当前位置:
X-MOL 学术
›
J. Hepatol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Impact of comorbidities on patient outcomes after interferon-free therapy-induced viral eradication in hepatitis C
Journal of Hepatology ( IF 26.8 ) Pub Date : 2018-05-01 , DOI: 10.1016/j.jhep.2017.12.019 Javier Ampuero , Carlota Jimeno , Rosa Quiles , José Miguel Rosales , Susana Llerena , Nieves Palomo , Patricia Cordero , Francisco Javier Serrano , Juan José Urquijo , José María Moreno-Planas , Guillermo Ontanilla , Marta Hernández , Aída Ortega-Alonso , Marta Maraver , Martín Bonacci , Ángela Rojas , Blanca Figueruela , Xavier Forns , Raúl J. Andrade , José Luis Calleja , Moisés Diago , Isabel Carmona , Manuel de la Mata , María Buti , Javier Crespo , Juan Manuel Pascasio , José María Navarro , Javier Salmerón , Manuel Romero-Gómez
Journal of Hepatology ( IF 26.8 ) Pub Date : 2018-05-01 , DOI: 10.1016/j.jhep.2017.12.019 Javier Ampuero , Carlota Jimeno , Rosa Quiles , José Miguel Rosales , Susana Llerena , Nieves Palomo , Patricia Cordero , Francisco Javier Serrano , Juan José Urquijo , José María Moreno-Planas , Guillermo Ontanilla , Marta Hernández , Aída Ortega-Alonso , Marta Maraver , Martín Bonacci , Ángela Rojas , Blanca Figueruela , Xavier Forns , Raúl J. Andrade , José Luis Calleja , Moisés Diago , Isabel Carmona , Manuel de la Mata , María Buti , Javier Crespo , Juan Manuel Pascasio , José María Navarro , Javier Salmerón , Manuel Romero-Gómez
|
BACKGROUND & AIMS
Patients with advanced liver fibrosis remain at risk of cirrhosis-related outcomes and those with severe comorbidities may not benefit from hepatitis C (HCV) eradication. We aimed to collect data on all-cause mortality and relevant clinical events within the first two years of direct-acting antiviral therapy, whilst determining the prognostic capability of a comorbidity-based model. METHODS
This was a prospective non-interventional study, from the beginning of direct-acting antiviral therapy to the event of interest (mortality) or up to two years of follow-up, including 14 Spanish University Hospitals. Patients with HCV infection, irrespective of liver fibrosis stage, who received direct-acting antiviral therapy were used to build an estimation and a validation cohort. Comorbidity was assessed according to Charlson comorbidity and CirCom indexes. RESULTS
A total of 3.4% (65/1,891) of individuals died within the first year, while 5.4% (102/1,891) died during the study. After adjusting for cirrhosis, platelet count, alanine aminotransferase and sex, the following factors were independently associated with one-year mortality: Charlson index (hazard ratio [HR] 1.55; 95% CI 1.29-1.86; p = 0.0001), bilirubin (HR 1.39; 95% CI 1.11-1.75; p = 0.004), age (HR 1.06 95% CI 1.02-1.11; p = 0.005), international normalized ratio (HR 3.49; 95% CI 1.36-8.97; p = 0.010), and albumin (HR 0.18; 95% CI 0.09-0.37; p = 0.0001). HepCom score showed a good calibration and discrimination (C-statistics 0.90), and was superior to the other prognostic scores (model for end-stage liver disease 0.81, Child-Pugh 0.72, CirCom 0.68) regarding one- and two-year mortality. HepCom score identified low- (≤5.7 points: 2%-3%) and high-risk (≥25 points: 56%-59%) mortality groups, both in the estimation and validation cohorts. The distribution of clinical events was similar between groups. CONCLUSIONS
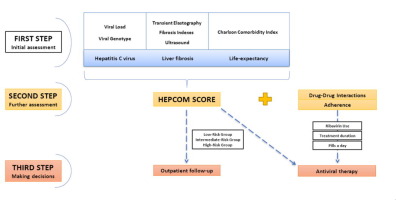
The HepCom score, a combination of Charlson comorbidity index, age, and liver function (international normalized ratio, albumin, and bilirubin) enables detection of a group at high risk of one- and two-year mortality, and relevant clinical events, after starting direct-acting antiviral therapy. LAY SUMMARY
The prognosis of patients with severe comorbidities may not benefit from HCV viral clearance. An algorithm to decide who will benefit from the treatment is needed to manage the chronic HCV infection better.
