Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Does This Patient Have Acute Mountain Sickness?
JAMA ( IF 63.1 ) Pub Date : 2017-11-14 , DOI: 10.1001/jama.2017.16192 David Meier 1 , Tinh-Hai Collet 2, 3 , Isabella Locatelli 3 , Jacques Cornuz 3 , Bengt Kayser 4 , David L. Simel 5, 6 , Claudio Sartori 1
JAMA ( IF 63.1 ) Pub Date : 2017-11-14 , DOI: 10.1001/jama.2017.16192 David Meier 1 , Tinh-Hai Collet 2, 3 , Isabella Locatelli 3 , Jacques Cornuz 3 , Bengt Kayser 4 , David L. Simel 5, 6 , Claudio Sartori 1
Affiliation
|
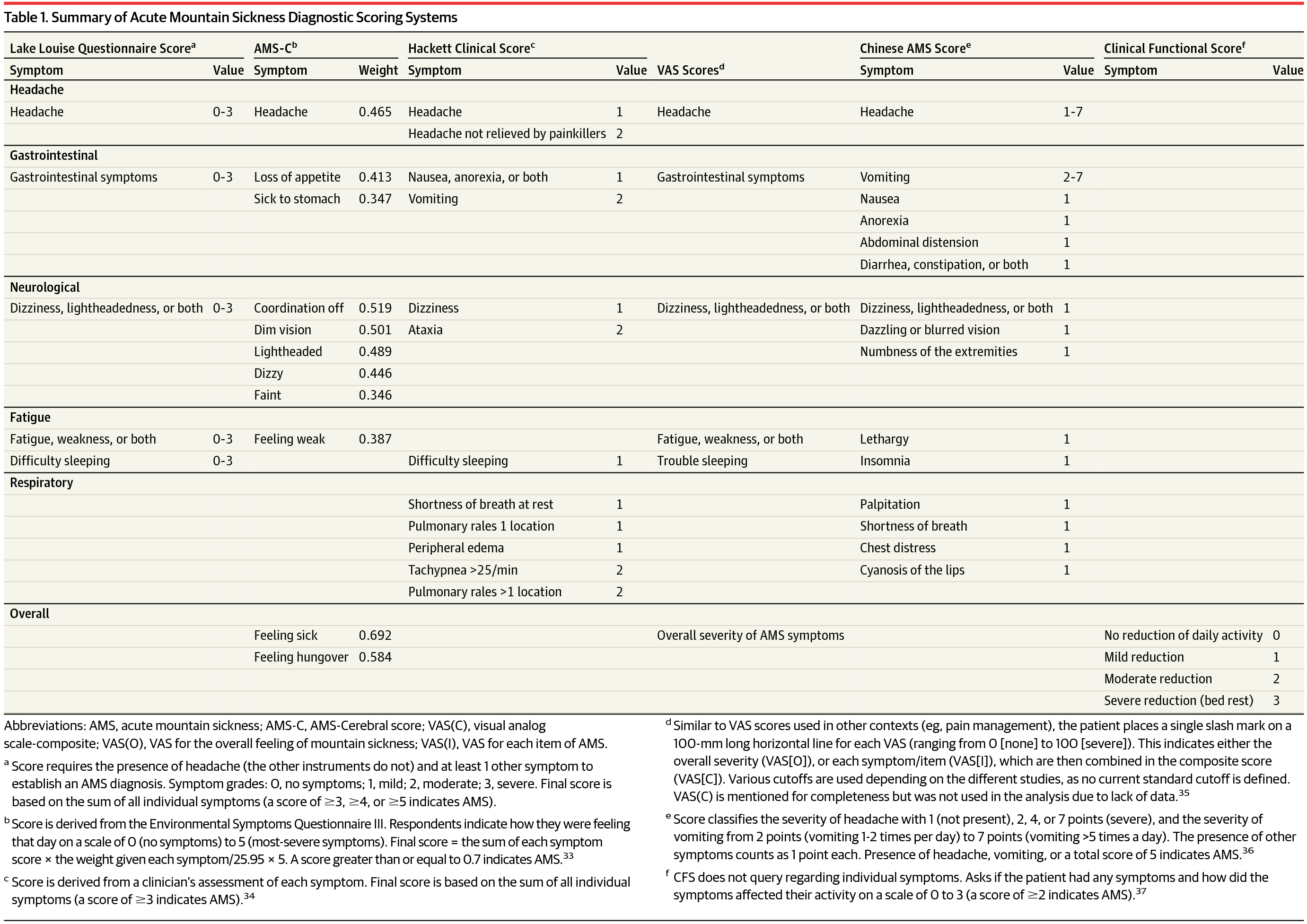
Importance Acute mountain sickness (AMS) affects more than 25% of individuals ascending to 3500 m (11 500 ft) and more than 50% of those above 6000 m (19 700 ft). AMS may progress from nonspecific symptoms to life-threatening high-altitude cerebral edema in less than 1% of patients. It is not clear how to best diagnose AMS. Objective To systematically review studies assessing the accuracy of AMS diagnostic instruments, including the visual analog scale (VAS) score, which quantifies the overall feeling of sickness at altitude (VAS[O]; various thresholds), Acute Mountain Sickness-Cerebral score (AMS-C; ≥0.7 indicates AMS), and the clinical functional score (CFS; ≥2 indicates AMS) compared with the Lake Louise Questionnaire Score (LLQS; score of ≥5). Data Extraction and Synthesis Searches of MEDLINE and EMBASE from inception to May 2017 identified 1245 publications of which 91 were suitable for prevalence analysis (66 944 participants) and 14 compared at least 2 instruments (1858 participants) using a score of 5 or greater on the LLQS as a reference standard. To determine the prevalence of AMS for establishing the pretest probability of AMS, a random-effects meta-regression was performed based on the reported prevalence of AMS as a function of altitude. Main Outcomes and Measures AMS prevalence, likelihood ratios (LRs), sensitivity, and specificity of screening instruments. Results The final analysis included 91 articles (comprising 66 944 study participants). Altitude predicted AMS and accounted for 28% of heterogeneity between studies. For each 1000-m (3300-ft) increase in altitude above 2500 m (8200 ft), AMS prevalence increased 13% (95% CI, 9.5%-17%). Testing characteristics were similar for VAS(O), AMS-C, and CFS vs a score of 5 or greater on the LLQS (positive LRs: range, 3.2-8.2; P = .22 for comparisons; specificity range, 67%-92%; negative LRs: range, 0.30-0.36; P = .50 for comparisons; sensitivity range, 67%-82%). The CFS asks a