当前位置:
X-MOL 学术
›
JAMA Pediatr.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Dose, Content, and Mediators of Family-Based Treatment for Childhood Obesity
JAMA Pediatrics ( IF 24.7 ) Pub Date : 2017-12-01 , DOI: 10.1001/jamapediatrics.2017.2960 Denise E Wilfley 1 , Brian E Saelens 2, 3 , Richard I Stein 4 , John R Best 5, 6, 7 , Rachel P Kolko 8 , Kenneth B Schechtman 9 , Michael Wallendorf 9 , R Robinson Welch 10 , Michael G Perri 11 , Leonard H Epstein 12
JAMA Pediatrics ( IF 24.7 ) Pub Date : 2017-12-01 , DOI: 10.1001/jamapediatrics.2017.2960 Denise E Wilfley 1 , Brian E Saelens 2, 3 , Richard I Stein 4 , John R Best 5, 6, 7 , Rachel P Kolko 8 , Kenneth B Schechtman 9 , Michael Wallendorf 9 , R Robinson Welch 10 , Michael G Perri 11 , Leonard H Epstein 12
Affiliation
|
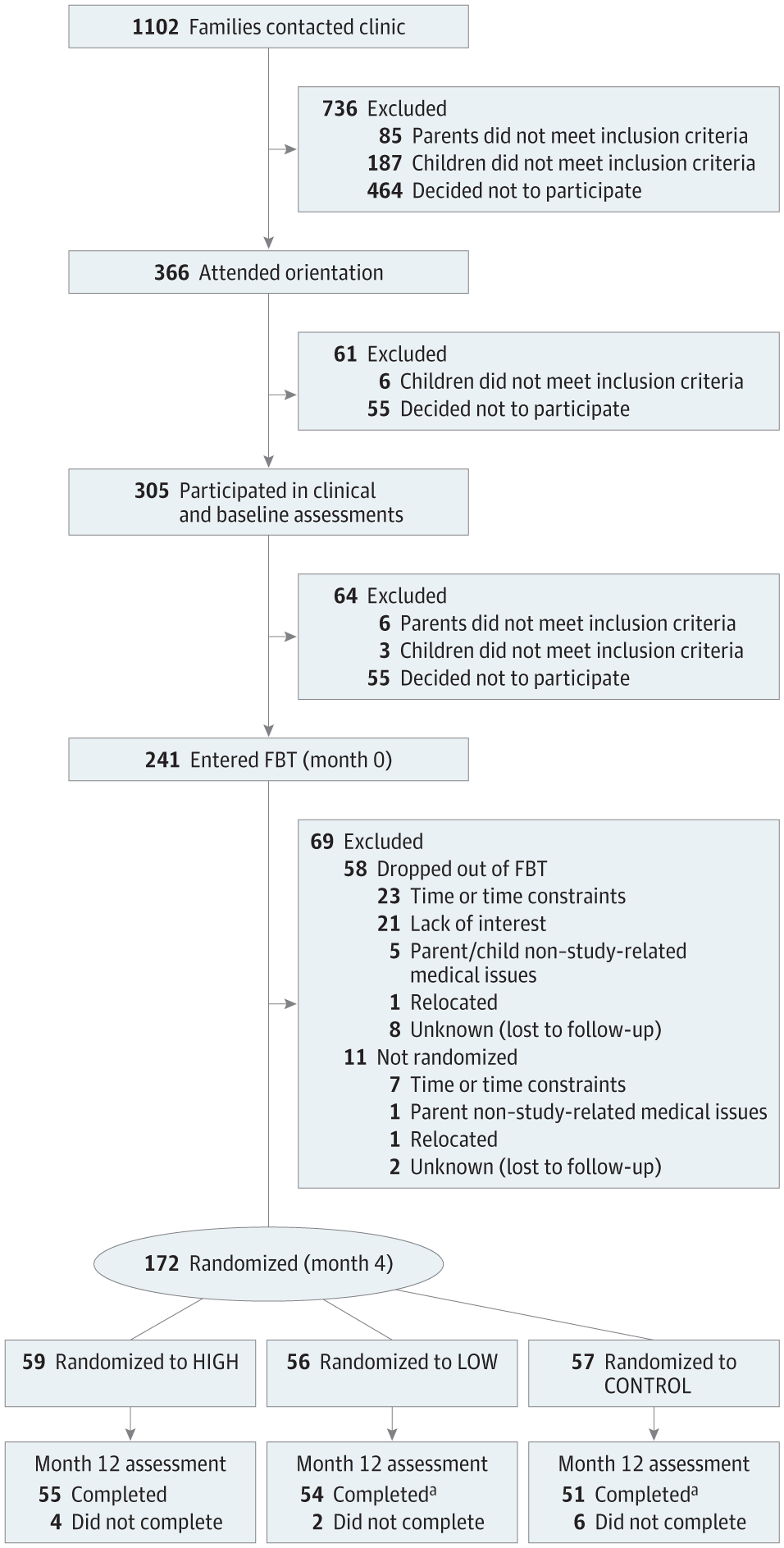
Importance Elucidation of optimal dosing and treatment content is critical for health care providers, payers, and policy makers, as well as mechanisms of change to inform intervention delivery and training initiatives for childhood obesity. Objectives To evaluate effects, following a 4-month family-based behavioral weight loss treatment (FBT), of 2 doses (HIGH or LOW) of a weight-control intervention (enhanced social facilitation maintenance [SFM+]) vs a weight-control education condition (CONTROL; matched for dose with LOW), on child anthropometrics, and to explore putative mediators of weight loss outcomes. Design, Setting, and Participants For this parallel-group randomized clinical trial conducted at 2 US academic medical centers from December 2009 to March 2013, 172 parent-child dyads completed FBT and were then randomized to 8 months of SFM+ (HIGH, n = 59; LOW, n = 56) or CONTROL (n = 57). Children (aged 7-11 years) with overweight and obesity (body mass index [BMI; calculated as weight in kilograms divided by height in meters squared] ≥85th percentile) with at least 1 parent with overweight and obesity (BMI ≥25) were recruited. Interventions HIGH SFM+ vs LOW SFM+ (CONTROL matched the dose of LOW). Main Outcomes and Measures Intention-to-treat analysis using mixed-effects models estimated change in child percentage overweight (percentage above the median BMI for a child's age and sex) for the