PLOS Medicine ( IF 10.5 ) Pub Date : 2017-11-14 , DOI: 10.1371/journal.pmed.1002427 James A Lopez Bernal 1, 2 , Christine Y Lu 2 , Antonio Gasparrini 1 , Steven Cummins 1 , J Frank Wharam 2 , Steven B Soumerai 2
|
Background
The 2012 Health and Social Care Act (HSCA) in England led to among the largest healthcare reforms in the history of the National Health Service (NHS). It gave control of £67 billion of the NHS budget for secondary care to general practitioner (GP) led Clinical Commissioning Groups (CCGs). An expected outcome was that patient care would shift away from expensive hospital and specialist settings, towards less expensive community-based models. However, there is little evidence for the effectiveness of this approach. In this study, we aimed to assess the association between the NHS reforms and hospital admissions and outpatient specialist visits.
Methods and findings
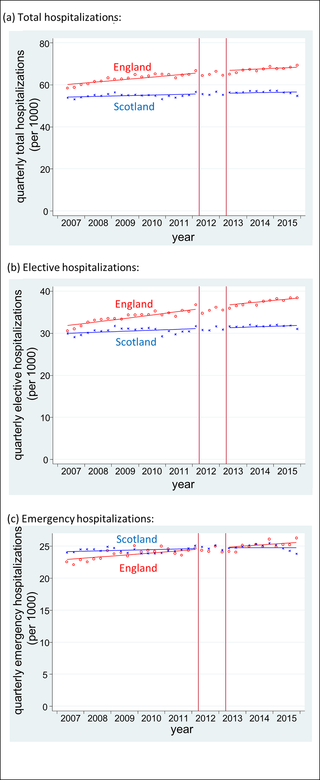
We conducted a controlled interrupted time series analysis to examine rates of outpatient specialist visits and inpatient hospitalisations before and after the implementation of the HSCA. We used national routine hospital administrative data (Hospital Episode Statistics) on all NHS outpatient specialist visits and inpatient hospital admissions in England between 2007 and 2015 (with a mean of 26.8 million new outpatient visits and 14.9 million inpatient admissions per year). As a control series, we used equivalent data on hospital attendances in Scotland. Primary outcomes were: total, elective, and emergency hospitalisations, and total and GP-referred specialist visits. Both countries had stable trends in all outcomes at baseline. In England, after the policy, there was a 1.1% (95% CI 0.7%–1.5%; p < 0.001) increase in total specialist visits per quarter and a 1.6% increase in GP-referred specialist visits (95% CI 1.2%–2.0%; p < 0.001) per quarter, equivalent to 12.7% (647,000 over the 5,105,000 expected) and 19.1% (507,000 over the 2,658,000 expected) more visits per quarter by the end of 2015, respectively. In Scotland, there was no change in specialist visits. Neither country experienced a change in trends in hospitalisations: change in slope for total, elective, and emergency hospitalisations were −0.2% (95% CI −0.6%–0.2%; p = 0.257), −0.2% (95% CI −0.6%–0.1%; p = 0.235), and 0.0% (95% CI −0.5%–0.4%; p = 0.866) per quarter in England. We are unable to exclude confounding due to other events occurring around the time of the policy. However, we limited the likelihood of such confounding by including relevant control series, in which no changes were seen.
Conclusions
Our findings suggest that giving control of healthcare budgets to GP-led CCGs was not associated with a reduction in overall hospitalisations and was associated with an increase in specialist visits.
中文翻译:
2012 年《健康和社会关怀法案》与英格兰专科医生就诊和住院之间的关联:受控中断时间序列分析
背景
英国 2012 年《健康与社会保健法案》(HSCA) 引发了国民医疗服务体系 (NHS) 历史上最大规模的医疗改革。它将 NHS 二级护理预算中 670 亿英镑的控制权交给全科医生 (GP) 领导的临床调试小组 (CCG)。预期的结果是患者护理将从昂贵的医院和专科环境转向更便宜的社区模式。然而,几乎没有证据表明这种方法的有效性。在这项研究中,我们旨在评估 NHS 改革与住院和门诊专家就诊之间的关联。
方法和结果
我们进行了受控中断时间序列分析,以检查 HSCA 实施前后的门诊专科就诊率和住院率。我们使用了 2007 年至 2015 年间英格兰所有 NHS 门诊专家就诊和住院患者入院的国家常规医院管理数据(医院事件统计)(平均每年新增门诊患者 2680 万人次,住院患者入院人数 1490 万人次)。作为对照系列,我们使用了苏格兰医院出勤率的等效数据。主要结局包括:总住院率、择期住院率和紧急住院率,以及总住院率和全科医生转介的专科医生就诊率。两国的基线所有结果均呈现稳定趋势。在英格兰,实施该政策后,每季度专科医生就诊总数增加了 1.1% (95% CI 0.7%–1.5%; p < 0.001),全科医生转介的专科医生就诊次数增加了 1.6% (95% CI 1.2) %–2.0%; p < 0.001),相当于到 2015 年底每季度访问量分别增加 12.7%(比预期 5,105,000 次增加 647,000 次)和 19.1%(比预期 2,658,000 次增加 507,000 次)。在苏格兰,专家就诊次数没有变化。两个国家的住院率趋势均未发生变化:总住院率、择期住院率和急诊住院率的斜率变化分别为 -0.2% (95% CI -0.6%–0.2%; p = 0.257)、-0.2% (95% CI -0.6) %–0.1%; p = 0.235),而英格兰每季度为 0.0%(95% CI -0.5%–0.4%; p = 0.866)。我们无法排除保单期间发生的其他事件造成的混淆。然而,我们通过包含相关的控制系列来限制这种混淆的可能性,其中没有看到任何变化。
结论
我们的研究结果表明,将医疗保健预算控制权交给全科医生主导的 CCG 与总体住院率的减少无关,而与专科医生就诊的增加有关。










































 京公网安备 11010802027423号
京公网安备 11010802027423号