Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Incidence and Trends of Sepsis in US Hospitals Using Clinical vs Claims Data, 2009-2014
JAMA ( IF 63.1 ) Pub Date : 2017-10-03 , DOI: 10.1001/jama.2017.13836 Chanu Rhee 1 , Raymund Dantes 2 , Lauren Epstein 3 , David J. Murphy 4 , Christopher W. Seymour 5 , Theodore J. Iwashyna 6 , Sameer S. Kadri 7 , Derek C. Angus 8 , Robert L. Danner 7 , Anthony E. Fiore 3 , John A. Jernigan 3 , Greg S. Martin 4 , Edward Septimus 9 , David K. Warren 10 , Anita Karcz 11 , Christina Chan 12 , John T. Menchaca 12 , Rui Wang 12 , Susan Gruber 12 , Michael Klompas 1 ,
JAMA ( IF 63.1 ) Pub Date : 2017-10-03 , DOI: 10.1001/jama.2017.13836 Chanu Rhee 1 , Raymund Dantes 2 , Lauren Epstein 3 , David J. Murphy 4 , Christopher W. Seymour 5 , Theodore J. Iwashyna 6 , Sameer S. Kadri 7 , Derek C. Angus 8 , Robert L. Danner 7 , Anthony E. Fiore 3 , John A. Jernigan 3 , Greg S. Martin 4 , Edward Septimus 9 , David K. Warren 10 , Anita Karcz 11 , Christina Chan 12 , John T. Menchaca 12 , Rui Wang 12 , Susan Gruber 12 , Michael Klompas 1 ,
Affiliation
|
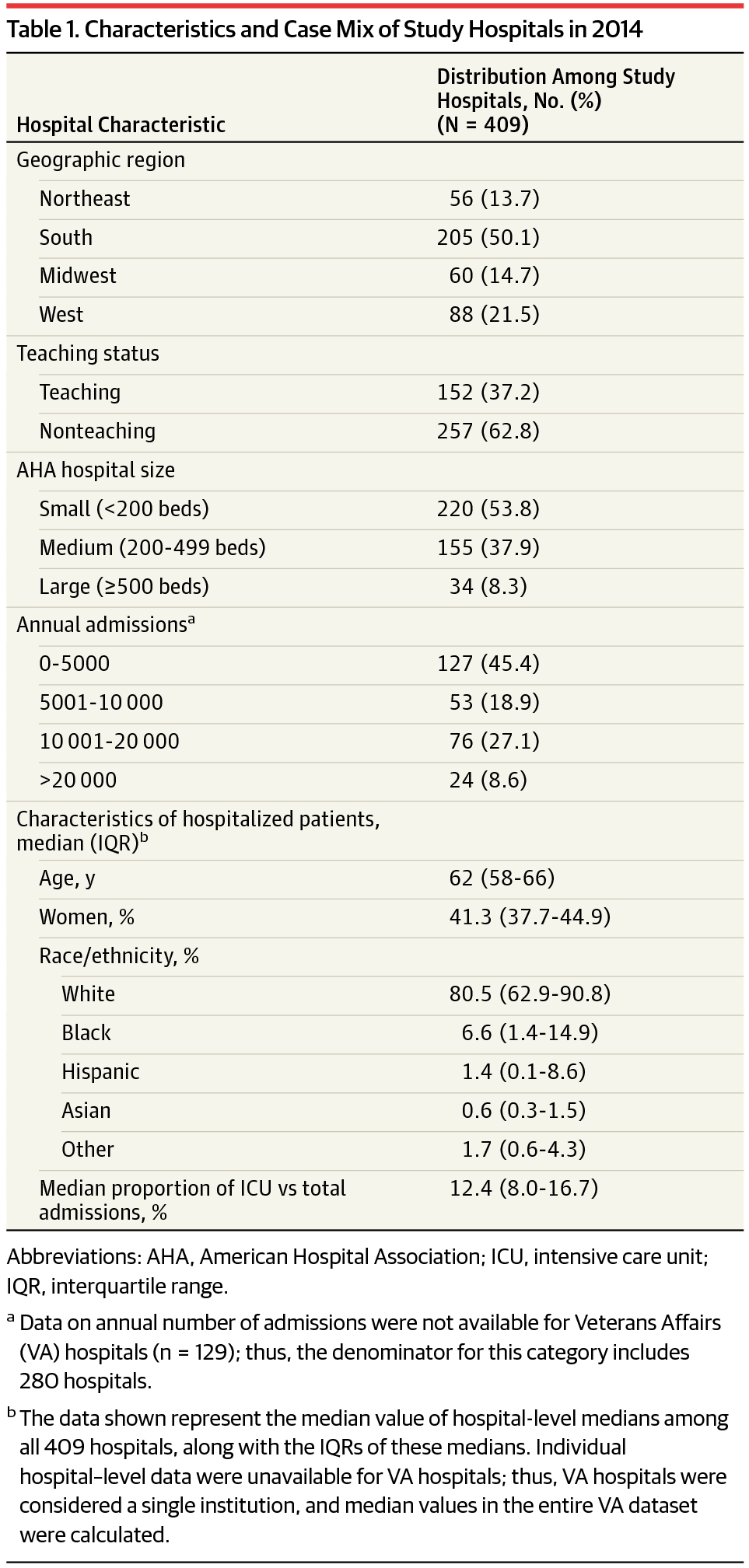
Importance Estimates from claims-based analyses suggest that the incidence of sepsis is increasing and mortality rates from sepsis are decreasing. However, estimates from claims data may lack clinical fidelity and can be affected by changing diagnosis and coding practices over time. Objective To estimate the US national incidence of sepsis and trends using detailed clinical data from the electronic health record (EHR) systems of diverse hospitals. Design, Setting, and Population Retrospective cohort study of adult patients admitted to 409 academic, community, and federal hospitals from 2009-2014. Exposures Sepsis was identified using clinical indicators of presumed infection and concurrent acute organ dysfunction, adapting Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) criteria for objective and consistent EHR-based surveillance. Main Outcomes and