JAMA Psychiatry ( IF 22.5 ) Pub Date : 2017-09-01 , DOI: 10.1001/jamapsychiatry.2017.1847 Bastian Ravesteijn 1 , Eli B. Schachar 2 , Aartjan T. F. Beekman 3 , Richard T. J. M. Janssen 4 , Patrick P. T. Jeurissen 5
|
Importance A higher out-of-pocket price for mental health care may lead not only to cost savings but also to negative downstream consequences.
Objective To examine the association of higher patient cost sharing with mental health care use and downstream effects, such as involuntary commitment and acute mental health care use.
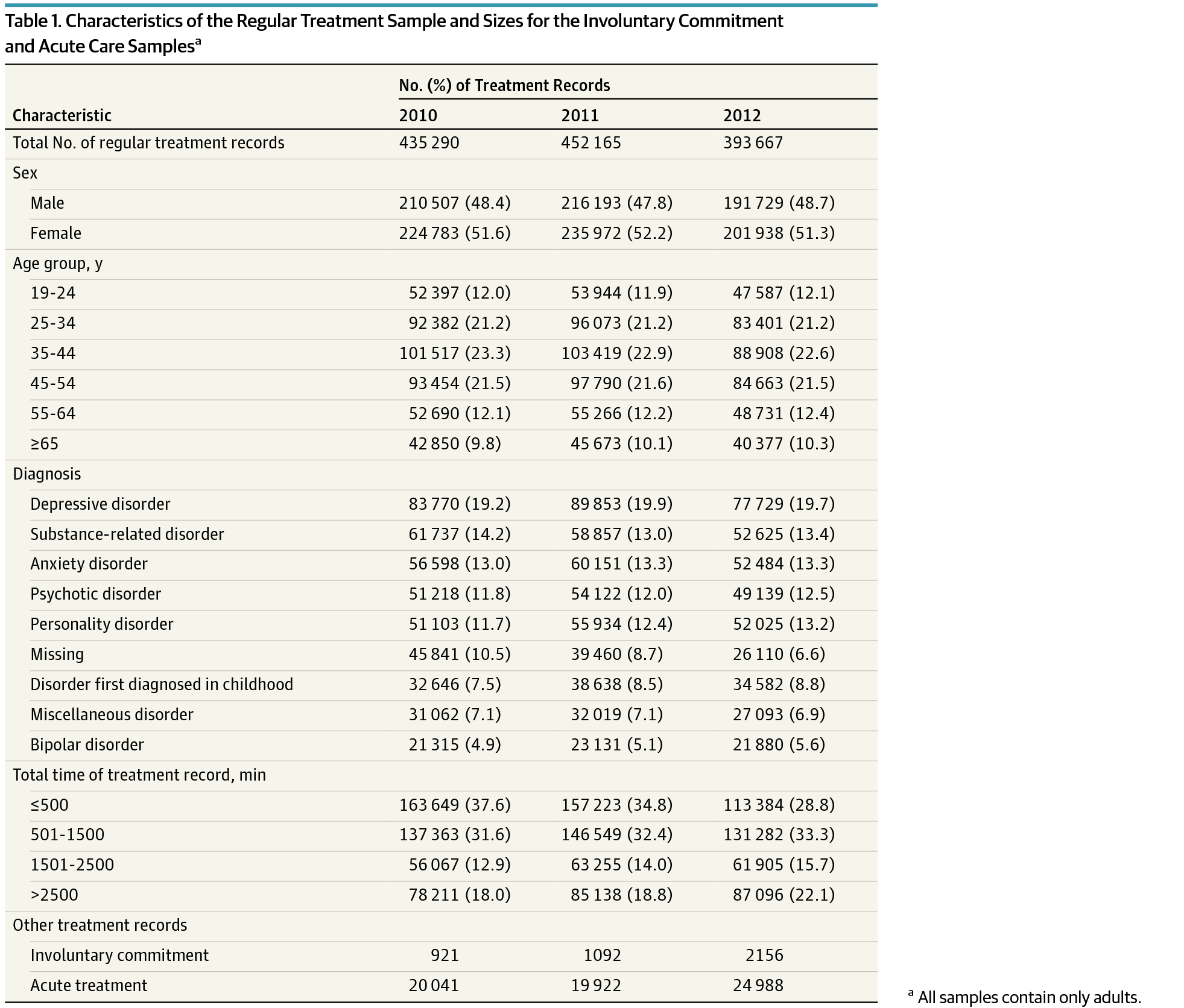
Design, Setting, and Participants This difference-in-differences study compared changes in mental health care use by adults, who experienced an increase in cost sharing, with changes in youths, who did not experience the increase and thus formed a control group. The study examined all 2 780 558 treatment records opened from January 1, 2010, through December 31, 2012, by 110 organizations that provide specialist mental health care in the Netherlands. Data analysis was performed from January 18, 2016, to May 9, 2017.
