Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Derivation and External Validation of Prediction Models for Advanced Chronic Kidney Disease Following Acute Kidney Injury
JAMA ( IF 63.1 ) Pub Date : 2017-11-14 , DOI: 10.1001/jama.2017.16326 Matthew T. James 1 , Neesh Pannu 2 , Brenda R. Hemmelgarn 1 , Peter C. Austin 3 , Zhi Tan 4 , Eric McArthur 5 , Braden J. Manns 1 , Marcello Tonelli 1 , Ron Wald 6 , Robert R. Quinn 1 , Pietro Ravani 1 , Amit X. Garg 7
JAMA ( IF 63.1 ) Pub Date : 2017-11-14 , DOI: 10.1001/jama.2017.16326 Matthew T. James 1 , Neesh Pannu 2 , Brenda R. Hemmelgarn 1 , Peter C. Austin 3 , Zhi Tan 4 , Eric McArthur 5 , Braden J. Manns 1 , Marcello Tonelli 1 , Ron Wald 6 , Robert R. Quinn 1 , Pietro Ravani 1 , Amit X. Garg 7
Affiliation
|
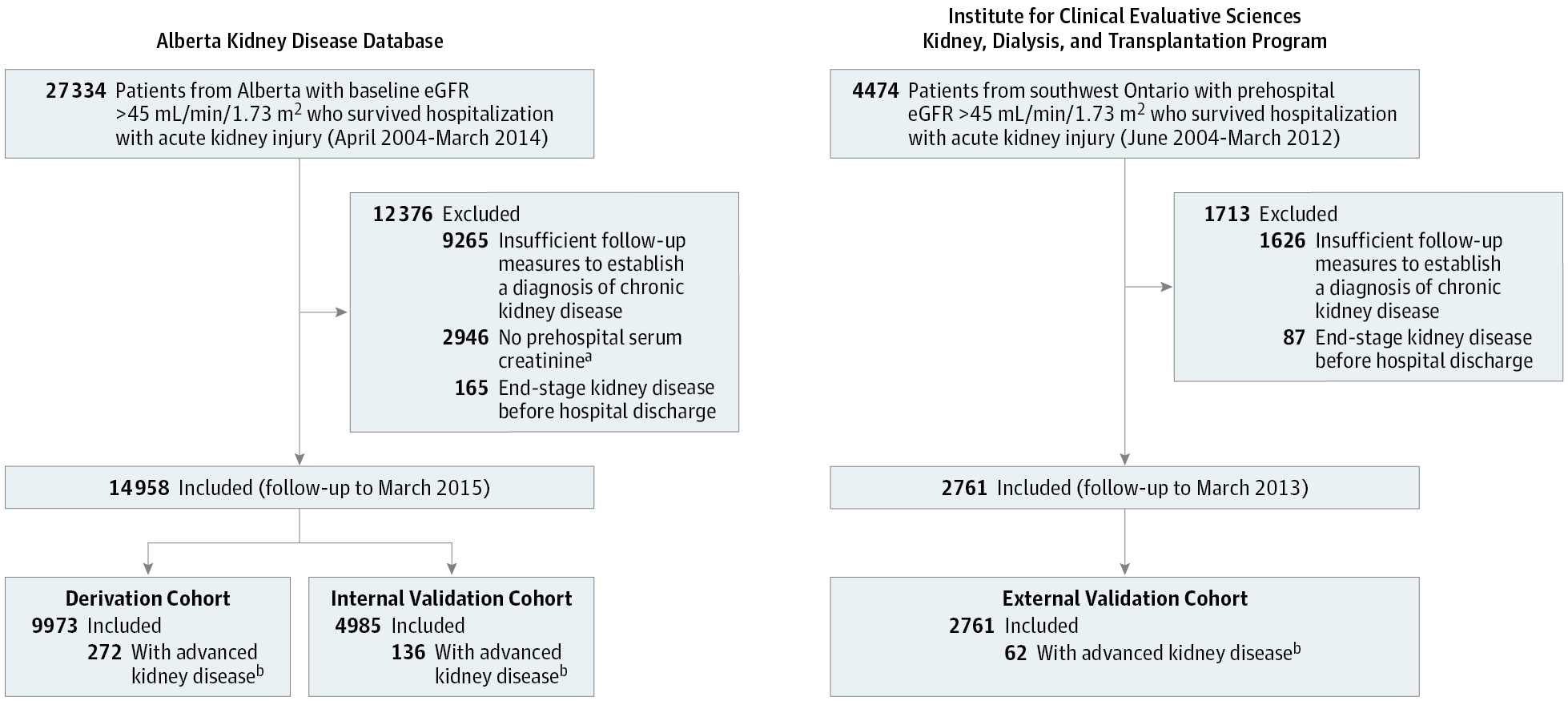
Importance Some patients will develop chronic kidney disease after a hospitalization with acute kidney injury; however, no risk-prediction tools have been developed to identify high-risk patients requiring follow-up. Objective To derive and validate predictive models for progression of acute kidney injury to advanced chronic kidney disease. Design, Setting, and Participants Data from 2 population-based cohorts of patients with a prehospitalization estimated glomerular filtration rate (eGFR) of more than 45 mL/min/1.73 m2 and who had survived hospitalization with acute kidney injury (defined by a serum creatinine increase during hospitalization > 0.3 mg/dL or > 50% of their prehospitalization baseline), were used to derive and validate multivariable prediction models. The risk models were derived from 9973 patients hospitalized in Alberta, Canada (April 2004-March 2014, with follow-up to March 2015). The risk models were externally validated with data from a cohort of 2761 patients hospitalized in Ontario, Canada (June 2004-March 2012, with follow-up to March 2013). Exposures Demographic, laboratory, and comorbidity variables measured prior to discharge. Main Outcomes and Measures Advanced chronic kidney disease was defined by a sustained reduction in eGFR less than 30 mL/min/1.73 m2 for