Measures Sepsis incidence, outcomes, and trends from 2009-2014 were calculated using regression models and compared with claims-based estimates using International Classification of Diseases, Ninth Revision, Clinical Modification codes for severe sepsis or septic shock. Case-finding criteria were validated against Sepsis-3 criteria using medical record reviews. Results A total of 173 690 sepsis cases (mean age, 66.5 [SD, 15.5] y; 77 660 [42.4%] women) were identified using clinical criteria among 2 901 019 adults admitted to study hospitals in 2014 (6.0% incidence). Of these, 26 061 (15.0%) died in the hospital and 10 731 (6.2%) were discharged to hospice. From 2009-2014, sepsis incidence using clinical criteria was stable (+0.6% relative change/y [95% CI, −2.3% to 3.5%], P = .67) whereas incidence per claims increased (+10.3%/y [95% CI, 7.2% to 13.3%], P < .001). In-hospital mortality using clinical criteria declined (−3.3%/y [95% CI, −5.6% to −1.0%], P = .004), but there was no significant change in the combined outcome of death or discharge to hospice (−1.3%/y [95% CI, −3.2% to 0.6%], P = .19). In contrast, mortality using claims declined significantly (−7.0%/y [95% CI, −8.8% to −5.2%], P < .001), as did death or discharge to hospice (−4.5%/y [95% CI, −6.1% to −2.8%], P < .001). Clinical criteria were more sensitive in identifying sepsis than claims (69.7% [95% CI, 52.9% to 92.0%] vs 32.3% [95% CI, 24.4% to 43.0%], P < .001), with comparable positive predictive value (70.4% [95% CI, 64.0% to 76.8%] vs 75.2% [95% CI, 69.8% to 80.6%], P = .23). Conclusions and Relevance In clinical data from 409 hospitals, sepsis was present in 6% of adult hospitalizations, and in contrast to claims-based analyses, neither the incidence of sepsis nor the combined outcome of death or discharge to hospice changed significantly between 2009-2014. The findings also suggest that EHR-based clinical data provide more objective estimates than claims-based data for sepsis surveillance.