Exposures On January 1, 2012, the Dutch national government increased the out-of-pocket price of mental health services for adults by up to €200 (US$226) per year for outpatient treatment and €150 (US$169) per month for inpatient treatment.
Main Outcomes and Measures The number of treatment records opened each day in regular specialist mental health care, involuntary commitment, and acute mental health care, and annual specialist mental health care spending.
Results This study included 1 448 541 treatment records opened from 2010 to 2012 (mean [SD] age, 41.4 [16.7] years; 712 999 men and 735 542 women). The number of regular mental health care records opened for adults decreased abruptly and persistently by 13.4% (95% CI, −16.0% to −10.8%; P < .001) per day when cost sharing was increased in 2012. The decrease was substantial and significant for severe and mild disorders and larger in low-income than in high-income neighborhoods. Simultaneously, in 2012, daily record openings increased for involuntary commitment by 96.8% (95% CI, 87.7%-105.9%; P < .001) and for acute mental health care by 25.1% (95% CI, 20.8%-29.4%; P < .001). In contrast to our findings for adults, the use of regular care among youths increased slightly and the use of involuntary commitment and acute care decreased slightly after the reform. Overall, the cost-sharing reform was associated with estimated savings of €13.4 million (US$15.1 million). However, for adults with psychotic disorder or bipolar disorder, the additional costs of involuntary commitment and acute mental health care exceeded savings by €25.5 million (US$28.8 million).
Conclusions and Relevance Higher cost sharing for seriously ill and low-income patients could discourage treatment of vulnerable populations and create substantial downstream costs.
中文翻译:
成本分摊与心理保健使用,非自愿承诺和急性保健的关联
重要性 精神保健的自付费用较高,不仅可能节省成本,而且还会导致负面的下游后果。
目的 探讨较高的患者费用分摊与精神卫生保健的使用和下游影响(如非自愿承诺和急性精神卫生保健的使用)的相关性。
设计,环境和参与者 这项差异研究比较了成年人的心理保健使用的变化,他们经历了费用分担的增加,而青年人的变化则没有经历,因此形成了一个对照组。该研究调查了由110个在荷兰提供专业心理健康护理的组织从2010年1月1日至2012年12月31日开放的所有2 780 558个治疗记录。数据分析于2016年1月18日至2017年5月9日进行。
风险暴露 2012年1月1日,荷兰中央政府将成人心理健康服务的自付费用提高了,门诊治疗每年最高200欧元(226美元),住院患者每月最高150欧元(169美元)。治疗。
主要结果和措施 每天在常规专科精神保健,非自愿承诺和急性精神保健以及每年专科精神保健支出中开放的治疗记录数量。
结果 本研究包括从2010年至2012年开放的1 448 541例治疗记录(平均[SD]年龄,41.4 [16.7]岁; 712 999名男性和735 542名女性)。 随着2012年费用分摊的增加,每天为成年人开设的常规精神卫生记录的数量急剧且持续减少,每天持续减少13.4%(95%CI,-16.0%,达到-10.8%;P <.001)。对于重度和轻度疾病而言意义重大,在低收入人群中比在高收入人群中更大。同时,在2012年,非自愿承诺的每日开盘记录增加了96.8%(95%CI,87.7%-105.9%;P <.001)和急性精神卫生保健服务增加了25.1%(95%CI,20.8%-29.4%) ;P <.001)。与我们对成人的调查结果相反,改革后,年轻人对常规护理的使用略有增加,对非自愿承诺和急性护理的使用略有减少。总体而言,成本分摊改革带来了约1,340万欧元(约合1,510万美元)的节省。但是,对于患有精神病或双相情感障碍的成年人,非自愿承诺和急性精神卫生保健的额外费用使节省的费用超过了2550万欧元(2880万美元)。
结论和相关性 重病和低收入患者的较高费用分担可能会阻碍弱势人群的治疗,并产生大量的下游费用。










































 京公网安备 11010802027423号
京公网安备 11010802027423号