at least 3 months during the year after discharge. All participants were followed up for up to 1 year. Results The participants (mean [SD] age, 66 [15] years in the derivation and internal validation cohorts and 69 [11] years in the external validation cohort; 40%-43% women per cohort) had a mean (SD) baseline serum creatinine level of 1.0 (0.2) mg/dL and more than 20% had stage 2 or 3 acute kidney injury. Advanced chronic kidney disease developed in 408 (2.7%) of 9973 patients in the derivation cohort and 62 (2.2%) of 2761 patients in the external validation cohort. In the derivation cohort, 6 variables were independently associated with the outcome: older age, female sex, higher baseline serum creatinine value, albuminuria, greater severity of acute kidney injury, and higher serum creatinine value at discharge. In the external validation cohort, a multivariable model including these 6 variables had a C statistic of 0.81 (95% CI, 0.75-0.86) and improved discrimination and reclassification compared with reduced models that included age, sex, and discharge serum creatinine value alone (integrated discrimination improvement, 2.6%; 95% CI, 1.1%-4.0%; categorical net reclassification index, 13.5%; 95% CI, 1.9%-25.1%) or included age, sex, and acute kidney injury stage alone (integrated discrimination improvement, 8.0%; 95% CI, 5.1%-11.0%; categorical net reclassification index, 79.9%; 95% CI, 60.9%-98.9%). Conclusions and Relevance A multivariable model using routine laboratory data was able to predict advanced chronic kidney disease following hospitalization with acute kidney injury. The utility of this model in clinical care requires further research.
中文翻译:

急性肾损伤后晚期慢性肾病预测模型的推导和外部验证
重要性 一些患者在因急性肾损伤住院后会发展为慢性肾病;然而,尚未开发出风险预测工具来识别需要随访的高风险患者。目的推导和验证急性肾损伤进展为晚期慢性肾病的预测模型。设计、设置和参与者 来自 2 个基于人群的患者队列的数据,这些患者入院前估计肾小球滤过率 (eGFR) 超过 45 mL/min/1.73 m2,并且因急性肾损伤(由血清肌酐定义)住院后幸存住院期间增加 > 0.3 mg/dL 或 > 住院前基线的 50%),用于推导和验证多变量预测模型。风险模型来自阿尔伯塔省住院的 9973 名患者,加拿大(2004 年 4 月至 2014 年 3 月,随访至 2015 年 3 月)。风险模型通过来自加拿大安大略省住院的 2761 名患者队列的数据进行外部验证(2004 年 6 月至 2012 年 3 月,随访至 2013 年 3 月)。出院前测量的人口统计学、实验室和合并症变量。