The Lancet Diabetes & Endocrinology ( IF 44.0 ) Pub Date : 2017-09-15 , DOI: 10.1016/s2213-8587(17)30313-3 Marc S Sabatine , Lawrence A Leiter , Stephen D Wiviott , Robert P Giugliano , Prakash Deedwania , Gaetano M De Ferrari , Sabina A Murphy , Julia F Kuder , Ioanna Gouni-Berthold , Basil S Lewis , Yehuda Handelsman , Armando Lira Pineda , Narimon Honarpour , Anthony C Keech , Peter S Sever , Terje R Pedersen
|
Background
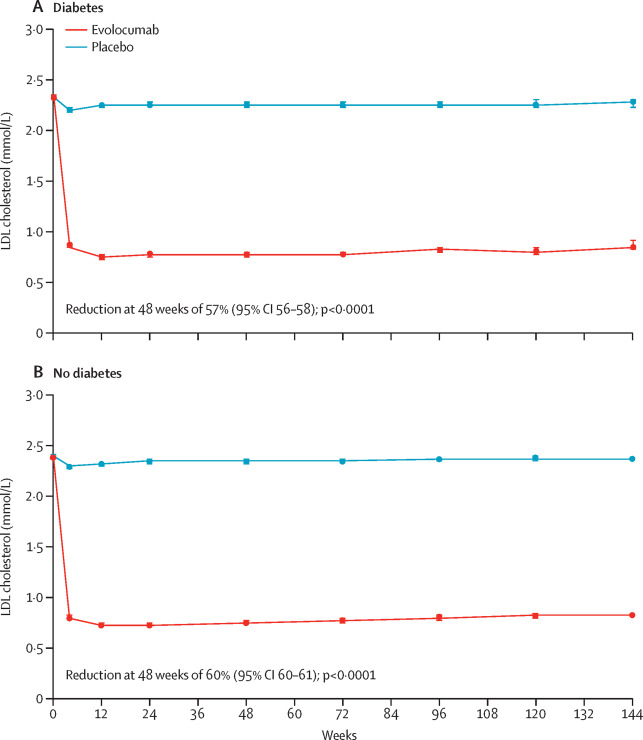
The proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor evolocumab reduced LDL cholesterol and cardiovascular events in the FOURIER trial. In this prespecified analysis of FOURIER, we investigated the efficacy and safety of evolocumab by diabetes status and the effect of evolocumab on glycaemia and risk of developing diabetes.
Methods
FOURIER was a randomised trial of evolocumab (140 mg every 2 weeks or 420 mg once per month) versus placebo in 27 564 patients with atherosclerotic disease who were on statin therapy, followed up for a median of 2·2 years. In this prespecified analysis, we investigated the effect of evolocumab on cardiovascular events by diabetes status at baseline, defined on the basis of patient history, clinical events committee review of medical records, or baseline HbA1c of 6·5% (48 mmol/mol) or greater or fasting plasma glucose (FPG) of 7·0 mmol/L or greater. The primary endpoint was a composite of cardiovascular death, myocardial infarction, stroke, hospital admission for unstable angina, or coronary revascularisation. The key secondary endpoint was a composite of cardiovascular death, myocardial infarction, or stroke. We also assessed the effect of evolocumab on glycaemia, and on the risk of new-onset diabetes among patients without diabetes at baseline. HbA1c was measured at baseline then every 24 weeks and FPG was measured at baseline, week 12, week 24, and every 24 weeks thereafter, and potential cases of new-onset diabetes were adjudicated centrally. In a post-hoc analysis, we also investigated the effects on glycaemia and diabetes risk in patients with prediabetes (HbA1c 5·7–6·4% [39–46 mmol/mol] or FPG 5·6–6·9 mmol/L) at baseline. FOURIER is registered with ClinicalTrials.gov, number NCT01764633.
Findings
At study baseline, 11 031 patients (40%) had diabetes and 16 533 (60%) did not have diabetes (of whom 10 344 had prediabetes and 6189 had normoglycaemia). Evolocumab significantly reduced cardiovascular outcomes consistently in patients with and without diabetes at baseline. For the primary composite endpoint, the hazard ratios (HRs) were 0·83 (95% CI 0·75–0·93; p=0·0008) for patients with diabetes and 0·87 (0·79–0·96; p=0·0052) for patients without diabetes (pinteraction=0·60). For the key secondary endpoint, the HRs were 0·82 (0·72–0·93; p=0·0021) for those with diabetes and 0·78 (0·69–0·89; p=0·0002) for those without diabetes (pinteraction=0·65). Evolocumab did not increase the risk of new-onset diabetes in patients without diabetes at baseline (HR 1·05, 0·94–1·17), including in those with prediabetes (HR 1·00, 0·89–1·13). Levels of HbA1c and FPG were similar between the evolocumab and placebo groups over time in patients with diabetes, prediabetes, or normoglycaemia. Among patients with diabetes at baseline, the proportions of patients with adverse events were 78·5% (4327 of 5513 patients) in the evolocumab group and 78·3% (4307 of 5502 patients) in the placebo group; among patients without diabetes at baseline, the proportions with adverse events were 76·8% (6337 of 8256 patients) in the evolocumab group and 76·8% (6337 of 8254 patients) in the placebo group.
