当前位置:
X-MOL 学术
›
J. Am. Coll. Cardiol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Lesion Complexity and Outcomes of Extended Dual Antiplatelet Therapy After Percutaneous Coronary Intervention
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2017-10-01 , DOI: 10.1016/j.jacc.2017.09.011 Robert W. Yeh , Dean J. Kereiakes , P. Gabriel Steg , Donald E. Cutlip , Kevin J. Croce , Joseph M. Massaro , Laura Mauri
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2017-10-01 , DOI: 10.1016/j.jacc.2017.09.011 Robert W. Yeh , Dean J. Kereiakes , P. Gabriel Steg , Donald E. Cutlip , Kevin J. Croce , Joseph M. Massaro , Laura Mauri
|
BACKGROUND
Subjects undergoing coronary stenting with complex lesion anatomy may experience different risks and benefits with prolonged dual antiplatelet therapy. OBJECTIVES
The authors assessed the effect of 30 months versus 12 months of dual antiplatelet therapy (DAPT) after percutaneous coronary intervention (PCI) based on the presence or absence of anatomically-complex target lesions. METHODS
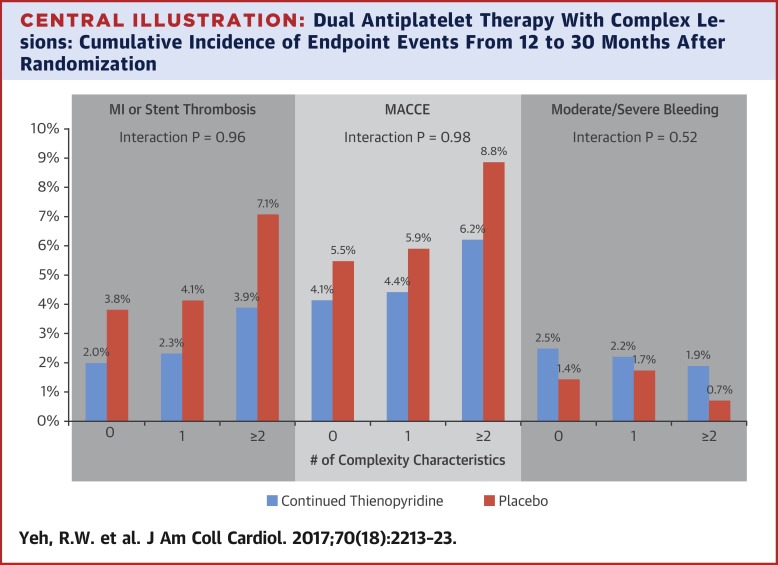
In the DAPT Study, combined myocardial infarction (MI) or stent thrombosis and moderate/severe bleeding were assessed in enrolled (n = 25,416) and randomized (n = 11,554) subjects. Complex lesions had any of the following characteristics: unprotected left main, >2 lesions/vessel, length ≥30 mm, bifurcation with side branch ≥2.5 mm, vein bypass graft, or thrombus-containing lesion. Events were evaluated according to increasing number of complexity characteristics and compared according to DAPT score. RESULTS
Enrolled subjects with more complex target lesions had higher rates of MI or stent thrombosis in the first 12 months after PCI (3.9% vs. 2.4%; p < 0.001). Among those who were event-free at 12 months, rates of MI or stent thrombosis between 12 and 30 months were similar between those with versus without complex anatomy (3.5% vs. 2.9%; p = 0.07). Reduction of MI or stent thrombosis with continued thienopyridine beyond 12 months versus placebo was similar for subjects with (2.5% vs. 4.5%; hazard ratio: 0.55; 95% confidence interval: 0.38 to 0.79; p = 0.001) and without (2.0% vs. 3.8%; hazard ratio: 0.52; 95% confidence interval: 0.39 to 0.69; p < 0.001) anatomic complexity (pinteraction = 0.81), as was increase in moderate/severe bleeding (pinteraction = 0.44). Among subjects with anatomic complexity, those with DAPT scores ≥2 randomized to continued thienopyridine had greater reductions in MI or stent thrombosis (3.0% vs. 6.1%; p < 0.001) compared with subjects with scores <2 (1.7% vs. 2.3%; p = 0.42; p value comparing risk differences = 0.03). CONCLUSIONS
Complex target-lesion anatomy is associated with increased ischemic events, particularly within the first year after PCI. Among those without events in the first 12 months, the benefits of extending DAPT were similar in subjects with and without complex lesions. A high DAPT score identified those experiencing the most benefit from extended treatment among patients with and without complex anatomy. (The Dual Antiplatelet Therapy Study [DAPT Study]; NCT00977938).
