PLOS Medicine ( IF 10.5 ) Pub Date : 2017-11-14 , DOI: 10.1371/journal.pmed.1002433 Batya Elul , Matthew R. Lamb , Maria Lahuerta , Fatima Abacassamo , Laurence Ahoua , Stephanie A. Kujawski , Maria Tomo , Ilesh Jani
|
Background
Concerning gaps in the HIV care continuum compromise individual and population health. We evaluated a combination intervention strategy (CIS) targeting prevalent barriers to timely linkage and sustained retention in HIV care in Mozambique.
Methods and findings
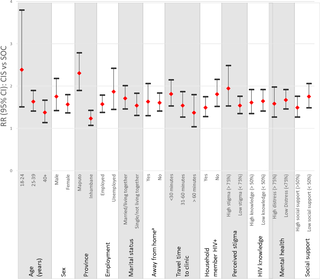
In this cluster-randomized trial, 10 primary health facilities in the city of Maputo and Inhambane Province were randomly assigned to provide the CIS or the standard of care (SOC). The CIS included point-of-care CD4 testing at the time of diagnosis, accelerated ART initiation, and short message service (SMS) health messages and appointment reminders. A pre–post intervention 2-sample design was nested within the CIS arm to assess the effectiveness of CIS+, an enhanced version of the CIS that additionally included conditional non-cash financial incentives for linkage and retention. The primary outcome was a combined outcome of linkage to care within 1 month and retention at 12 months after diagnosis. From April 22, 2013, to June 30, 2015, we enrolled 2,004 out of 5,327 adults ≥18 years of age diagnosed with HIV in the voluntary counseling and testing clinics of participating health facilities: 744 (37%) in the CIS group, 493 (25%) in the CIS+ group, and 767 (38%) in the SOC group. Fifty-seven percent of the CIS group achieved the primary outcome versus 35% in the SOC group (relative risk [RR]CIS vs SOC = 1.58, 95% CI 1.05–2.39). Eighty-nine percent of the CIS group linked to care on the day of diagnosis versus 16% of the SOC group (RRCIS vs SOC = 9.13, 95% CI 1.65–50.40). There was no significant benefit of adding financial incentives to the CIS in terms of the combined outcome (55% of the CIS+ group achieved the primary outcome, RRCIS+ vs CIS = 0.96, 95% CI 0.81–1.16). Key limitations include the use of existing medical records to assess outcomes, the inability to isolate the effect of each component of the CIS, non-concurrent enrollment of the CIS+ group, and exclusion of many patients newly diagnosed with HIV.
Conclusions
The CIS showed promise for making much needed gains in the HIV care continuum in our study, particularly in the critical first step of timely linkage to care following diagnosis.
Trial registration
ClinicalTrials.gov NCT01930084
中文翻译:
莫桑比克诊断后改善与艾滋病毒护理的联系和保留的联合干预策略:一项整群随机研究
背景
关于艾滋病毒护理连续性方面的差距损害了个人和人口的健康。我们评估了联合干预策略(CIS),该策略针对莫桑比克艾滋病毒治疗中及时联系和持续保留的普遍障碍。
方法和发现
在该整群随机试验中,马普托市和伊尼扬巴内省的10个主要医疗机构被随机分配以提供CIS或护理标准(SOC)。CIS包括诊断时的即时医疗CD4测试,加速的ART发起以及短消息服务(SMS)健康消息和约会提醒。在CIS部门内部嵌套了一个事前干预2样本设计,以评估CIS +的有效性,CIS +是CIS的增强版本,另外还包括有条件的非现金财务激励措施,以实现联系和保留。主要结局是在诊断后1个月内联系护理并在诊断后12个月保留的综合结果。从2013年4月22日到2015年6月30日,我们在5人中注册了2,004人,在参与的卫生机构的自愿咨询和检测诊所中,有327名≥18岁的成年人被诊断出患有HIV:CIS组中的744(37%),CIS +组中的493(25%)和767+(38%)。 SOC组。CIS组有57%达到了主要结局,而SOC组为35%(相对风险[RR]CIS vs SOC = 1.58,95%CI 1.05–2.39)。CIS组中有89%在诊断当天与护理相关,而SOC组为16%(RR CIS vs SOC = 9.13,95%CI 1.65–50.40)。就合并结果而言,向独联体国家增加经济激励没有显着益处(55%的独联体+达到了主要结局,RR CIS + vs独联体= 0.96,95%CI 0.81–1.16)。主要的局限性包括使用现有的医疗记录评估结果,无法隔离CIS各个组成部分的影响,CIS +组的非同时入组以及排除许多新诊断为HIV的患者。
结论
独联体在我们的研究中显示出有望在艾滋病毒护理连续体中取得急需的收获的希望,特别是在诊断后及时与护理建立联系的关键第一步。
试用注册
ClinicalTrials.gov NCT01930084









































 京公网安备 11010802027423号
京公网安备 11010802027423号