当前位置:
X-MOL 学术
›
JAMA Intern. Med.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Intensive Blood Pressure Control in Autosomal Dominant Polycystic Kidney Disease—How Safe Is It?—Reply
JAMA Internal Medicine ( IF 22.5 ) Pub Date : 2017-11-01 , DOI: 10.1001/jamainternmed.2017.4925 Wan-Chuan Tsai, Kuo-Liong Chien, Hon-Yen Wu
JAMA Internal Medicine ( IF 22.5 ) Pub Date : 2017-11-01 , DOI: 10.1001/jamainternmed.2017.4925 Wan-Chuan Tsai, Kuo-Liong Chien, Hon-Yen Wu
|
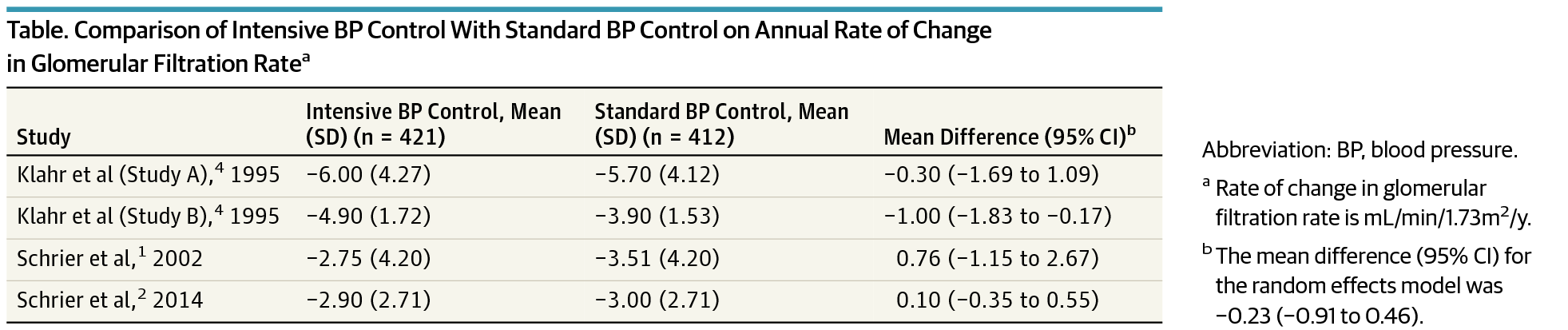
Intensive Blood Pressure Control in Autosomal Dominant Polycystic Kidney Disease— How Safe Is It? To the Editor Maintaining optimal blood pressure in patients without diabetes with chronic kidney disease (CKD) has always been controversial. In a systematic review and metaanalysis published in a recent issue of JAMA Internal Medicine, Tsai et al1 assessed the clinical data of 8127 patients; they focused on detecting an association between intensive blood pressure control and renal outcomes in patients without diabetes with CKD. Consequently, no significant difference in major renal outcomes was found between intensive (<130/80 mm Hg) and standard BP control (<140/90 mm Hg) groups during a median follow-up of 3.3 years. Nevertheless, nonblack patients or those with higher levels of proteinuria were found to benefit from the intensive BP-lowering strategy. Interestingly, patients with polycystic kidney disease (ADPKD) were also included in this study.1 Very few studies have been conducted on the hypertension control in the population of patients with ADPKD. Schrier et al,2 in a study conducted on 558 patients ages 15 to 49 years and in their early CKD stages, assigned the groups to either standard (120/70130/80 mm Hg) or low (95/60-110/75 mm Hg) blood pressure target groups. Authors found that maintaining rigorous BP control in young healthy hypertensive patients with ADPKD with relatively preserved kidney function at earlier stages of the disease is associated with a slower increase in total kidney volume, greater reduction in urinary albumin excretion, and a greater decline in the left ventricular mass index. However, no further renal benefits such as improved renal function was observed following low BP target strategy. Unlike patients with CKD with other underlying mechanisms, intensive blood pressure lowering should be practiced more cautiously in patients with ADPKD. Given that there is bilateral intrarenal ischemia in ADPKD due to the compression effect of the cyst, these patients are potentially vulnerable to acute renal perfusion changes following initiation of RAAS blockers particularly in those with severer renal insufficiency and massive cystic diseases. RAAS (renin-angiotensin-aldosterone system) blockers might impair the already-compromised perfusion of the intact normal renal parenchyma which is compensated by the elevated systemic pressure. Hence, administration of RAAS blockers should be performed more vigilantly in patients with ADPKD.