single question: “overall if you had any symptoms, how did they affect your activity (ordinal scale 0-3)?” For CFS, moderate to severe reduction in daily activities had a positive LR of 3.2 (95% CI, 1.4-7.2) and specificity of 67% (95% CI, 37%-97%); no reduction to mild reduction in activities had a negative LR of 0.30 (95% CI, 0.22-0.39) and sensitivity of 82% (95% CI, 77%-87%). Conclusions and Relevance The prevalence of acute mountain sickness increases with higher altitudes. The visual analog scale for the overall feeling of sickness at altitude, Acute Mountain Sickness-Cerebral, and clinical functional score perform similarly to the Lake Louise Questionnaire Score using a score of 5 or greater as a reference standard. In clinical and travel settings, the clinical functional score is the simplest instrument to use. Clinicians evaluating high-altitude travelers who report moderate to severe limitations in activities of daily living (clinical functional score ≥2) should use the Lake Louise Questionnaire Score to assess the severity of acute mountain sickness.
中文翻译:

这个病人有急性高山病吗?
重要性 急性高山病 (AMS) 影响超过 25% 的上升到 3500 m (11 500 ft) 的人和超过 50% 的 6000 m (19 700 ft) 以上的人。不到 1% 的 AMS 患者可能会从非特异性症状发展为危及生命的高原脑水肿。目前尚不清楚如何最好地诊断 AMS。目的 系统回顾评估 AMS 诊断工具准确性的研究,包括视觉模拟量表 (VAS) 评分,该评分可量化高海拔地区的整体不适感 (VAS[O];各种阈值)、急性高山病脑评分 (AMS) -C;≥0.7 表示 AMS),临床功能评分(CFS;≥2 表示 AMS)与路易斯湖问卷评分(LLQS;评分≥5)相比。从成立到 2017 年 5 月,MEDLINE 和 EMBASE 的数据提取和综合搜索确定了 1245 篇出版物,其中 91 篇适合流行率分析(66944 名参与者),14 篇使用 5 分或更高的分数比较了至少 2 种工具(1858 名参与者) LLQS 作为参考标准。为了确定 AMS 的患病率以建立 AMS 的前测概率,基于报告的 AMS 患病率作为海拔的函数进行了随机效应元回归。主要结果和测量 AMS 患病率、似然比 (LR)、筛查工具的敏感性和特异性。结果 最终分析包括 91 篇文章(包括 66 944 名研究参与者)。海拔高度预测了 AMS,占研究间异质性的 28%。在海拔 2500 米(8200 英尺)以上每增加 1000 米(3300 英尺),AMS 患病率就会增加 13%(95% CI,9.5%-17%)。VAS(O)、AMS-C 和 CFS 的测试特征与 LLQS 5 分或更高的测试特征相似(阳性 LR:范围,3.2-8.2;用于比较的 P = .22;特异性范围,67%-92 %;负 LR:范围,0.30-0.36;用于比较的 P = .50;灵敏度范围,67%-82%)。CFS 只问了一个问题:“总体而言,如果您有任何症状,它们对您的活动有何影响(顺序量表 0-3)?” 对于 CFS,中度至重度日常活动减少的阳性 LR 为 3.2(95% CI,1.4-7.2),特异性为 67%(95% CI,37%-97%);活动没有减少到轻度减少的负 LR 为 0.30(95% CI,0.22-0.39),敏感性为 82%(95% CI,77%-87%)。结论和相关性 急性高山病的患病率随海拔升高而增加。高海拔地区整体疾病感觉、急性高山病脑病和临床功能评分的视觉模拟量表与路易斯湖问卷评分类似,使用 5 分或更高作为参考标准。在临床和旅行环境中,临床功能评分是最简单的工具。评估高海拔旅行者报告日常生活活动中度至重度受限(临床功能评分≥2)的临床医生应使用路易斯湖问卷评分来评估急性高山病的严重程度。和临床功能评分的表现类似于路易斯湖问卷评分,使用 5 分或更高的评分作为参考标准。在临床和旅行环境中,临床功能评分是最简单的工具。评估高海拔旅行者报告日常生活活动中度至重度受限(临床功能评分≥2)的临床医生应使用路易斯湖问卷评分来评估急性高山病的严重程度。和临床功能评分的表现类似于路易斯湖问卷评分,使用 5 分或更高的评分作为参考标准。在临床和旅行环境中,临床功能评分是最简单的工具。评估高海拔旅行者报告日常生活活动中度至重度受限(临床功能评分≥2)的临床医生应使用路易斯湖问卷评分来评估急性高山病的严重程度。
更新日期:2017-11-14
中文翻译:
这个病人有急性高山病吗?
