当前位置:
X-MOL 学术
›
Eur. J. Heart Fail.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Impact of baseline kidney dysfunction on oral diuretic efficacy following hospitalization for heart failure – insights from TRANSFORM‐HF
European Journal of Heart Failure ( IF 18.2 ) Pub Date : 2024-04-01 , DOI: 10.1002/ejhf.3207 Pieter Martens 1, 2 , Stephen J. Greene 3 , Robert J. Mentz 3 , Shuang Li 3 , Daniel Wojdyla 3 , Chris J. Kapelios 4 , Wilfried Mullens 1 , Michael E. Hall 5 , Fassil Ketema 6 , Dong‐Yun Kim 6 , Eric L. Eisenstein 3 , Kevin Anstrom 3 , James C. Fang 4 , Bertram Pitt 7 , Eric J. Velazquez 3 , W.H. Wilson Tang 2
European Journal of Heart Failure ( IF 18.2 ) Pub Date : 2024-04-01 , DOI: 10.1002/ejhf.3207 Pieter Martens 1, 2 , Stephen J. Greene 3 , Robert J. Mentz 3 , Shuang Li 3 , Daniel Wojdyla 3 , Chris J. Kapelios 4 , Wilfried Mullens 1 , Michael E. Hall 5 , Fassil Ketema 6 , Dong‐Yun Kim 6 , Eric L. Eisenstein 3 , Kevin Anstrom 3 , James C. Fang 4 , Bertram Pitt 7 , Eric J. Velazquez 3 , W.H. Wilson Tang 2
Affiliation
|
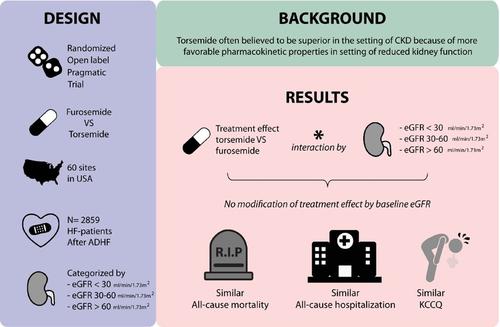
AimAmong patients discharged after hospitalization for heart failure (HF), a strategy of torsemide versus furosemide showed no difference in all‐cause mortality or hospitalization. Clinicians have traditionally favoured torsemide in the setting of kidney dysfunction due to better oral bioavailability and longer half‐life, but direct supportive evidence is lacking.Methods and resultsThe TRANSFORM‐HF trial randomized patients hospitalized for HF to a long‐term strategy of torsemide versus furosemide, and enrolled patients across the spectrum of renal function (without dialysis). In this post‐hoc analysis, baseline renal function during the index hospitalization was assessed as categories of estimated glomerular filtration rate (eGFR; <30, 30–<60, ≥60 ml/min/1.73 m2 ). The interaction between baseline renal function and treatment effect of torsemide versus furosemide was assessed with respect to mortality and hospitalization outcomes, and the change in Kansas City Cardiomyopathy Questionnaire clinical summary score (KCCQ‐CSS). Of 2859 patients randomized, 336 (11.8%) had eGFR <30 ml/min/1.73 m2 , 1138 (39.8%) had eGFR 30–<60 ml/min/1.73 m2 , and 1385 (48.4%) had eGFR ≥60 ml/min/1.73 m2 . Baseline eGFR did not modify treatment effects of torsemide versus furosemide on all adverse clinical outcomes including individual components or composites of all‐cause mortality and all‐cause (re)‐hospitalizations, both when assessing eGFR categorically or continuously (p ‐value for interaction all >0.108). Similarly, no treatment effect modification by eGFR was found for the change in KCCQ‐CSS (p ‐value for interaction all >0.052) when assessing eGFR categorically or continuously.ConclusionAmong patients discharged after hospitalization for HF, there was no significant difference in clinical and patient‐reported outcomes between torsemide and furosemide, irrespective of renal function.
中文翻译:

心力衰竭住院后基线肾功能障碍对口服利尿剂疗效的影响——来自 TRANSFORM-HF 的见解
目的在因心力衰竭 (HF) 住院后出院的患者中,托拉塞米与呋塞米策略显示全因死亡率或住院率没有差异。由于口服生物利用度更好和半衰期更长,临床医生传统上倾向于在肾功能不全的情况下使用托拉塞米,但缺乏直接支持证据。 方法和结果 TRANSFORM-HF 试验将因心力衰竭住院的患者随机分为托拉塞米长期治疗方案和托拉塞米治疗方案。呋塞米,并招募了各种肾功能的患者(无需透析)。在这项事后分析中,指数住院期间的基线肾功能被评估为估计肾小球滤过率(eGFR;<30、30–<60、≥60 ml/min/1.73 m2 )。根据死亡率和住院结果以及堪萨斯城心肌病问卷临床总结评分(KCCQ-CSS)的变化,评估基线肾功能与托拉塞米与呋塞米治疗效果之间的相互作用。在 2859 名随机患者中,336 名 (11.8%) 的 eGFR <30 ml/min/1.73 m2 , 1138 (39.8%) 的 eGFR 30–<60 ml/min/1.73 m2 ,1385 名 (48.4%) 的 eGFR ≥60 ml/min/1.73 m2 。基线 eGFR 并没有改变托拉塞米与呋塞米对所有不良临床结果的治疗效果,包括全因死亡率和全因(再)住院率的单个组成部分或综合结果,无论是分类还是连续评估 eGFR 时(p ‐交互作用值均>0.108)。同样,没有发现 eGFR 对 KCCQ-CSS 变化的治疗效果有影响(p ‐当明确或连续评估 eGFR 时,交互作用值均 >0.052)。结论 在因 HF 住院后出院的患者中,无论肾功能如何,托拉塞米和呋塞米的临床和患者报告结果均无显着差异。
更新日期:2024-04-01
中文翻译:
心力衰竭住院后基线肾功能障碍对口服利尿剂疗效的影响——来自 TRANSFORM-HF 的见解
目的在因心力衰竭 (HF) 住院后出院的患者中,托拉塞米与呋塞米策略显示全因死亡率或住院率没有差异。由于口服生物利用度更好和半衰期更长,临床医生传统上倾向于在肾功能不全的情况下使用托拉塞米,但缺乏直接支持证据。 方法和结果 TRANSFORM-HF 试验将因心力衰竭住院的患者随机分为托拉塞米长期治疗方案和托拉塞米治疗方案。呋塞米,并招募了各种肾功能的患者(无需透析)。在这项事后分析中,指数住院期间的基线肾功能被评估为估计肾小球滤过率(eGFR;<30、30–<60、≥60 ml/min/1.73 m


























 京公网安备 11010802027423号
京公网安备 11010802027423号