当前位置:
X-MOL 学术
›
Am. J. Kidney Dis.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
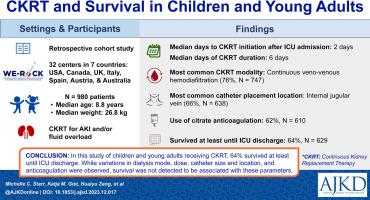
Continuous Kidney Replacement Therapy and Survival in Children and Young Adults: Findings From the Multinational WE-ROCK Collaborative
American Journal of Kidney Diseases ( IF 13.2 ) Pub Date : 2024-02-15 , DOI: 10.1053/j.ajkd.2023.12.017 Michelle C. Starr , Katja M. Gist , Huaiyu Zang , Nicholas J. Ollberding , Shanthi Balani , Andrea Cappoli , Eileen Ciccia , Catherine Joseph , Aadil Kakajiwala , Aaron Kessel , Melissa Muff-Luett , María J. Santiago Lozano , Matthew Pinto , Stephanie Reynaud , Sonia Solomon , Cara Slagle , Rachana Srivastava , Weiwen V. Shih , Tennille Webb , Shina Menon , Emily Ahern , Ayse Akcan Arikan , Issa Alhamoud , Rashid Alobaidi , Pilar Anton-Martin , Matthew Barhight , Abby Basalely , Amee M. Bigelow , Gabriella Bottari , Michaela Collins , Denise Colosimo , Gerard Cortina , Mihaela A. Damian , Sara De la Mata Navazo , Gabrielle DeAbreu , Akash Deep , Kathy L. Ding , Kristin J. Dolan , Sarah N. Fernandez Lafever , Dana Y. Fuhrman , Ben Gelbart , Stephen M. Gorga , Francesco Guzzi , Isabella Guzzo , Taiki Haga , Elizabeth Harvey , Denise C. Hasson , Taylor Hill-Horowitz , Haleigh Inthavong , Ahmad Kaddourah , Sarah Korn , Kelli A. Krallman , David M. Kwiatkowski , Jasmine Lee , Laurance Lequier , Tina Madani Kia , Kenneth E. Mah , Eleonora Marinari , Susan D. Martin , Tahagod H. Mohamed , Catherine Morgan , Theresa A. Mottes , Siva Namachivayam , Tara M. Neumayr , Jennifer Nhan , Abigail O'Rourke , Dua Qutob , Valeria Raggi , Zaccaria Ricci , Zachary A. Rumlow , Emily See , David T. Selewski , Carmela Serpe , Alyssa Serratore , Ananya Shah , H Stella Shin , Danielle E. Soranno , Natalja L. Stanski , Erin K. Stenson , Amy E. Strong , Susan A. Taylor , Sameer V. Thadani , Amanda M. Uber , Brynna Van Wyk ARNP , Emily E. Zangla , Michael Zappitelli
American Journal of Kidney Diseases ( IF 13.2 ) Pub Date : 2024-02-15 , DOI: 10.1053/j.ajkd.2023.12.017 Michelle C. Starr , Katja M. Gist , Huaiyu Zang , Nicholas J. Ollberding , Shanthi Balani , Andrea Cappoli , Eileen Ciccia , Catherine Joseph , Aadil Kakajiwala , Aaron Kessel , Melissa Muff-Luett , María J. Santiago Lozano , Matthew Pinto , Stephanie Reynaud , Sonia Solomon , Cara Slagle , Rachana Srivastava , Weiwen V. Shih , Tennille Webb , Shina Menon , Emily Ahern , Ayse Akcan Arikan , Issa Alhamoud , Rashid Alobaidi , Pilar Anton-Martin , Matthew Barhight , Abby Basalely , Amee M. Bigelow , Gabriella Bottari , Michaela Collins , Denise Colosimo , Gerard Cortina , Mihaela A. Damian , Sara De la Mata Navazo , Gabrielle DeAbreu , Akash Deep , Kathy L. Ding , Kristin J. Dolan , Sarah N. Fernandez Lafever , Dana Y. Fuhrman , Ben Gelbart , Stephen M. Gorga , Francesco Guzzi , Isabella Guzzo , Taiki Haga , Elizabeth Harvey , Denise C. Hasson , Taylor Hill-Horowitz , Haleigh Inthavong , Ahmad Kaddourah , Sarah Korn , Kelli A. Krallman , David M. Kwiatkowski , Jasmine Lee , Laurance Lequier , Tina Madani Kia , Kenneth E. Mah , Eleonora Marinari , Susan D. Martin , Tahagod H. Mohamed , Catherine Morgan , Theresa A. Mottes , Siva Namachivayam , Tara M. Neumayr , Jennifer Nhan , Abigail O'Rourke , Dua Qutob , Valeria Raggi , Zaccaria Ricci , Zachary A. Rumlow , Emily See , David T. Selewski , Carmela Serpe , Alyssa Serratore , Ananya Shah , H Stella Shin , Danielle E. Soranno , Natalja L. Stanski , Erin K. Stenson , Amy E. Strong , Susan A. Taylor , Sameer V. Thadani , Amanda M. Uber , Brynna Van Wyk ARNP , Emily E. Zangla , Michael Zappitelli
|
There are limited studies describing the epidemiology and outcomes in children and young adults receiving continuous kidney replacement therapy (CKRT). We aimed to describe associations between patient characteristics, CKRT prescription, and survival. Retrospective multicenter cohort study. 980 patients aged from birth to 25 years who received CKRT between 2015 and 2021 at 1 of 32 centers in 7 countries participating in WE-ROCK (Worldwide Exploration of Renal Replacement Outcomes Collaborative in Kidney Diseases). CKRT for acute kidney injury or volume overload. Death before intensive care unit (ICU) discharge. Descriptive statistics. Median age was 8.8 years (IQR, 1.6-15.0), and median weight was 26.8 (IQR, 11.6-55.0) kg. CKRT was initiated a median of 2 (IQR, 1-6) days after ICU admission and lasted a median of 6 (IQR, 3-14) days. The most common CKRT modality was continuous venovenous hemodiafiltration. Citrate anticoagulation was used in 62%, and the internal jugular vein was the most common catheter placement location (66%). 629 participants (64.1%) survived at least until ICU discharge. CKRT dose, filter type, and anticoagulation were similar in those who did and did not survive to ICU discharge. There were apparent practice variations by institutional ICU size. Retrospective design; limited representation from centers outside the United States. In this study of children and young adults receiving CKRT, approximately two thirds survived at least until ICU discharge. Although variations in dialysis mode and dose, catheter size and location, and anticoagulation were observed, survival was not detected to be associated with these parameters. In this large contemporary epidemiological study of children and young adults receiving continuous kidney replacement therapy in the intensive care unit, we observed that two thirds of patients survived at least until ICU discharge. However, patients with comorbidities appeared to have worse outcomes. Compared with previously published reports on continuous kidney replacement therapy practice, we observed greater use of continuous venovenous hemodiafiltration with regional citrate anticoagulation.
