当前位置:
X-MOL 学术
›
J. Am. Coll. Cardiol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
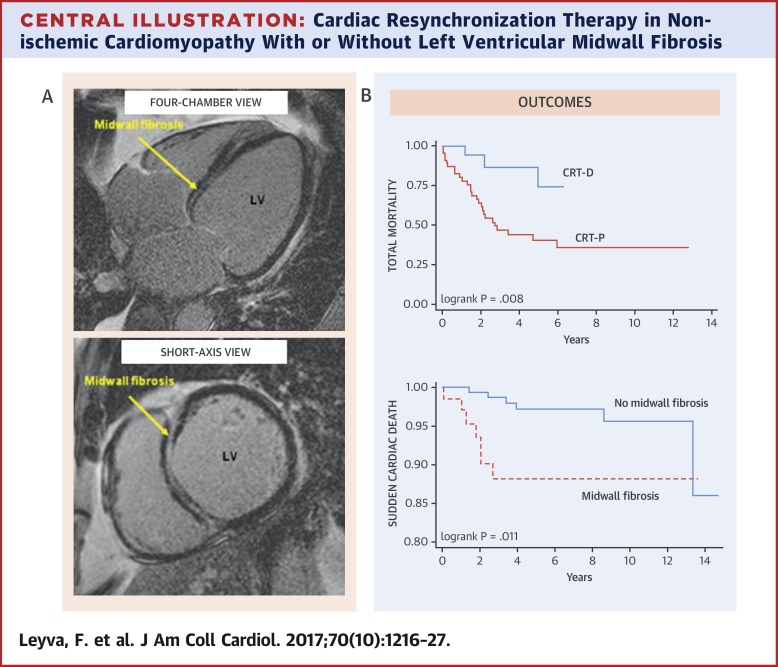
Outcomes of Cardiac Resynchronization Therapy With or Without Defibrillation in Patients With Nonischemic Cardiomyopathy
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2017-09-01 , DOI: 10.1016/j.jacc.2017.07.712 Francisco Leyva , Abbasin Zegard , Edmund Acquaye , Christopher Gubran , Robin Taylor , Paul W.X. Foley , Fraz Umar , Kiran Patel , Jonathan Panting , Howard Marshall , Tian Qiu
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2017-09-01 , DOI: 10.1016/j.jacc.2017.07.712 Francisco Leyva , Abbasin Zegard , Edmund Acquaye , Christopher Gubran , Robin Taylor , Paul W.X. Foley , Fraz Umar , Kiran Patel , Jonathan Panting , Howard Marshall , Tian Qiu
|
BACKGROUND
Recent studies have cast doubt on the benefit of cardiac resynchronization therapy (CRT) with defibrillation (CRT-D) versus pacing (CRT-P) for patients with nonischemic cardiomyopathy (NICM). Left ventricular myocardial scar portends poor clinical outcomes. OBJECTIVES
The aim of this study was to determine whether CRT-D is superior to CRT-P in patients with NICM either with (+) or without (-) left ventricular midwall fibrosis (MWF), detected by cardiac magnetic resonance. METHODS
Clinical events were quantified in patients with NICM who were +MWF (n = 68) or -MWF (n = 184) who underwent cardiac magnetic resonance prior to CRT device implantation. RESULTS
In the total study population, +MWF emerged as an independent predictor of total mortality (adjusted hazard ratio [aHR]: 2.31; 95% confidence interval [CI]: 1.45 to 3.68), total mortality or heart failure hospitalization (aHR: 2.02; 95% CI: 1.32 to 3.09), total mortality or hospitalization for major adverse cardiac events (aHR: 2.02; 95% CI: 1.32 to 3.07), death from pump failure (aHR: 1.95; 95% CI: 1.11 to 3.41), and sudden cardiac death (aHR: 3.75; 95% CI: 1.26 to 11.2) over a maximum follow-up period of 14 years (median 3.8 years [interquartile range: 2.0 to 6.1 years] for +MWF and 4.6 years [interquartile range: 2.4 to 8.3 years] for -MWF). In separate analyses of +MWF and -MWF, total mortality (aHR: 0.23; 95% CI: 0.07 to 0.75), total mortality or heart failure hospitalization (aHR: 0.32; 95% CI: 0.12 to 0.82), and total mortality or hospitalization for major adverse cardiac events (aHR: 0.30; 95% CI: 0.12 to 0.78) were lower after CRT-D than after CRT-P in +MWF but not in -MWF. CONCLUSIONS
In patients with NICM, CRT-D was superior to CRT-P in +MWF but not -MWF. These findings have implications for the choice of device therapy in patients with NICM.
