2010-2014 年,接受活体肾移植的差异有所增加。这些研究结果表明,应该重新审视解决接受活体肾移植的差异的国家战略。


























 京公网安备 11010802027423号
京公网安备 11010802027423号