JACC: Cardiovascular Imaging ( IF 12.8 ) Pub Date : 2018-12-01 , DOI: 10.1016/j.jcmg.2017.09.003 Joshua D. Mitchell , Robert Paisley , Patrick Moon , Eric Novak , Todd C. Villines
|
Objectives This study aimed to assess the long-term risk of death and atherosclerotic cardiovascular disease (ASCVD) outcomes, including stroke, in a real-world cohort that underwent coronary artery calcium (CAC) scoring.
Background Large-scale, long-term studies assessing the independent relationship of CAC for prediction of ASCVD events, to include stroke, in young, low-risk patients are uncommon outside of the clinical trial setting.
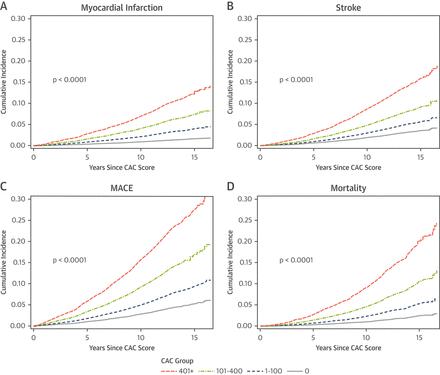
Methods A total of 23,637 consecutive subjects without ASCVD who underwent CAC scoring from 1997 to 2009 were studied. Subjects were assessed for myocardial infarction (MI), stroke, major adverse cardiovascular events (MACE) (e.g., MI, stroke, or cardiovascular death), and all-cause mortality. Outcomes were extracted from the Military Data Repository and the National Death Index and assessed using Cox proportional hazards models, controlling for baseline risk factors, atrial fibrillation, and competing mortality.
Results Patients (mean age 50.0 ± 8.5 years) were followed over a median of 11.4 years. The relative adjusted subhazard ratio (aSHR) for CAC 1 to 100, 101 to 400, and >400 was 2.2, 3.8, and 5.9 for MI; 1.2, 1.4, and 1.9 for stroke; 1.4, 2.0, and 2.8 for MACE; and 1.2, 1.5 and 2.1 for death (p < 0.0001). The addition of CAC score to risk factors significantly improved the prognostic accuracy for all outcomes by the likelihood ratio test. Area under the curve increased from 0.658 to 0.738 for MI, 0.703 to 0.704 for stroke, 0.685 to 0.705 for MACE, and 0.759 to 0.767 for mortality. Among subjects without traditional risk factors (n = 6,208; mean age 43.8 ± 4.4 years), the presence of any CAC (>0; n = 848) was associated with an increased risk of MACE (aSHR: 1.67; 95% confidence interval: 1.16 to 2.39).
Conclusions CAC scoring significantly improved long-term prognostic accuracy for MACE events and mortality, irrespective of age and risk factors. These results support CAC screening for improving individual ASCVD risk assessment and prevention in low-risk, young adults.
中文翻译:
目的本研究旨在评估在接受冠状动脉钙(CAC)评分的真实队列中,包括卒中在内的长期死亡和动脉粥样硬化性心血管疾病(ASCVD)结果的长期风险。
背景技术大规模,长期研究评估了CAC预测ASCVD事件(包括中风)在年轻,低风险患者中的独立关系,这在临床试验范围之外并不常见。
方法对1997年至2009年连续23637例无ASCVD的连续受试者进行CAC评分。对受试者进行了心肌梗塞(MI),中风,主要不良心血管事件(MACE)(例如MI,中风或心血管死亡)和全因死亡率的评估。从军事数据存储库和国家死亡指数中提取结果,并使用Cox比例风险模型进行评估,以控制基线风险因素,心房颤动和竞争性死亡率。
结果随访患者(平均年龄50.0±8.5岁),中位时间为11.4年。CAC 1比100、101比400和> 400的相对调整后亚危险比(aSHR)对于MI分别为2.2、3.8和5.9;中风的1.2、1.4和1.9; 适用于MACE的1.4、2.0和2.8;以及死亡的1.2、1.5和2.1(p <0.0001)。通过可能性比检验,将CAC评分添加到危险因素中可显着提高所有结局的预后准确性。MI曲线下面积从0.658增至0.738,中风从0.703增至0.704,MACE从0.685增至0.705,死亡率从0.759增至0.767。在没有传统危险因素的受试者中(n = 6,208;平均年龄43.8±4.4岁),任何CAC的存在(> 0; n = 848)与MACE风险增加相关(aSHR:1.67; 95%置信区间: 1.16至2.39)。
结论CAC评分显着提高了MACE事件和死亡率的长期预后准确性,而不受年龄和危险因素的影响。这些结果支持CAC筛查,以改善低风险,年轻成年人的个体ASCVD风险评估和预防。










































 京公网安备 11010802027423号
京公网安备 11010802027423号