JAMA Oncology ( IF 22.5 ) Pub Date : 2017-09-01 , DOI: 10.1001/jamaoncol.2017.0223 Birke Bausch 1 , Francesca Schiavi 2 , Ying Ni 3 , Jenny Welander 4 , Attila Patocs 5, 6 , Joanne Ngeow 7 , Ulrich Wellner 8 , Angelica Malinoc 9 , Elisa Taschin 2 , Giovanni Barbon 2 , Virginia Lanza 2 , Peter Söderkvist 4 , Adam Stenman 10 , Catharina Larsson 10 , Fredrika Svahn 10 , Jin-Lian Chen 3 , Jessica Marquard 3 , Merav Fraenkel 11 , Martin A Walter 12 , Mariola Peczkowska 13 , Aleksander Prejbisz 13 , Barbara Jarzab 14 , Kornelia Hasse-Lazar 14 , Stephan Petersenn 15 , Lars C Moeller 16 , Almuth Meyer 17 , Nicole Reisch 18 , Arnold Trupka 19 , Christoph Brase 20 , Matthias Galiano 21 , Simon F Preuss 22 , Pingling Kwok 23 , Nikoletta Lendvai 6 , Gani Berisha 9 , Özer Makay 24 , Carsten C Boedeker 25 , Georges Weryha 26 , Karoly Racz 5 , Andrzej Januszewicz 13 , Martin K Walz 27 , Oliver Gimm 4, 28 , Giuseppe Opocher 2 , Charis Eng 29 , Hartmut P H Neumann 30 ,
|
Importance Effective cancer prevention is based on accurate molecular diagnosis and results of genetic family screening, genotype-informed risk assessment, and tailored strategies for early diagnosis. The expanding etiology for hereditary pheochromocytomas and paragangliomas has recently included SDHA, TMEM127, MAX, and SDHAF2 as susceptibility genes. Clinical management guidelines for patients with germline mutations in these 4 newly included genes are lacking.
Objective To study the clinical spectra and age-related penetrance of individuals with mutations in the SDHA, TMEM127, MAX, and SDHAF2 genes.
Design, Setting, and Patients This study analyzed the prospective, longitudinally followed up European-American-Asian Pheochromocytoma-Paraganglioma Registry for prevalence of SDHA, TMEM127, MAX, and SDHAF2 germline mutation carriers from 1993 to 2016. Genetic predictive testing and clinical investigation by imaging from neck to pelvis was offered to mutation-positive registrants and their relatives to clinically characterize the pheochromocytoma/paraganglioma diseases associated with mutations of the 4 new genes.
Main Outcomes and Measures Prevalence and spectra of germline mutations in the SDHA, TMEM127, MAX, and SDHAF2 genes were assessed. The clinical features of SDHA, TMEM127, MAX, and SDHAF2 disease were characterized.
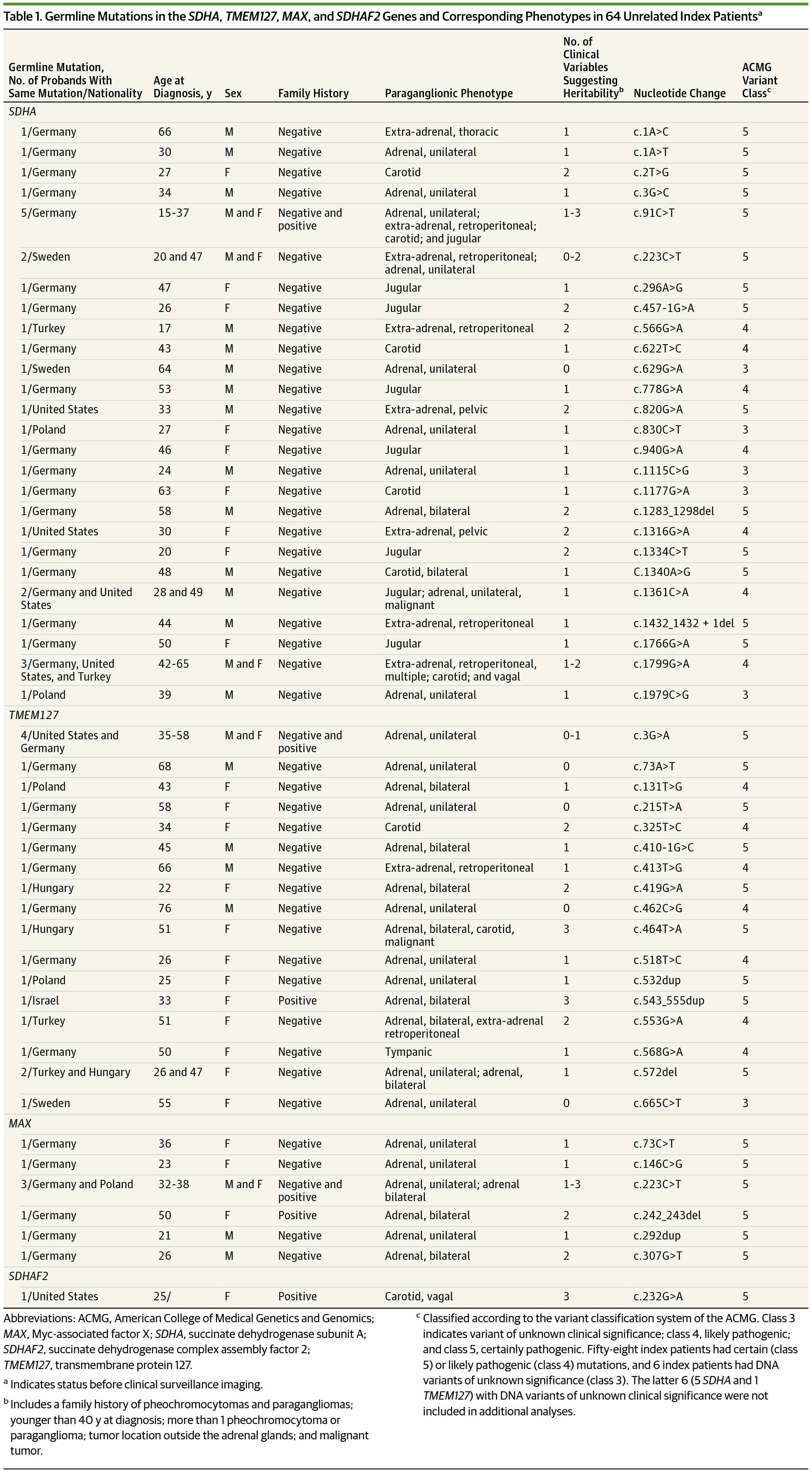
