PLOS Medicine ( IF 10.5 ) Pub Date : 2017-10-17 , DOI: 10.1371/journal.pmed.1002410 Sanjay Basu , Jeremy B. Sussman , Joseph Rigdon , Lauren Steimle , Brian T. Denton , Rodney A. Hayward
|
Background
Intensive blood pressure (BP) treatment can avert cardiovascular disease (CVD) events but can cause some serious adverse events. We sought to develop and validate risk models for predicting absolute risk difference (increased risk or decreased risk) for CVD events and serious adverse events from intensive BP therapy. A secondary aim was to test if the statistical method of elastic net regularization would improve the estimation of risk models for predicting absolute risk difference, as compared to a traditional backwards variable selection approach.
Methods and findings
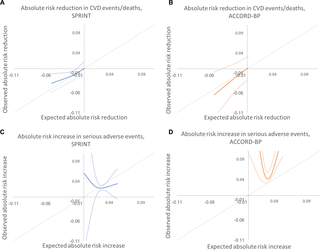
Cox models were derived from SPRINT trial data and validated on ACCORD-BP trial data to estimate risk of CVD events and serious adverse events; the models included terms for intensive BP treatment and heterogeneous response to intensive treatment. The Cox models were then used to estimate the absolute reduction in probability of CVD events (benefit) and absolute increase in probability of serious adverse events (harm) for each individual from intensive treatment. We compared the method of elastic net regularization, which uses repeated internal cross-validation to select variables and estimate coefficients in the presence of collinearity, to a traditional backwards variable selection approach. Data from 9,069 SPRINT participants with complete data on covariates were utilized for model development, and data from 4,498 ACCORD-BP participants with complete data were utilized for model validation. Participants were exposed to intensive (goal systolic pressure < 120 mm Hg) versus standard (<140 mm Hg) treatment. Two composite primary outcome measures were evaluated: (i) CVD events/deaths (myocardial infarction, acute coronary syndrome, stroke, congestive heart failure, or CVD death), and (ii) serious adverse events (hypotension, syncope, electrolyte abnormalities, bradycardia, or acute kidney injury/failure). The model for CVD chosen through elastic net regularization included interaction terms suggesting that older age, black race, higher diastolic BP, and higher lipids were associated with greater CVD risk reduction benefits from intensive treatment, while current smoking was associated with fewer benefits. The model for serious adverse events chosen through elastic net regularization suggested that male sex, current smoking, statin use, elevated creatinine, and higher lipids were associated with greater risk of serious adverse events from intensive treatment. SPRINT participants in the highest predicted benefit subgroup had a number needed to treat (NNT) of 24 to prevent 1 CVD event/death over 5 years (absolute risk reduction [ARR] = 0.042, 95% CI: 0.018, 0.066; P = 0.001), those in the middle predicted benefit subgroup had a NNT of 76 (ARR = 0.013, 95% CI: −0.0001, 0.026; P = 0.053), and those in the lowest subgroup had no significant risk reduction (ARR = 0.006, 95% CI: −0.007, 0.018; P = 0.71). Those in the highest predicted harm subgroup had a number needed to harm (NNH) of 27 to induce 1 serious adverse event (absolute risk increase [ARI] = 0.038, 95% CI: 0.014, 0.061; P = 0.002), those in the middle predicted harm subgroup had a NNH of 41 (ARI = 0.025, 95% CI: 0.012, 0.038; P < 0.001), and those in the lowest subgroup had no significant risk increase (ARI = −0.007, 95% CI: −0.043, 0.030; P = 0.72). In ACCORD-BP, participants in the highest subgroup of predicted benefit had significant absolute CVD risk reduction, but the overall ACCORD-BP participant sample was skewed towards participants with less predicted benefit and more predicted risk than in SPRINT. The models chosen through traditional backwards selection had similar ability to identify absolute risk difference for CVD as the elastic net models, but poorer ability to correctly identify absolute risk difference for serious adverse events. A key limitation of the analysis is the limited sample size of the ACCORD-BP trial, which expanded confidence intervals for ARI among persons with type 2 diabetes. Additionally, it is not possible to mechanistically explain the physiological relationships explaining the heterogeneous treatment effects captured by the models, since the study was an observational secondary data analysis.