中文翻译:

非缺血性心肌病患者心脏再同步治疗伴或不伴除颤的结果
背景 最近的研究对心脏再同步治疗 (CRT) 与除颤 (CRT-D) 与起搏 (CRT-P) 对非缺血性心肌病 (NICM) 患者的益处提出了质疑。左心室心肌瘢痕预示着临床结果不佳。目的 本研究的目的是确定 CRT-D 是否优于 CRT-P 在 NICM 患者中,无论是 (+) 还是没有 (-) 左心室中壁纤维化 (MWF),通过心脏磁共振检测。方法 在 CRT 装置植入前接受心脏磁共振的 NICM 患者的临床事件进行量化,这些患者为 +MWF(n = 68)或 -MWF(n = 184)。结果 在整个研究人群中,+MWF 成为总死亡率的独立预测因子(调整后的风险比 [aHR]:2.31;95% 置信区间 [CI]:1.45 至 3.68),总死亡率或心力衰竭住院率(aHR:2.02;95% CI:1.32 至 3.09),主要不良心脏事件的总死亡率或住院率(aHR:2.02;95% CI:1.32 至 3.07),泵衰竭死亡(aHR: 1.95;95% CI:1.11 至 3.41)和心源性猝死(aHR:3.75;95% CI:1.26 至 11.2),最长随访 14 年(中位数 3.8 年 [四分位距:2.0 至 6.1 年) ] +MWF 和 4.6 年 [四分位距:2.4 至 8.3 年] -MWF)。在对 +MWF 和 -MWF 的单独分析中,总死亡率(aHR:0.23;95% CI:0.07 至 0.75)、总死亡率或心力衰竭住院(aHR:0.32;95% CI:0.12 至 0.82)和总死亡率或在 +MWF 中,CRT-D 后因主要不良心脏事件住院(aHR:0.30;95% CI:0.12 至 0.78)低于 CRT-P,但在 -MWF 中则不然。结论 在 NICM 患者中,CRT-D 在 +MWF 中优于 CRT-P,但在 -MWF 中不优于 CRT-P。这些发现对 NICM 患者的器械治疗选择具有重要意义。
更新日期:2017-09-01
中文翻译:
非缺血性心肌病患者心脏再同步治疗伴或不伴除颤的结果
背景 最近的研究对心脏再同步治疗 (CRT) 与除颤 (CRT-D) 与起搏 (CRT-P) 对非缺血性心肌病 (NICM) 患者的益处提出了质疑。左心室心肌瘢痕预示着临床结果不佳。目的 本研究的目的是确定 CRT-D 是否优于 CRT-P 在 NICM 患者中,无论是 (+) 还是没有 (-) 左心室中壁纤维化 (MWF),通过心脏磁共振检测。方法 在 CRT 装置植入前接受心脏磁共振的 NICM 患者的临床事件进行量化,这些患者为 +MWF(n = 68)或 -MWF(n = 184)。结果 在整个研究人群中,+MWF 成为总死亡率的独立预测因子(调整后的风险比 [aHR]:2.31;95% 置信区间 [CI]:1.45 至 3.68),总死亡率或心力衰竭住院率(aHR:2.02;95% CI:1.32 至 3.09),主要不良心脏事件的总死亡率或住院率(aHR:2.02;95% CI:1.32 至 3.07),泵衰竭死亡(aHR: 1.95;95% CI:1.11 至 3.41)和心源性猝死(aHR:3.75;95% CI:1.26 至 11.2),最长随访 14 年(中位数 3.8 年 [四分位距:2.0 至 6.1 年) ] +MWF 和 4.6 年 [四分位距:2.4 至 8.3 年] -MWF)。在对 +MWF 和 -MWF 的单独分析中,总死亡率(aHR:0.23;95% CI:0.07 至 0.75)、总死亡率或心力衰竭住院(aHR:0.32;95% CI:0.12 至 0.82)和总死亡率或在 +MWF 中,CRT-D 后因主要不良心脏事件住院(aHR:0.30;95% CI:0.12 至 0.78)低于 CRT-P,但在 -MWF 中则不然。结论 在 NICM 患者中,CRT-D 在 +MWF 中优于 CRT-P,但在 -MWF 中不优于 CRT-P。这些发现对 NICM 患者的器械治疗选择具有重要意义。








































 京公网安备 11010802027423号
京公网安备 11010802027423号