重要性 急性高山病 (AMS) 影响超过 25% 的上升到 3500 m (11 500 ft) 的人和超过 50% 的 6000 m (19 700 ft) 以上的人。不到 1% 的 AMS 患者可能会从非特异性症状发展为危及生命的高原脑水肿。目前尚不清楚如何最好地诊断 AMS。目的 系统回顾评估 AMS 诊断工具准确性的研究,包括视觉模拟量表 (VAS) 评分,该评分可量化高海拔地区的整体不适感 (VAS[O];各种阈值)、急性高山病脑评分 (AMS) -C;≥0.7 表示 AMS),临床功能评分(CFS;≥2 表示 AMS)与路易斯湖问卷评分(LLQS;评分≥5)相比。从成立到 2017 年 5 月,MEDLINE 和 EMBASE 的数据提取和综合搜索确定了 1245 篇出版物,其中 91 篇适合流行率分析(66944 名参与者),14 篇使用 5 分或更高的分数比较了至少 2 种工具(1858 名参与者) LLQS 作为参考标准。为了确定 AMS 的患病率以建立 AMS 的前测概率,基于报告的 AMS 患病率作为海拔的函数进行了随机效应元回归。主要结果和测量 AMS 患病率、似然比 (LR)、筛查工具的敏感性和特异性。结果 最终分析包括 91 篇文章(包括 66 944 名研究参与者)。海拔高度预测了 AMS,占研究间异质性的 28%。在海拔 2500 米(8200 英尺)以上每增加 1000 米(3300 英尺),AMS 患病率就会增加 13%(95% CI,9.5%-17%)。VAS(O)、AMS-C 和 CFS 的测试特征与 LLQS 5 分或更高的测试特征相似(阳性 LR:范围,3.2-8.2;用于比较的 P = .22;特异性范围,67%-92 %;负 LR:范围,0.30-0.36;用于比较的 P = .50;灵敏度范围,67%-82%)。CFS 只问了一个问题:“总体而言,如果您有任何症状,它们对您的活动有何影响(顺序量表 0-3)?” 对于 CFS,中度至重度日常活动减少的阳性 LR 为 3.2(95% CI,1.4-7.2),特异性为 67%(95% CI,37%-97%);活动没有减少到轻度减少的负 LR 为 0.30(95% CI,0.22-0.39),敏感性为 82%(95% CI,77%-87%)。结论和相关性 急性高山病的患病率随海拔升高而增加。高海拔地区整体疾病感觉、急性高山病脑病和临床功能评分的视觉模拟量表与路易斯湖问卷评分类似,使用 5 分或更高作为参考标准。在临床和旅行环境中,临床功能评分是最简单的工具。评估高海拔旅行者报告日常生活活动中度至重度受限(临床功能评分≥2)的临床医生应使用路易斯湖问卷评分来评估急性高山病的严重程度。和临床功能评分的表现类似于路易斯湖问卷评分,使用 5 分或更高的评分作为参考标准。在临床和旅行环境中,临床功能评分是最简单的工具。评估高海拔旅行者报告日常生活活动中度至重度受限(临床功能评分≥2)的临床医生应使用路易斯湖问卷评分来评估急性高山病的严重程度。和临床功能评分的表现类似于路易斯湖问卷评分,使用 5 分或更高的评分作为参考标准。在临床和旅行环境中,临床功能评分是最简单的工具。评估高海拔旅行者报告日常生活活动中度至重度受限(临床功能评分≥2)的临床医生应使用路易斯湖问卷评分来评估急性高山病的严重程度。










































 京公网安备 11010802027423号
京公网安备 11010802027423号