中文翻译:

无干扰素治疗诱导丙型肝炎病毒根除后合并症对患者预后的影响
背景和目的 晚期肝纤维化患者仍有发生肝硬化相关结局的风险,而那些有严重合并症的患者可能无法从丙型肝炎 (HCV) 根除中获益。我们的目标是在直接作用抗病毒治疗的前两年内收集全因死亡率和相关临床事件的数据,同时确定基于合并症的模型的预后能力。方法 这是一项前瞻性非干预性研究,从直接作用抗病毒治疗的开始到感兴趣的事件(死亡)或长达两年的随访,包括 14 家西班牙大学医院。无论肝纤维化阶段如何,接受直接抗病毒治疗的 HCV 感染患者被用于建立估计和验证队列。根据 Charlson 合并症和 CirCom 指数评估合并症。结果 共有 3.4% (65/1,891) 的个体在第一年内死亡,而 5.4% (102/1,891) 在研究期间死亡。在调整肝硬化、血小板计数、丙氨酸氨基转移酶和性别后,以下因素与一年死亡率独立相关:查尔森指数(风险比 [HR] 1.55;95% CI 1.29-1.86;p = 0.0001)、胆红素(HR 1.39;95% CI 1.11-1.75;p = 0.004),年龄(HR 1.06 95% CI 1.02-1.11;p = 0.005),国际标准化比率(HR 3.49;95% CI 1.36-8.97;p =)白蛋白(HR 0.18;95% CI 0.09-0.37;p = 0.0001)。HepCom 评分显示出良好的校准和辨别力(C 统计量为 0.90),并且优于其他预后评分(终末期肝病模型 0.81,Child-Pugh 0.72,CirCom 0. 68) 关于一年和两年的死亡率。HepCom 评分确定了估计和验证队列中的低(≤5.7 分:2%-3%)和高风险(≥25 分:56%-59%)死亡率组。组间临床事件的分布相似。结论 HepCom 评分是 Charlson 合并症指数、年龄和肝功能(国际标准化比值、白蛋白和胆红素)的组合,能够检测出一年和两年死亡率高风险组以及相关临床事件。开始直接作用抗病毒治疗。概述 有严重合并症的患者的预后可能不会从 HCV 病毒清除中受益。需要一种算法来决定谁将从治疗中受益,以更好地管理慢性 HCV 感染。2%-3%)和高风险(≥25 分:56%-59%)死亡率组,均在估计和验证队列中。组间临床事件的分布相似。结论 HepCom 评分是 Charlson 合并症指数、年龄和肝功能(国际标准化比值、白蛋白和胆红素)的组合,能够检测出一年和两年死亡率高风险组以及相关临床事件。开始直接作用抗病毒治疗。概述 有严重合并症的患者的预后可能不会从 HCV 病毒清除中受益。需要一种算法来决定谁将从治疗中受益,以更好地管理慢性 HCV 感染。2%-3%)和高风险(≥25 分:56%-59%)死亡率组,均在估计和验证队列中。组间临床事件的分布相似。结论 HepCom 评分是 Charlson 合并症指数、年龄和肝功能(国际标准化比值、白蛋白和胆红素)的组合,能够检测出一年和两年死亡率高风险组以及相关临床事件。开始直接作用抗病毒治疗。概述 有严重合并症的患者的预后可能不会从 HCV 病毒清除中受益。需要一种算法来决定谁将从治疗中受益,以更好地管理慢性 HCV 感染。组间临床事件的分布相似。结论 HepCom 评分是 Charlson 合并症指数、年龄和肝功能(国际标准化比值、白蛋白和胆红素)的组合,能够检测出一年和两年死亡率高风险组以及相关临床事件。开始直接作用抗病毒治疗。概述 有严重合并症的患者的预后可能不会从 HCV 病毒清除中受益。需要一种算法来决定谁将从治疗中受益,以更好地管理慢性 HCV 感染。组间临床事件的分布相似。结论 HepCom 评分是 Charlson 合并症指数、年龄和肝功能(国际标准化比值、白蛋白和胆红素)的组合,能够检测出一年和两年死亡率高风险组以及相关临床事件。开始直接作用抗病毒治疗。概述 有严重合并症的患者的预后可能不会从 HCV 病毒清除中受益。需要一种算法来决定谁将从治疗中受益,以更好地管理慢性 HCV 感染。开始直接抗病毒治疗后。概述 有严重合并症的患者的预后可能不会从 HCV 病毒清除中受益。需要一种算法来决定谁将从治疗中受益,以更好地管理慢性 HCV 感染。开始直接抗病毒治疗后。概述 有严重合并症的患者的预后可能不会从 HCV 病毒清除中受益。需要一种算法来决定谁将从治疗中受益,以更好地管理慢性 HCV 感染。
更新日期:2018-05-01
中文翻译:
无干扰素治疗诱导丙型肝炎病毒根除后合并症对患者预后的影响