Interpretation
PCSK9 inhibition with evolocumab significantly reduced cardiovascular risk in patients with and without diabetes. Evolocumab did not increase the risk of new-onset diabetes, nor did it worsen glycaemia. These data suggest evolocumab use in patients with atherosclerotic disease is efficacious and safe in patients with and without diabetes.
Funding
Amgen.
中文翻译:
PCSK9抑制剂evolocumab在有糖尿病和无糖尿病患者中的心血管安全性和有效性,以及evolocumab对血糖和新发糖尿病风险的影响:FOURIER随机对照试验的预先分析
背景
在FOURIER试验中,前蛋白转化酶枯草杆菌蛋白酶/ kexin 9型(PCSK9)抑制剂evolocumab降低了LDL胆固醇和心血管事件。在此预先确定的FOURIER分析中,我们通过糖尿病状况调查了依维洛单抗的疗效和安全性,以及依维洛单抗对血糖和糖尿病风险的影响。
方法
FOURIER是在接受他汀类药物治疗的27 564例动脉粥样硬化性疾病患者中,对evolocumab(每2周140 mg或每月一次420 mg)与安慰剂进行的随机试验,平均随访2·2年。在这项预先设定的分析中,我们调查了依洛伐单抗在基线时的糖尿病状态(根据患者病史,临床事件委员会对病历的审查或基线HbA 1c的定义)对心血管事件的影响。≥6·5%(48 mmol / mol)或空腹血浆葡萄糖(FPG)≥7·0 mmol / L。主要终点指标是心血管死亡,心肌梗塞,中风,因不稳定型心绞痛住院或冠状动脉血运重建的综合因素。关键的次要终点是心血管死亡,心肌梗塞或中风的综合症状。我们还评估了基线时无糖尿病患者中依维洛单抗对血糖和新发糖尿病风险的影响。血红蛋白1c在基线时进行测量,然后每24周测量一次,在基线时,第12周,第24周以及此后的每24周测量FPG,并对潜在的新发糖尿病病例进行集中裁决。在事后分析中,我们还研究了对糖尿病前期患者(HbA 1c 5·7–6·4%[39–46 mmol / mol]或FPG 5·6–6·9 mmol)对血糖和糖尿病风险的影响/ L)。FOURIER已在ClinicalTrials.gov上注册,编号为NCT01764633。
发现
在研究基线时,有11031名患者(40%)患有糖尿病,而16533名患者(60%)没有糖尿病(其中10344名患有糖尿病前期,6189名患有血糖正常)。在基线时有或没有糖尿病的患者,依伏洛单抗均能显着降低心血管结局。对于主要的复合终点,糖尿病患者的危险比(HRs)为0·83(95%CI 0·75-0·93; p = 0·0008)和0·87(0·79-0·96) ; p = 0·0052)对于没有糖尿病的患者(p交互作用= 0·60)。对于关键的次要终点,糖尿病患者的HRs为0·82(0·72-0·93; p = 0·0021),糖尿病患者的HRs为0·78(0·69-0·89; p = 0·0002)。对于没有糖尿病的患者(p交互作用= 0·65)。基线时无糖尿病患者(HR 1·05,0·94-1·17),包括糖尿病前期患者(HR 1·00,0·89-1·13),依夫洛单抗并没有增加新发糖尿病的风险)。随着时间的流逝,糖尿病,糖尿病前期或正常血糖患者的evolocumab组和安慰剂组之间的HbA 1c和FPG水平相似。在基线期糖尿病患者中,依维洛单抗组有不良事件的患者比例为78·5%(5513例患者中的4327例),而安慰剂组为78·3%(5502例患者中的4307例);在基线时无糖尿病的患者中,evolocumab组发生不良事件的比例为76.8%(8256例患者中的6337例),而安慰剂组为76.8%(8254例患者中的6337例)。
解释
evolocumab对PCSK9的抑制作用可显着降低患有和不患有糖尿病的患者的心血管风险。Evolocumab不会增加新发糖尿病的风险,也不会加重血糖。这些数据表明,在患有和没有糖尿病的患者中,将evolocumab用于动脉粥样硬化疾病是有效且安全的。
资金
安进










































 京公网安备 11010802027423号
京公网安备 11010802027423号