Conclusions
We found that predictive models could help identify subgroups of participants in both SPRINT and ACCORD-BP who had lower versus higher ARRs in CVD events/deaths with intensive BP treatment, and participants who had lower versus higher ARIs in serious adverse events.
中文翻译:
强化血压治疗的利弊:使用SPRINT和ACCORD试验的数据推导和验证风险模型
背景
高血压(BP)治疗可以避免心血管疾病(CVD)事件,但可以引起一些严重的不良事件。我们寻求开发和验证风险模型,以预测强化BP治疗引起的CVD事件和严重不良事件的绝对风险差异(风险增加或风险降低)。第二个目的是测试与传统的向后变量选择方法相比,弹性网正则化的统计方法是否可以改善用于预测绝对风险差异的风险模型的估计。
方法和发现
Cox模型来自SPRINT试验数据,并在ACCORD-BP试验数据上进行了验证,以估计CVD事件和严重不良事件的风险。这些模型包括强化治疗的术语和强化治疗的异质性反应。然后,将Cox模型用于评估强化治疗后每个人的CVD事件发生概率的绝对减少(获益)和严重不良事件发生的可能性(危害)的绝对增加。我们将弹性网正则化的方法与传统的向后变量选择方法进行了比较,该方法使用重复的内部交叉验证来选择变量并在存在共线性的情况下估计系数。来自9,069位SPRINT参与者的数据以及有关协变量的完整数据被用于模型开发,而来自4位的数据 498位ACCORD-BP参与者及其完整数据被用于模型验证。与标准治疗(<140 mm Hg)相比,参与者接受了强化治疗(目标收缩压<120 mm Hg)。评价了两种主要的主要结局指标:(i)CVD事件/死亡(心肌梗塞,急性冠状动脉综合征,中风,充血性心力衰竭或CVD死亡),以及(ii)严重不良事件(低血压,晕厥,电解质异常,心动过缓) ,或急性肾损伤/失败)。通过弹性净正则化选择的CVD模型包括相互作用项,这些相互作用表明年龄,黑种人,舒张压较高,血脂较高与强化治疗可带来更大的CVD风险降低收益,而当前吸烟所带来的收益则较少。通过弹性净正则化选择的严重不良事件模型表明,男性,当前吸烟,他汀类药物使用,肌酐升高和血脂升高与强化治疗导致严重不良事件的风险更高相关。预期最高收益亚组中的SPRINT参与者需要治疗的人数(NNT)为24,以在5年内预防1次CVD事件/死亡(绝对风险降低[ARR] = 0.042,95%CI:0.018,0.066;P = 0.001),处于中间预期收益分组的患者的NNT为76(ARR = 0.013,95%CI:-0.0001,0.026; P = 0.053),而处于最低预测分组的患者的NNT没有显着降低风险(ARR = 0.006,95%CI:-0.007,0.018;P= 0.71)。预计危害最高的亚组的人需要伤害(NNH)的数量为27,以诱发1次严重不良事件(绝对风险增加[ARI] = 0.038,95%CI:0.014,0.061; P = 0.002),中等预测伤害亚组的NNH为41(ARI = 0.025,95%CI:0.012,0.038 ; P < 0.001),最低亚组的NNH没有显着风险增加(ARI = -0.007,95%CI:-0.043 ,0.030; P= 0.72)。在ACCORD-BP中,预计收益的最高子组的参与者具有绝对的绝对CVD风险降低,但总的ACCORD-BP参与者样本偏向于预测利益比SPRINT少且预测风险更高的参与者。通过传统的向后选择所选择的模型具有与CVD弹性网模型相似的识别CVD绝对风险差异的能力,但对于严重不良事件的正确识别绝对风险差异的能力较弱。该分析的一个关键限制是ACCORD-BP试验的样本量有限,从而扩大了2型糖尿病患者ARI的置信区间。此外,无法机械地解释生理关系,从而解释模型所捕获的异质治疗效果,
结论
我们发现,预测模型可以帮助识别在强化BP治疗下CVD事件/死亡中ARR较低或较高的SPRINT和ACCORD-BP参与者的亚组,以及在严重不良事件中ARI较低或较高的参与者的亚组。










































 京公网安备 11010802027423号
京公网安备 11010802027423号