背景和目的 晚期肝纤维化患者仍有发生肝硬化相关结局的风险,而那些有严重合并症的患者可能无法从丙型肝炎 (HCV) 根除中获益。我们的目标是在直接作用抗病毒治疗的前两年内收集全因死亡率和相关临床事件的数据,同时确定基于合并症的模型的预后能力。方法 这是一项前瞻性非干预性研究,从直接作用抗病毒治疗的开始到感兴趣的事件(死亡)或长达两年的随访,包括 14 家西班牙大学医院。无论肝纤维化阶段如何,接受直接抗病毒治疗的 HCV 感染患者被用于建立估计和验证队列。根据 Charlson 合并症和 CirCom 指数评估合并症。结果 共有 3.4% (65/1,891) 的个体在第一年内死亡,而 5.4% (102/1,891) 在研究期间死亡。在调整肝硬化、血小板计数、丙氨酸氨基转移酶和性别后,以下因素与一年死亡率独立相关:查尔森指数(风险比 [HR] 1.55;95% CI 1.29-1.86;p = 0.0001)、胆红素(HR 1.39;95% CI 1.11-1.75;p = 0.004),年龄(HR 1.06 95% CI 1.02-1.11;p = 0.005),国际标准化比率(HR 3.49;95% CI 1.36-8.97;p =)白蛋白(HR 0.18;95% CI 0.09-0.37;p = 0.0001)。HepCom 评分显示出良好的校准和辨别力(C 统计量为 0.90),并且优于其他预后评分(终末期肝病模型 0.81,Child-Pugh 0.72,CirCom 0. 68) 关于一年和两年的死亡率。HepCom 评分确定了估计和验证队列中的低(≤5.7 分:2%-3%)和高风险(≥25 分:56%-59%)死亡率组。组间临床事件的分布相似。结论 HepCom 评分是 Charlson 合并症指数、年龄和肝功能(国际标准化比值、白蛋白和胆红素)的组合,能够检测出一年和两年死亡率高风险组以及相关临床事件。开始直接作用抗病毒治疗。概述 有严重合并症的患者的预后可能不会从 HCV 病毒清除中受益。需要一种算法来决定谁将从治疗中受益,以更好地管理慢性 HCV 感染。2%-3%)和高风险(≥25 分:56%-59%)死亡率组,均在估计和验证队列中。组间临床事件的分布相似。结论 HepCom 评分是 Charlson 合并症指数、年龄和肝功能(国际标准化比值、白蛋白和胆红素)的组合,能够检测出一年和两年死亡率高风险组以及相关临床事件。开始直接作用抗病毒治疗。概述 有严重合并症的患者的预后可能不会从 HCV 病毒清除中受益。需要一种算法来决定谁将从治疗中受益,以更好地管理慢性 HCV 感染。2%-3%)和高风险(≥25 分:56%-59%)死亡率组,均在估计和验证队列中。组间临床事件的分布相似。结论 HepCom 评分是 Charlson 合并症指数、年龄和肝功能(国际标准化比值、白蛋白和胆红素)的组合,能够检测出一年和两年死亡率高风险组以及相关临床事件。开始直接作用抗病毒治疗。概述 有严重合并症的患者的预后可能不会从 HCV 病毒清除中受益。需要一种算法来决定谁将从治疗中受益,以更好地管理慢性 HCV 感染。组间临床事件的分布相似。结论 HepCom 评分是 Charlson 合并症指数、年龄和肝功能(国际标准化比值、白蛋白和胆红素)的组合,能够检测出一年和两年死亡率高风险组以及相关临床事件。开始直接作用抗病毒治疗。概述 有严重合并症的患者的预后可能不会从 HCV 病毒清除中受益。需要一种算法来决定谁将从治疗中受益,以更好地管理慢性 HCV 感染。组间临床事件的分布相似。结论 HepCom 评分是 Charlson 合并症指数、年龄和肝功能(国际标准化比值、白蛋白和胆红素)的组合,能够检测出一年和两年死亡率高风险组以及相关临床事件。开始直接作用抗病毒治疗。概述 有严重合并症的患者的预后可能不会从 HCV 病毒清除中受益。需要一种算法来决定谁将从治疗中受益,以更好地管理慢性 HCV 感染。开始直接抗病毒治疗后。概述 有严重合并症的患者的预后可能不会从 HCV 病毒清除中受益。需要一种算法来决定谁将从治疗中受益,以更好地管理慢性 HCV 感染。开始直接抗病毒治疗后。概述 有严重合并症的患者的预后可能不会从 HCV 病毒清除中受益。需要一种算法来决定谁将从治疗中受益,以更好地管理慢性 HCV 感染。










































 京公网安备 11010802027423号
京公网安备 11010802027423号