中文翻译:

儿童和青少年的持续肾脏替代治疗和生存:来自跨国 WE-ROCK 合作组织的调查结果
描述接受连续肾脏替代治疗 (CKRT) 的儿童和年轻人的流行病学和结果的研究有限。我们的目的是描述患者特征、CKRT 处方和生存之间的关联。回顾性多中心队列研究。 2015 年至 2021 年间,980 名年龄从出生到 25 岁的患者在参与 WE-ROCK(肾脏疾病肾脏替代结果全球探索合作)的 7 个国家的 32 个中心之一接受了 CKRT。 CKRT 用于治疗急性肾损伤或容量超负荷。重症监护病房 (ICU) 出院前死亡。描述性统计。中位年龄为 8.8 岁(IQR,1.6-15.0),中位体重为 26.8(IQR,11.6-55.0)kg。 CKRT 在入住 ICU 后中位 2(IQR,1-6)天开始,持续中位 6(IQR,3-14)天。最常见的 CKRT 方式是连续静脉-静脉血液透析滤过。 62% 使用柠檬酸盐抗凝,颈内静脉是最常见的导管放置位置 (66%)。 629 名参与者 (64.1%) 至少存活到 ICU 出院。存活至 ICU 和未存活至 ICU 的患者的 CKRT 剂量、过滤器类型和抗凝治疗相似。不同机构 ICU 规模的实践存在明显差异。回顾性设计;来自美国以外的中心的代表性有限。在这项针对接受 CKRT 的儿童和年轻人的研究中,大约三分之二的人至少存活到 ICU 出院。尽管观察到透析模式和剂量、导管尺寸和位置以及抗凝治疗的变化,但未发现存活率与这些参数相关。在这项针对在重症监护病房接受连续肾脏替代治疗的儿童和年轻人的大型当代流行病学研究中,我们观察到三分之二的患者至少存活到 ICU 出院。然而,患有合并症的患者的预后似乎更差。与之前发表的有关连续肾脏替代治疗实践的报告相比,我们观察到连续静脉血液透析滤过与局部柠檬酸盐抗凝的使用更多。
更新日期:2024-02-15
中文翻译:
儿童和青少年的持续肾脏替代治疗和生存:来自跨国 WE-ROCK 合作组织的调查结果
描述接受连续肾脏替代治疗 (CKRT) 的儿童和年轻人的流行病学和结果的研究有限。我们的目的是描述患者特征、CKRT 处方和生存之间的关联。回顾性多中心队列研究。 2015 年至 2021 年间,980 名年龄从出生到 25 岁的患者在参与 WE-ROCK(肾脏疾病肾脏替代结果全球探索合作)的 7 个国家的 32 个中心之一接受了 CKRT。 CKRT 用于治疗急性肾损伤或容量超负荷。重症监护病房 (ICU) 出院前死亡。描述性统计。中位年龄为 8.8 岁(IQR,1.6-15.0),中位体重为 26.8(IQR,11.6-55.0)kg。 CKRT 在入住 ICU 后中位 2(IQR,1-6)天开始,持续中位 6(IQR,3-14)天。最常见的 CKRT 方式是连续静脉-静脉血液透析滤过。 62% 使用柠檬酸盐抗凝,颈内静脉是最常见的导管放置位置 (66%)。 629 名参与者 (64.1%) 至少存活到 ICU 出院。存活至 ICU 和未存活至 ICU 的患者的 CKRT 剂量、过滤器类型和抗凝治疗相似。不同机构 ICU 规模的实践存在明显差异。回顾性设计;来自美国以外的中心的代表性有限。在这项针对接受 CKRT 的儿童和年轻人的研究中,大约三分之二的人至少存活到 ICU 出院。尽管观察到透析模式和剂量、导管尺寸和位置以及抗凝治疗的变化,但未发现存活率与这些参数相关。在这项针对在重症监护病房接受连续肾脏替代治疗的儿童和年轻人的大型当代流行病学研究中,我们观察到三分之二的患者至少存活到 ICU 出院。然而,患有合并症的患者的预后似乎更差。与之前发表的有关连续肾脏替代治疗实践的报告相比,我们观察到连续静脉血液透析滤过与局部柠檬酸盐抗凝的使用更多。


























 京公网安备 11010802027423号
京公网安备 11010802027423号