FBT period (0-4 months) and the SFM+ period (4-12 months), and proportion of children achieving a clinically significant change in percentage overweight (≥9-unit decrease; months 0-12). Theory-based outcome mediators were also evaluated. Results This study recruited 172 parent-child dyads (mean [SD] age: parents 42.3 [6.4] years; children, 9.4 [1.3] years). The omnibus treatment × time interaction for child percentage overweight was significant (F8, 618.9 = 2.89; P = .004). Planned pairwise comparisons revealed that from months 4 to 12, LOW had better outcomes than CONTROL (difference, −3.34; 95% CI, −6.21 to −0.47; d = −0.40; P = .02). HIGH had better outcomes than LOW (difference, −3.37; 95% CI, −6.15 to −0.59; d = −0.38; P = .02) and CONTROL (difference, −6.71; 95% CI, −9.57 to −3.84; d = −0.77; P < .001). A greater proportion of children in HIGH (45 [82%]) vs LOW (34 [64%]) (difference, 18.00; 95% CI, 1.00-34.00; P = .03; number needed to treat = 5.56) and CONTROL (25 [48%]) (difference, 34.00; 95% CI, 16.00-51.00; P < .001; number needed to treat = 2.94) had clinically significant percentage overweight reductions. Food and activity monitoring and goal setting mediated the effect of LOW vs CONTROL (50%). Monitoring and goal setting, family and home environment, and healthy behaviors with peers mediated the effect of HIGH vs CONTROL (25%-42%). Conclusions and Relevance Following FBT, specialized intervention content (SFM+) enhanced children’s weight outcomes and outperformed a credible control condition, with high dose delivery yielding the best outcomes. Sustained monitoring and goal setting, support from the family and home environment, and healthy peer interactions explained outcome differences, highlighting key treatment targets. Trial Registration clinicaltrials.gov Identifier: NCT00759746
中文翻译:

儿童肥胖家庭治疗的剂量、内容和中介因素
重要性 阐明最佳剂量和治疗内容对于卫生保健提供者、付款者和政策制定者以及为儿童肥胖干预措施和培训举措提供信息的变革机制至关重要。目的 评估 4 个月的基于家庭的行为减肥治疗 (FBT) 后,2 剂(高或低)体重控制干预措施(增强社会促进维持 [SFM+])与体重控制教育的效果条件(对照;与低剂量匹配),关于儿童人体测量学,并探索减肥结果的假定中介因素。设计、设置和参与者 这项平行组随机临床试验于 2009 年 12 月至 2013 年 3 月在美国 2 个学术医疗中心进行,172 名亲子夫妇完成了 FBT,然后随机接受 8 个月的 SFM+(高,n = 59) ;低,n = 56)或对照(n = 57)。超重和肥胖儿童(7-11岁)(体重指数[BMI;计算方法为体重公斤数除以身高米平方]≥85%),且至少有一名父母超重和肥胖(BMI≥25)被招募了。干预措施 高 SFM+ 与低 SFM+(对照组与低剂量相匹配)。