中文翻译:

经皮冠状动脉介入治疗后延长双重抗血小板治疗的病变复杂性和结果
背景 接受冠状动脉支架植入术且病变解剖结构复杂的受试者可能会经历长期双重抗血小板治疗的不同风险和益处。目的 作者根据解剖复杂的靶病变的存在与否,评估了经皮冠状动脉介入治疗 (PCI) 后 30 个月与 12 个月双重抗血小板治疗 (DAPT) 的效果。方法 在 DAPT 研究中,对纳入 (n = 25,416) 和随机 (n = 11,554) 受试者的合并心肌梗死 (MI) 或支架血栓形成和中/重度出血进行了评估。复杂病变具有以下任何特征:无保护的左主干,>2个病变/血管,长度≥30 mm,分叉侧支≥2.5 mm,静脉旁路移植或含血栓病变。根据复杂性特征数量的增加对事件进行评估,并根据 DAPT 评分进行比较。结果 在 PCI 后的前 12 个月内,目标病变更复杂的入选受试者的 MI 或支架血栓形成率更高(3.9% 对 2.4%;p < 0.001)。在 12 个月时无事件的患者中,12 至 30 个月期间 MI 或支架内血栓形成的发生率在解剖结构复杂的患者与非解剖结构复杂的患者之间相似(3.5% 对 2.9%;p = 0.07)。对于以下受试者(2.5% 对 4.5%;风险比:0.55;95% 置信区间:0.38 至 0.79;p = 0.001)和不使用(2.0%对比 3.8%;风险比:0.52;95% 置信区间:0.39 到 0.69;p < 0.001)解剖复杂性(pinteraction = 0.81),中度/重度出血的增加也是如此(pinteraction = 0.44)。在解剖复杂的受试者中,DAPT 评分≥2 的受试者随机接受持续噻吩并吡啶治疗,与评分 <2 的受试者(1.7% 对 2.3%)相比,MI 或支架内血栓形成的减少幅度更大(3.0% 对 6.1%;p < 0.001) ;p = 0.42;比较风险差异的 p 值 = 0.03)。结论 复杂的靶病变解剖结构与缺血事件增加有关,尤其是在 PCI 后的第一年内。在前 12 个月内没有发生事件的患者中,延长 DAPT 的益处在有和没有复杂病变的受试者中相似。高 DAPT 评分确定了那些在有和没有复杂解剖结构的患者中从延长治疗中获益最多的人。(双重抗血小板治疗研究 [DAPT 研究];NCT00977938)。
更新日期:2017-10-01
中文翻译:
经皮冠状动脉介入治疗后延长双重抗血小板治疗的病变复杂性和结果
背景 接受冠状动脉支架植入术且病变解剖结构复杂的受试者可能会经历长期双重抗血小板治疗的不同风险和益处。目的 作者根据解剖复杂的靶病变的存在与否,评估了经皮冠状动脉介入治疗 (PCI) 后 30 个月与 12 个月双重抗血小板治疗 (DAPT) 的效果。方法 在 DAPT 研究中,对纳入 (n = 25,416) 和随机 (n = 11,554) 受试者的合并心肌梗死 (MI) 或支架血栓形成和中/重度出血进行了评估。复杂病变具有以下任何特征:无保护的左主干,>2个病变/血管,长度≥30 mm,分叉侧支≥2.5 mm,静脉旁路移植或含血栓病变。根据复杂性特征数量的增加对事件进行评估,并根据 DAPT 评分进行比较。结果 在 PCI 后的前 12 个月内,目标病变更复杂的入选受试者的 MI 或支架血栓形成率更高(3.9% 对 2.4%;p < 0.001)。在 12 个月时无事件的患者中,12 至 30 个月期间 MI 或支架内血栓形成的发生率在解剖结构复杂的患者与非解剖结构复杂的患者之间相似(3.5% 对 2.9%;p = 0.07)。对于以下受试者(2.5% 对 4.5%;风险比:0.55;95% 置信区间:0.38 至 0.79;p = 0.001)和不使用(2.0%对比 3.8%;风险比:0.52;95% 置信区间:0.39 到 0.69;p < 0.001)解剖复杂性(pinteraction = 0.81),中度/重度出血的增加也是如此(pinteraction = 0.44)。在解剖复杂的受试者中,DAPT 评分≥2 的受试者随机接受持续噻吩并吡啶治疗,与评分 <2 的受试者(1.7% 对 2.3%)相比,MI 或支架内血栓形成的减少幅度更大(3.0% 对 6.1%;p < 0.001) ;p = 0.42;比较风险差异的 p 值 = 0.03)。结论 复杂的靶病变解剖结构与缺血事件增加有关,尤其是在 PCI 后的第一年内。在前 12 个月内没有发生事件的患者中,延长 DAPT 的益处在有和没有复杂病变的受试者中相似。高 DAPT 评分确定了那些在有和没有复杂解剖结构的患者中从延长治疗中获益最多的人。(双重抗血小板治疗研究 [DAPT 研究];NCT00977938)。










































 京公网安备 11010802027423号
京公网安备 11010802027423号