中文翻译:

常染色体显性多囊肾病的强化血压控制——安全性如何?——回复
常染色体显性多囊肾病的强化血压控制——安全性如何?致编辑 对于患有慢性肾病 (CKD) 的非糖尿病患者维持最佳血压一直存在争议。在最近一期 JAMA Internal Medicine 上发表的系统评价和荟萃分析中,Tsai 等人 1 评估了 8127 名患者的临床数据;他们专注于检测非糖尿病 CKD 患者强化血压控制与肾脏结局之间的关联。因此,在中位随访 3.3 年期间,强化(<130/80 mmHg)和标准血压控制(<140/90 mmHg)组之间的主要肾脏结局没有显着差异。尽管如此,发现非黑人患者或蛋白尿水平较高的患者受益于强化降压策略。有趣的是,多囊肾病 (ADPKD) 患者也包括在本研究中。1 关于 ADPKD 患者人群高血压控制的研究很少。Schrier 等人 2 在对 558 名年龄在 15 至 49 岁且处于早期 CKD 阶段的患者进行的研究中,将各组分为标准 (120/70130/80 毫米汞柱) 或低 (95/60-110/75 毫米汞柱) Hg) 血压目标群体。作者发现,在疾病早期阶段肾功能相对保留的年轻健康的 ADPKD 高血压患者中保持严格的血压控制与总肾脏体积增加较慢,尿白蛋白排泄减少更多有关,并且左心室质量指数下降幅度更大。然而,在低血压目标策略后没有观察到进一步的肾脏益处,例如改善肾功能。与具有其他潜在机制的 CKD 患者不同,ADPKD 患者应更加谨慎地进行强化降压。鉴于由于囊肿的压迫作用,ADPKD 患者存在双侧肾内缺血,这些患者在开始使用 RAAS 阻滞剂后可能容易受到急性肾灌注变化的影响,特别是在那些患有严重肾功能不全和大量囊性疾病的患者中。RAAS(肾素-血管紧张素-醛固酮系统)阻滞剂可能会损害已经受损的完整正常肾实质的灌注,而该灌注可通过升高的全身压力得到补偿。因此,
更新日期:2017-11-01
中文翻译:
常染色体显性多囊肾病的强化血压控制——安全性如何?——回复
常染色体显性多囊肾病的强化血压控制——安全性如何?致编辑 对于患有慢性肾病 (CKD) 的非糖尿病患者维持最佳血压一直存在争议。在最近一期 JAMA Internal Medicine 上发表的系统评价和荟萃分析中,Tsai 等人 1 评估了 8127 名患者的临床数据;他们专注于检测非糖尿病 CKD 患者强化血压控制与肾脏结局之间的关联。因此,在中位随访 3.3 年期间,强化(<130/80 mmHg)和标准血压控制(<140/90 mmHg)组之间的主要肾脏结局没有显着差异。尽管如此,发现非黑人患者或蛋白尿水平较高的患者受益于强化降压策略。有趣的是,多囊肾病 (ADPKD) 患者也包括在本研究中。1 关于 ADPKD 患者人群高血压控制的研究很少。Schrier 等人 2 在对 558 名年龄在 15 至 49 岁且处于早期 CKD 阶段的患者进行的研究中,将各组分为标准 (120/70130/80 毫米汞柱) 或低 (95/60-110/75 毫米汞柱) Hg) 血压目标群体。作者发现,在疾病早期阶段肾功能相对保留的年轻健康的 ADPKD 高血压患者中保持严格的血压控制与总肾脏体积增加较慢,尿白蛋白排泄减少更多有关,并且左心室质量指数下降幅度更大。然而,在低血压目标策略后没有观察到进一步的肾脏益处,例如改善肾功能。与具有其他潜在机制的 CKD 患者不同,ADPKD 患者应更加谨慎地进行强化降压。鉴于由于囊肿的压迫作用,ADPKD 患者存在双侧肾内缺血,这些患者在开始使用 RAAS 阻滞剂后可能容易受到急性肾灌注变化的影响,特别是在那些患有严重肾功能不全和大量囊性疾病的患者中。RAAS(肾素-血管紧张素-醛固酮系统)阻滞剂可能会损害已经受损的完整正常肾实质的灌注,而该灌注可通过升高的全身压力得到补偿。因此,






































 京公网安备 11010802027423号
京公网安备 11010802027423号