主要成果和措施 使用混合效应模型进行意向治疗分析,估计 FBT 期(0-4 个月)和 SFM+ 期(4 -12个月),以及超重百分比出现临床显着变化的儿童比例(减少≥9个单位;0-12个月)。还评估了基于理论的结果中介。结果本研究招募了 172 名亲子二人组(平均 [SD] 年龄:父母 42.3 [6.4] 岁;子女 9.4 [1.3] 岁)。 儿童超重百分比的综合治疗 × 时间交互作用显着 (F8, 618.9 = 2.89; P = .004)。计划的成对比较显示,从第 4 个月到第 12 个月,“低”组的结果优于“对照组”(差异,-3.34;95% CI,-6.21 至 -0.47;d = -0.40;P = .02)。 HIGH 的结果优于 LOW(差异,-3.37;95% CI,-6.15 至 -0.59;d = -0.38;P = .02)和 CONTROL(差异,-6.71;95% CI,-9.57 至 -3.84;95% CI,-9.57 至 -3.84; d = -0.77;P < .001)。高 (45 [82%]) 儿童比例高于低 (34 [64%])(差异,18.00;95% CI,1.00-34.00;P = .03;需要治疗的人数 = 5.56)和对照组(25 [48%])(差异,34.00;95% CI,16.00-51.00;P < .001;需要治疗的人数 = 2.94)具有临床显着的超重百分比减少。食物和活动监测以及目标设定介导了“低”与“控制”的影响(50%)。监控和目标设定、家庭和家庭环境以及与同伴的健康行为介导了“高”与“控制”的影响(25%-42%)。结论和相关性 FBT 后,专门的干预内容 (SFM+) 改善了儿童的体重结果,并优于可靠的控制条件,高剂量给药可产生最佳结果。持续的监测和目标设定、家庭和家庭环境的支持以及健康的同伴互动解释了结果差异,突出了关键的治疗目标。试验注册临床试验。政府标识符:NCT00759746
更新日期:2017-12-01
中文翻译:
儿童肥胖家庭治疗的剂量、内容和中介因素
重要性 阐明最佳剂量和治疗内容对于卫生保健提供者、付款者和政策制定者以及为儿童肥胖干预措施和培训举措提供信息的变革机制至关重要。目的 评估 4 个月的基于家庭的行为减肥治疗 (FBT) 后,2 剂(高或低)体重控制干预措施(增强社会促进维持 [SFM+])与体重控制教育的效果条件(对照;与低剂量匹配),关于儿童人体测量学,并探索减肥结果的假定中介因素。设计、设置和参与者 这项平行组随机临床试验于 2009 年 12 月至 2013 年 3 月在美国 2 个学术医疗中心进行,172 名亲子夫妇完成了 FBT,然后随机接受 8 个月的 SFM+(高,n = 59) ;低,n = 56)或对照(n = 57)。超重和肥胖儿童(7-11岁)(体重指数[BMI;计算方法为体重公斤数除以身高米平方]≥85%),且至少有一名父母超重和肥胖(BMI≥25)被招募了。干预措施 高 SFM+ 与低 SFM+(对照组与低剂量相匹配)。主要成果和措施 使用混合效应模型进行意向治疗分析,估计 FBT 期(0-4 个月)和 SFM+ 期(4 -12个月),以及超重百分比出现临床显着变化的儿童比例(减少≥9个单位;0-12个月)。还评估了基于理论的结果中介。结果本研究招募了 172 名亲子二人组(平均 [SD] 年龄:父母 42.3 [6.4] 岁;子女 9.4 [1.3] 岁)。 儿童超重百分比的综合治疗 × 时间交互作用显着 (F8, 618.9 = 2.89; P = .004)。计划的成对比较显示,从第 4 个月到第 12 个月,“低”组的结果优于“对照组”(差异,-3.34;95% CI,-6.21 至 -0.47;d = -0.40;P = .02)。 HIGH 的结果优于 LOW(差异,-3.37;95% CI,-6.15 至 -0.59;d = -0.38;P = .02)和 CONTROL(差异,-6.71;95% CI,-9.57 至 -3.84;95% CI,-9.57 至 -3.84; d = -0.77;P < .001)。高 (45 [82%]) 儿童比例高于低 (34 [64%])(差异,18.00;95% CI,1.00-34.00;P = .03;需要治疗的人数 = 5.56)和对照组(25 [48%])(差异,34.00;95% CI,16.00-51.00;P < .001;需要治疗的人数 = 2.94)具有临床显着的超重百分比减少。食物和活动监测以及目标设定介导了“低”与“控制”的影响(50%)。监控和目标设定、家庭和家庭环境以及与同伴的健康行为介导了“高”与“控制”的影响(25%-42%)。结论和相关性 FBT 后,专门的干预内容 (SFM+) 改善了儿童的体重结果,并优于可靠的控制条件,高剂量给药可产生最佳结果。持续的监测和目标设定、家庭和家庭环境的支持以及健康的同伴互动解释了结果差异,突出了关键的治疗目标。试验注册临床试验。政府标识符:NCT00759746










































 京公网安备 11010802027423号
京公网安备 11010802027423号