中文翻译:

使用 2009-2014 年临床与索赔数据的美国医院脓毒症的发生率和趋势
重要性 基于索赔的分析估计表明,败血症的发病率正在增加,败血症的死亡率正在下降。然而,索赔数据的估计可能缺乏临床保真度,并且可能会随着时间的推移而改变诊断和编码实践。目的 使用来自不同医院的电子健康记录 (EHR) 系统的详细临床数据估计美国全国败血症的发病率和趋势。2009 年至 2014 年在 409 家学术、社区和联邦医院收治的成年患者的设计、设置和人群回顾性队列研究。暴露 使用假定感染和并发急性器官功能障碍的临床指标确定脓毒症,调整第三国际败血症和败血性休克 (Sepsis-3) 标准的共识定义,以进行客观和一致的基于 EHR 的监测。主要结果和指标 2009-2014 年脓毒症发病率、结果和趋势使用回归模型计算,并与使用国际疾病分类、第九次修订、严重脓毒症或脓毒性休克临床修改代码的基于索赔的估计值进行比较。使用病历审查根据 Sepsis-3 标准验证病例发现标准。结果 在 2014 年入院研究医院的 2 901 019 名成人(发病率为 6.0%)中,使用临床标准共确定了 173 690 例败血症病例(平均年龄,66.5 [SD,15.5] 岁;77 660 [42.4%] 名女性)。其中,26061 人(15.0%)在医院死亡,10731 人(6.2%)出院到临终关怀医院。从 2009 年到 2014 年,使用临床标准的败血症发生率稳定(+0.6% 相对变化/年 [95% CI,-2.3% 至 3.5%],P = .67),而每次索赔的发生率增加(+10.3%/年 [95% CI,7.2 % 到 13.3%],P < .001)。使用临床标准的院内死亡率下降(-3.3%/年 [95% CI,-5.6% 至 -1.0%],P = .004),但死亡或出院到临终关怀的综合结果没有显着变化(-1.3%/年 [95% CI,-3.2% 至 0.6%],P = .19)。相比之下,使用索赔的死亡率显着下降(-7.0%/y [95% CI,-8.8% 至 -5.2%],P < .001),死亡或出院至临终关怀(-4.5%/y [95% CI,-6.1% 至 -2.8%],P < .001)。临床标准在鉴别脓毒症方面比索赔更敏感(69.7% [95% CI,52.9% 至 92.0%] vs 32.3% [95% CI,24.4% 至 43.0%],P < .001),具有可比的阳性预测值(70.4% [95% CI,64.0% 至 76。8%] vs 75.2% [95% CI,69.8% 到 80.6%],P = .23)。结论和相关性 在 409 家医院的临床数据中,6% 的成人住院患者存在败血症,与基于索赔的分析相比,2009 年至 2014 年间败血症的发生率以及死亡或出院的综合结果均未发生显着变化. 研究结果还表明,对于败血症监测,基于 EHR 的临床数据比基于索赔的数据提供了更客观的估计。
更新日期:2017-10-03
中文翻译:
使用 2009-2014 年临床与索赔数据的美国医院脓毒症的发生率和趋势
重要性 基于索赔的分析估计表明,败血症的发病率正在增加,败血症的死亡率正在下降。然而,索赔数据的估计可能缺乏临床保真度,并且可能会随着时间的推移而改变诊断和编码实践。目的 使用来自不同医院的电子健康记录 (EHR) 系统的详细临床数据估计美国全国败血症的发病率和趋势。2009 年至 2014 年在 409 家学术、社区和联邦医院收治的成年患者的设计、设置和人群回顾性队列研究。暴露 使用假定感染和并发急性器官功能障碍的临床指标确定脓毒症,调整第三国际败血症和败血性休克 (Sepsis-3) 标准的共识定义,以进行客观和一致的基于 EHR 的监测。主要结果和指标 2009-2014 年脓毒症发病率、结果和趋势使用回归模型计算,并与使用国际疾病分类、第九次修订、严重脓毒症或脓毒性休克临床修改代码的基于索赔的估计值进行比较。使用病历审查根据 Sepsis-3 标准验证病例发现标准。结果 在 2014 年入院研究医院的 2 901 019 名成人(发病率为 6.0%)中,使用临床标准共确定了 173 690 例败血症病例(平均年龄,66.5 [SD,15.5] 岁;77 660 [42.4%] 名女性)。其中,26061 人(15.0%)在医院死亡,10731 人(6.2%)出院到临终关怀医院。从 2009 年到 2014 年,使用临床标准的败血症发生率稳定(+0.6% 相对变化/年 [95% CI,-2.3% 至 3.5%],P = .67),而每次索赔的发生率增加(+10.3%/年 [95% CI,7.2 % 到 13.3%],P < .001)。使用临床标准的院内死亡率下降(-3.3%/年 [95% CI,-5.6% 至 -1.0%],P = .004),但死亡或出院到临终关怀的综合结果没有显着变化(-1.3%/年 [95% CI,-3.2% 至 0.6%],P = .19)。相比之下,使用索赔的死亡率显着下降(-7.0%/y [95% CI,-8.8% 至 -5.2%],P < .001),死亡或出院至临终关怀(-4.5%/y [95% CI,-6.1% 至 -2.8%],P < .001)。临床标准在鉴别脓毒症方面比索赔更敏感(69.7% [95% CI,52.9% 至 92.0%] vs 32.3% [95% CI,24.4% 至 43.0%],P < .001),具有可比的阳性预测值(70.4% [95% CI,64.0% 至 76。8%] vs 75.2% [95% CI,69.8% 到 80.6%],P = .23)。结论和相关性 在 409 家医院的临床数据中,6% 的成人住院患者存在败血症,与基于索赔的分析相比,2009 年至 2014 年间败血症的发生率以及死亡或出院的综合结果均未发生显着变化. 研究结果还表明,对于败血症监测,基于 EHR 的临床数据比基于索赔的数据提供了更客观的估计。










































 京公网安备 11010802027423号
京公网安备 11010802027423号