主要结果和措施 晚期慢性肾病定义为出院后一年内 eGFR 持续降低低于 30 mL/min/1.73 m2 至少 3 个月。所有参与者都进行了长达 1 年的随访。结果 参与者(平均 [SD] 年龄,在推导和内部验证队列中为 66 [15] 岁,在外部验证队列中为 69 [11] 岁;每个队列 40%-43% 的女性)具有平均 (SD) 基线血清肌酐水平为 1.0 (0. 2) mg/dL 且超过 20% 的患者患有 2 或 3 期急性肾损伤。推导队列中 9973 名患者中有 408 名 (2.7%) 发生晚期慢性肾病,外部验证队列中 2761 名患者中有 62 名 (2.2%) 发生晚期慢性肾病。在推导队列中,6 个变量与结果独立相关:年龄较大、女性、较高的基线血清肌酐值、蛋白尿、急性肾损伤的严重程度以及出院时较高的血清肌酐值。在外部验证队列中,包含这 6 个变量的多变量模型的 C 统计量为 0.81(95% CI,0.75-0.86),与仅包括年龄、性别和出院血清肌酐值的简化模型相比,区分和重新分类得到改善。综合歧视改善,2.6%;95% CI,1.1%-4.0%;分类净重分类指数,13.5%;95% CI,1.9%-25.1%)或仅包括年龄、性别和急性肾损伤阶段(综合鉴别改善,8.0%;95% CI,5.1%-11.0%;分类净重分类指数,79.9%;95%置信区间,60.9%-98.9%)。结论和相关性 使用常规实验室数据的多变量模型能够预测因急性肾损伤住院后的晚期慢性肾病。这种模式在临床护理中的效用需要进一步研究。结论和相关性 使用常规实验室数据的多变量模型能够预测因急性肾损伤住院后的晚期慢性肾病。这种模式在临床护理中的效用需要进一步研究。结论和相关性 使用常规实验室数据的多变量模型能够预测因急性肾损伤住院后的晚期慢性肾病。这种模式在临床护理中的效用需要进一步研究。
更新日期:2017-11-14
中文翻译:
急性肾损伤后晚期慢性肾病预测模型的推导和外部验证
重要性 一些患者在因急性肾损伤住院后会发展为慢性肾病;然而,尚未开发出风险预测工具来识别需要随访的高风险患者。目的推导和验证急性肾损伤进展为晚期慢性肾病的预测模型。设计、设置和参与者 来自 2 个基于人群的患者队列的数据,这些患者入院前估计肾小球滤过率 (eGFR) 超过 45 mL/min/1.73 m2,并且因急性肾损伤(由血清肌酐定义)住院后幸存住院期间增加 > 0.3 mg/dL 或 > 住院前基线的 50%),用于推导和验证多变量预测模型。风险模型来自阿尔伯塔省住院的 9973 名患者,加拿大(2004 年 4 月至 2014 年 3 月,随访至 2015 年 3 月)。风险模型通过来自加拿大安大略省住院的 2761 名患者队列的数据进行外部验证(2004 年 6 月至 2012 年 3 月,随访至 2013 年 3 月)。出院前测量的人口统计学、实验室和合并症变量。主要结果和措施 晚期慢性肾病定义为出院后一年内 eGFR 持续降低低于 30 mL/min/1.73 m2 至少 3 个月。所有参与者都进行了长达 1 年的随访。结果 参与者(平均 [SD] 年龄,在推导和内部验证队列中为 66 [15] 岁,在外部验证队列中为 69 [11] 岁;每个队列 40%-43% 的女性)具有平均 (SD) 基线血清肌酐水平为 1.0 (0. 2) mg/dL 且超过 20% 的患者患有 2 或 3 期急性肾损伤。推导队列中 9973 名患者中有 408 名 (2.7%) 发生晚期慢性肾病,外部验证队列中 2761 名患者中有 62 名 (2.2%) 发生晚期慢性肾病。在推导队列中,6 个变量与结果独立相关:年龄较大、女性、较高的基线血清肌酐值、蛋白尿、急性肾损伤的严重程度以及出院时较高的血清肌酐值。在外部验证队列中,包含这 6 个变量的多变量模型的 C 统计量为 0.81(95% CI,0.75-0.86),与仅包括年龄、性别和出院血清肌酐值的简化模型相比,区分和重新分类得到改善。综合歧视改善,2.6%;95% CI,1.1%-4.0%;分类净重分类指数,13.5%;95% CI,1.9%-25.1%)或仅包括年龄、性别和急性肾损伤阶段(综合鉴别改善,8.0%;95% CI,5.1%-11.0%;分类净重分类指数,79.9%;95%置信区间,60.9%-98.9%)。结论和相关性 使用常规实验室数据的多变量模型能够预测因急性肾损伤住院后的晚期慢性肾病。这种模式在临床护理中的效用需要进一步研究。结论和相关性 使用常规实验室数据的多变量模型能够预测因急性肾损伤住院后的晚期慢性肾病。这种模式在临床护理中的效用需要进一步研究。结论和相关性 使用常规实验室数据的多变量模型能够预测因急性肾损伤住院后的晚期慢性肾病。这种模式在临床护理中的效用需要进一步研究。










































 京公网安备 11010802027423号
京公网安备 11010802027423号