Results Of 972 unrelated registrants without mutations in the classic pheochromocytoma- and paraganglioma-associated genes (632 female [65.0%] and 340 male [35.0%]; age range, 8-80; mean [SD] age, 41.0 [13.3] years), 58 (6.0%) carried germline mutations of interest, including 29 SDHA, 20 TMEM127, 8 MAX, and 1 SDHAF2. Fifty-three of 58 patients (91%) had familial, multiple, extra-adrenal, and/or malignant tumors and/or were younger than 40 years. Newly uncovered are 7 of 63 (11%) malignant pheochromocytomas and paragangliomas in SDHA and TMEM127 disease. SDHA disease occurred as early as 8 years of age. Extra-adrenal tumors occurred in 28 mutation carriers (48%) and in 23 of 29 SDHA mutation carriers (79%), particularly with head and neck paraganglioma. MAX disease occurred almost exclusively in the adrenal glands with frequently bilateral tumors. Penetrance in the largest subset, SDHA carriers, was 39% at 40 years of age and is statistically different in index patients (45%) vs mutation-carrying relatives (13%; P < .001).
Conclusions and Relevance The SDHA, TMEM127, MAX, and SDHAF2 genes may contribute to hereditary pheochromocytoma and paraganglioma. Genetic testing is recommended in patients at clinically high risk if the classic genes are mutation negative. Gene-specific prevention and/or early detection requires regular, systematic whole-body investigation.
中文翻译:
用于基因知情预防的嗜铬细胞瘤和副神经节瘤易感基因 SDHA、TMEM127、MAX 和 SDHAF2 的临床特征
重要性 有效的癌症预防基于准确的分子诊断和遗传家族筛查结果、基于基因型的风险评估以及为早期诊断量身定制的策略。遗传性嗜铬细胞瘤和副神经节瘤的病因不断扩大,最近包括SDHA、TMEM127、MAX和SDHAF2作为易感基因。缺乏针对这 4 个新纳入基因的种系突变患者的临床管理指南。
目的 研究SDHA、TMEM127、MAX和SDHAF2基因突变个体的临床谱和年龄相关外显率。
设计、设置和患者本研究分析了 1993 年至 2016 年SDHA、TMEM127、MAX和SDHAF2种系突变携带者的前瞻性、纵向随访的欧洲-美国-亚洲嗜铬细胞瘤-副神经节瘤登记处的患病率。基因预测测试和临床调查由向突变阳性登记者及其亲属提供从颈部到骨盆的成像,以临床表征与 4 个新基因突变相关的嗜铬细胞瘤/副神经节瘤疾病。
主要结果和措施 评估了 SDHA、TMEM127、MAX和SDHAF2基因种系突变的患病率和谱。对SDHA、TMEM127、MAX和SDHAF2疾病的临床特征进行了表征。
结果 972 名无典型嗜铬细胞瘤和副神经节瘤相关基因突变的无关登记者(632 名女性 [65.0%] 和 340 名男性 [35.0%];年龄范围,8-80 岁;平均 [SD] 年龄,41.0 [13.3] 岁) ),58 个 (6.0%) 携带感兴趣的种系突变,包括 29个 SDHA、 20 个TMEM127、8个MAX和 1 个SDHAF2。58 名患者中有 53 名 (91%) 患有家族性、多发性、肾上腺外和/或恶性肿瘤和/或年龄小于 40 岁。新发现的是SDHA和TMEM127疾病中的 63 例 (11%) 恶性嗜铬细胞瘤和副神经节瘤中的7 例。SDHA该病早在8岁时就发生了。28 名突变携带者(48%)和 29名 SDHA突变携带者中的 23 名(79%)发生肾上腺外肿瘤,尤其是头颈部副神经节瘤。MAX病几乎只发生在肾上腺,常伴有双侧肿瘤。最大子集SDHA携带者的外显率在 40 岁时为 39%,并且在指数患者 (45%) 与携带突变的亲属 (13%; P < .001) 中存在统计学差异。
结论和相关性 SDHA 、 TMEM127 、MAX和SDHAF2基因可能与遗传性嗜铬细胞瘤和副神经节瘤有关。如果经典基因突变阴性,建议对临床高危患者进行基因检测。基因特异性预防和/或早期检测需要定期、系统的全身调查。










































 京公网安备 11010802027423号
京公网安备 11010802027423号