JAMA Oncology ( IF 22.5 ) Pub Date : 2018-06-01 , DOI: 10.1001/jamaoncol.2017.3598 Stacie B. Dusetzina 1, 2, 3, 4 , Haiden A. Huskamp 5 , Aaron N. Winn 2 , Ethan Basch 2, 3, 6 , Nancy L. Keating 5, 7
|
Importance Oral anticancer medications are increasingly important but costly treatment options for patients with cancer. By early 2017, 43 states and Washington, DC, had passed laws to ensure patients with private insurance enrolled in fully insured health plans pay no more for anticancer medications administered by mouth than anticancer medications administered by infusion. Federal legislation regarding this issue is currently pending. Despite their rapid acceptance, the changes associated with state adoption of oral chemotherapy parity laws have not been described.
Objective To estimate changes in oral anticancer medication use, out-of-pocket spending, and health plan spending associated with oral chemotherapy parity law adoption.
Design, Setting, and Participants Analysis of administrative health plan claims data from 2008-2012 for 3 large nationwide insurers aggregated by the Health Care Cost Institute. Data analysis was first completed in 2015 and updated in 2017. The study population included 63 780 adults living in 1 of 16 states that passed parity laws during the study period and who received anticancer drug treatment for which orally administered treatment options were available. Study analysis used a difference-in-differences approach.
Exposures Time period before and after adoption of state parity laws, controlling for whether the patient was enrolled in a plan subject to parity (fully insured) or not (self-funded, exempt via the Employee Retirement Income Security Act).
Main Outcomes and Measures Oral anticancer medication use, out-of-pocket spending, and total health care spending.
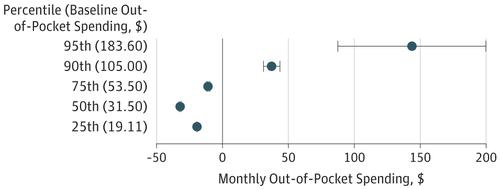
Results Of the 63 780 adults aged 18 through 64 years, 51.4% participated in fully insured plans and 48.6% in self-funded plans (57.2% were women; 76.8% were aged 45 to 64 years). The use of oral anticancer medication treatment as a proportion of all anticancer treatment increased from 18% to 22% (adjusted difference-in-differences risk ratio [aDDRR], 1.04; 95% CI, 0.96-1.13; P = .34) comparing months before vs after parity. In plans subject to parity laws, the proportion of prescription fills for orally administered therapy without copayment increased from 15.0% to 53.0%, more than double the increase (12.3%-18.0%) in plans not subject to parity (P < .001). The proportion of patients with out-of-pocket spending of more than $100 per month increased from 8.4% to 11.1% compared with a slight decline from 12.0% to 11.7% in plans not subject to parity (P = .004). In plans subject to parity laws, estimated monthly out-of-pocket spending decreased by $19.44 at the 25th percentile, by $32.13 at the 50th percentile, and by $10.83 at the 75th percentile but increased at the 90th ($37.19) and 95th ($143.25) percentiles after parity (all P < .001, controlling for changes in plans not subject to parity). Parity laws did not increase 6-month total spending for users of any anticancer therapy or for users of oral anticancer therapy alone.
Conclusions and Relevance While oral chemotherapy parity laws modestly improved financial protection for many patients without increasing total health care spending, these laws alone may be insufficient to ensure that patients are protected from high out-of-pocket medication costs.
中文翻译:
通过国家平价法后采用口服抗癌治疗的患者的自付费用和医疗保健支出变化
重要性 口服抗癌药物对于癌症患者而言日益重要,但治疗方法成本高昂。到2017年初,美国43个州和华盛顿特区已通过法律,确保参加全面保险医疗计划的拥有私人保险的患者为口服抗癌药物支付的费用不会比输液抗癌药物支付的费用高。目前,有关此问题的联邦立法尚待审批。尽管被迅速接受,但尚未描述与国家采用口服化学疗法平价法相关的变化。
目的 评估与采用口服化学疗法平价法相关的口服抗癌药物使用,自付费用和健康计划支出的变化。
设计,制定和参与人 由卫生保健成本研究所汇总的2008年至2012年3家全国性大型保险公司的行政医疗计划理赔数据进行了分析。数据分析于2015年首次完成,并于2017年更新。研究人群包括生活在16个州中的1个州中的63 780名成年人,他们在研究期间通过了同等法律,并且接受了抗癌药物治疗,并且可以口服治疗。研究分析使用差异中差异方法。
暴露 通过州平等法之前和之后的时间段,控制患者是否参加了受平等(完全保险)计划(自筹资金,通过《雇员退休收入保障法》豁免的计划)。
主要结果和措施 口服抗癌药物的使用,自付费用以及医疗保健总支出。
结果 63 780名年龄在18至64岁之间的成年人中,有51.4%参加了全额投保计划,有48.6%参加了自费计划(其中57.2%为妇女; 76.8%为45至64岁)。口服抗癌药物治疗占所有抗癌治疗的比例从18%增加到22%(调整后的差异风险比[aDDRR]为1.04; 95%CI为0.96-1.13;P = 0.34)平价之前或之后的几个月。在遵守同等法律的计划中,无需共付额的口服治疗处方药的比例从15.0%增加到53.0%,是不受到同等医疗的计划所增加的比例(12.3%-18.0%)的两倍以上(P <.001)。每月自付费用超过100美元的患者比例从8.4%增加到11.1%,相比之下,在没有受到均等限制的计划中,其比例从12.0%略微下降到11.7%(P = .004)。在受均等法律约束的计划中,估计的每月实际支出支出在第25个百分位数减少了19.44美元,在第50个百分位数减少了32.13美元,在第75个百分位数减少了10.83美元,但在第90个百分位数(37.19美元)和第95个百分位数(143.25美元)增加了奇偶校验后的百分位数(所有P <0.001,控制不受奇偶校验的计划更改)。均等法律并未增加使用任何抗癌疗法或仅口服抗癌疗法的6个月总支出。
结论和相关性 虽然口服化学疗法均等法在不增加医疗总支出的情况下适度改善了对许多患者的财务保护,但仅靠这些法律可能不足以确保患者免于支付高额的自付费用。









































 京公网安备 11010802027423号
京公网安备 11010802027423号