当前位置:
X-MOL 学术
›
J. Am. Coll. Cardiol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Prognostic Significance of Central Apneas Throughout a 24-Hour Period in Patients With Heart Failure
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2017-09-01 , DOI: 10.1016/j.jacc.2017.07.740 Michele Emdin , Gianluca Mirizzi , Alberto Giannoni , Roberta Poletti , Giovanni Iudice , Francesca Bramanti , Claudio Passino
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2017-09-01 , DOI: 10.1016/j.jacc.2017.07.740 Michele Emdin , Gianluca Mirizzi , Alberto Giannoni , Roberta Poletti , Giovanni Iudice , Francesca Bramanti , Claudio Passino
|
BACKGROUND
Large trials using noninvasive mechanical ventilation to treat central apnea (CA) occurring at night ("sleep apnea") in patients with systolic heart failure (HF) have failed to improve prognosis. The prevalence and prognostic value of CA during daytime and over an entire 24-h period are not well described. OBJECTIVES
This study evaluated the occurrence and prognostic significance of nighttime, daytime, and 24-h CA episodes in a large cohort of patients with systolic HF. METHODS
Consecutive patients receiving guideline-recommended treatment for HF (n = 525; left ventricular ejection fraction [LVEF] of 33 ± 9%; 66 ± 12 years of age; 77% males) underwent prospective evaluation, including 24-h respiratory recording, and were followed-up using cardiac mortality as an endpoint. RESULTS
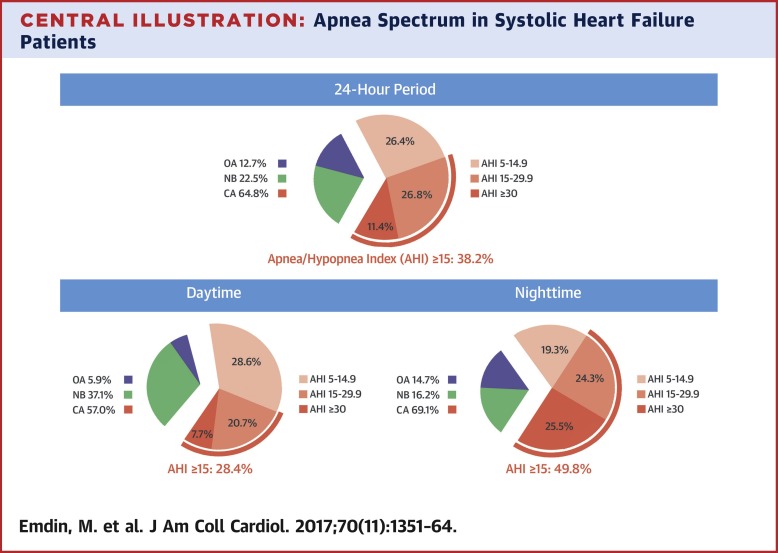
The 24-h prevalence of predominant CAs (apnea/hypopnea index [AHI] ≥5 events/h, with CA of >50%) was 64.8% (nighttime: 69.1%; daytime: 57.0%), whereas the prevalence of predominant obstructive apneas (OA) was 12.8% (AHI ≥5 events/h with OAs >50%; nighttime: 14.7%; daytime: 5.9%). Episodes of CA were associated with neurohormonal activation, ventricular arrhythmic burden, and systolic/diastolic dysfunction (all p < 0.05). During a median 34-month follow-up (interquartile range [IQR]: 17 to 36 months), 50 cardiac deaths occurred. Nighttime, daytime, and 24-h moderate-to-severe CAs were associated with increased cardiac mortality (AHI of
中文翻译:

心力衰竭患者 24 小时内中枢性呼吸暂停的预后意义
背景 使用无创机械通气来治疗收缩性心力衰竭 (HF) 患者夜间发生的中枢性呼吸暂停 (CA)(“睡眠呼吸暂停”)的大型试验未能改善预后。CA 在白天和整个 24 小时内的流行率和预后价值没有得到很好的描述。目的 本研究评估了大量收缩性 HF 患者夜间、白天和 24 小时 CA 发作的发生率和预后意义。方法 接受指南推荐的 HF 治疗的连续患者(n = 525;左心室射血分数 [LVEF] 为 33 ± 9%;66 ± 12 岁;77% 男性)接受前瞻性评估,包括 24 小时呼吸记录,并以心脏死亡率作为终点进行随访。结果 主要 CA 的 24 小时患病率(呼吸暂停/低通气指数 [AHI] ≥ 5 个事件/小时,CA > 50%)为 64.8%(夜间:69.1%;白天:57.0%),而主要阻塞性呼吸暂停 (OA) 为 12.8%(AHI ≥5 个事件/小时,OAs >50%;夜间:14.7%;白天:5.9%)。CA 发作与神经激素激活、室性心律失常负荷和收缩/舒张功能障碍有关(所有 p < 0.05)。在中位 34 个月的随访期间(四分位距 [IQR]:17 至 36 个月),发生了 50 例心脏死亡。夜间、白天和 24 小时中度至重度 CA 与心脏死亡率增加相关(AHI 为 8%(AHI ≥ 5 个事件/小时,OAs > 50%;夜间:14.7%;白天:5.9%)。CA 发作与神经激素激活、室性心律失常负荷和收缩/舒张功能障碍有关(所有 p < 0.05)。在中位 34 个月的随访期间(四分位距 [IQR]:17 至 36 个月),发生了 50 例心脏死亡。夜间、白天和 24 小时中度至重度 CA 与心脏死亡率增加相关(AHI 为 8%(AHI ≥ 5 个事件/小时,OAs > 50%;夜间:14.7%;白天:5.9%)。CA 发作与神经激素激活、室性心律失常负荷和收缩/舒张功能障碍有关(所有 p < 0.05)。在中位 34 个月的随访期间(四分位距 [IQR]:17 至 36 个月),发生了 50 例心脏死亡。夜间、白天和 24 小时中度至重度 CA 与心脏死亡率增加相关(AHI 为
更新日期:2017-09-01
中文翻译:
心力衰竭患者 24 小时内中枢性呼吸暂停的预后意义
背景 使用无创机械通气来治疗收缩性心力衰竭 (HF) 患者夜间发生的中枢性呼吸暂停 (CA)(“睡眠呼吸暂停”)的大型试验未能改善预后。CA 在白天和整个 24 小时内的流行率和预后价值没有得到很好的描述。目的 本研究评估了大量收缩性 HF 患者夜间、白天和 24 小时 CA 发作的发生率和预后意义。方法 接受指南推荐的 HF 治疗的连续患者(n = 525;左心室射血分数 [LVEF] 为 33 ± 9%;66 ± 12 岁;77% 男性)接受前瞻性评估,包括 24 小时呼吸记录,并以心脏死亡率作为终点进行随访。结果 主要 CA 的 24 小时患病率(呼吸暂停/低通气指数 [AHI] ≥ 5 个事件/小时,CA > 50%)为 64.8%(夜间:69.1%;白天:57.0%),而主要阻塞性呼吸暂停 (OA) 为 12.8%(AHI ≥5 个事件/小时,OAs >50%;夜间:14.7%;白天:5.9%)。CA 发作与神经激素激活、室性心律失常负荷和收缩/舒张功能障碍有关(所有 p < 0.05)。在中位 34 个月的随访期间(四分位距 [IQR]:17 至 36 个月),发生了 50 例心脏死亡。夜间、白天和 24 小时中度至重度 CA 与心脏死亡率增加相关(AHI 为 8%(AHI ≥ 5 个事件/小时,OAs > 50%;夜间:14.7%;白天:5.9%)。CA 发作与神经激素激活、室性心律失常负荷和收缩/舒张功能障碍有关(所有 p < 0.05)。在中位 34 个月的随访期间(四分位距 [IQR]:17 至 36 个月),发生了 50 例心脏死亡。夜间、白天和 24 小时中度至重度 CA 与心脏死亡率增加相关(AHI 为 8%(AHI ≥ 5 个事件/小时,OAs > 50%;夜间:14.7%;白天:5.9%)。CA 发作与神经激素激活、室性心律失常负荷和收缩/舒张功能障碍有关(所有 p < 0.05)。在中位 34 个月的随访期间(四分位距 [IQR]:17 至 36 个月),发生了 50 例心脏死亡。夜间、白天和 24 小时中度至重度 CA 与心脏死亡率增加相关(AHI 为








































 京公网安备 11010802027423号
京公网安备 11010802027423号