Article Text

Abstract
Background Fractal dimension (D) characterises the size distribution of low attenuation clusters on CT and assesses the spatial heterogeneity of emphysema that per cent low attenuation volume (%LAV) cannot detect. This study tested the hypothesis that %LAV and D have different roles in predicting decline in FEV1, exacerbation and mortality in patients with COPD.
Methods Chest inspiratory CT scans in the baseline and longitudinal follow-up records for FEV1, exacerbation and mortality prospectively collected over 10 years in the Hokkaido COPD Cohort Study were examined (n=96). The associations between CT measures and long-term outcomes were replicated in the Kyoto University cohort (n=130).
Results In the Hokkaido COPD cohort, higher %LAV, but not D, was associated with a greater decline in FEV1 and 10-year mortality, whereas lower D, but not %LAV, was associated with shorter time to first exacerbation. Multivariable analysis for the Kyoto University cohort confirmed that lower D at baseline was independently associated with shorter time to first exacerbation and that higher LAV% was independently associated with increased mortality after adjusting for age, height, weight, FEV1 and smoking status.
Conclusion These well-established cohorts clarify the different prognostic roles of %LAV and D, whereby lower D is associated with a higher risk of exacerbation and higher %LAV is associated with a rapid decline in lung function and long-term mortality. Combination of %LAV and fractal D may identify COPD subgroups at high risk of a poor clinical outcome more sensitively.
- emphysema
- COPD ÀÜ mechanisms
Statistics from Altmetric.com
Key messages
What is the key question?
Do the CT indices of emphysema, that is, per cent low attenuation volume and the fractal dimension of low attenuation clusters, have different roles in predicting long-term clinical outcomes in patients with COPD?
What is the bottom line?
Measuring the fractal dimension of emphysematous regions on CT may help to identify a subgroup of patients with COPD who are at higher risk of future exacerbations.
Why read on?
Assessment of the fractal dimension of low attenuation clusters combined with the current standard emphysema index, that is, per cent low attenuation volume, can facilitate stratification of subjects with COPD into clinically relevant phenotypes in terms of the three major long-term outcomes of COPD, namely, decline in lung function, exacerbation and survival
Introduction
COPD is one of the leading causes of death worldwide and imposes a huge socioeconomic burden.1 Management of the disease remains unsatisfactory, and prediction of the heterogeneous clinical outcomes for individual patients remains challenging. Even longitudinal decline in airflow obstruction, a physiological hallmark of COPD assessed as FEV1, varies markedly from patient to patient.2 3
Emphysema is a major pathology in COPD that is characterised by airspace enlargement with destruction of the alveolar septa and can be identified as low attenuation regions on CT scans.4 5 The volume percentage of the low attenuation regions over total lung (%LAV) is the most widely used emphysema index. CT studies have shown that %LAV is associated with many clinical features6 7 and predicts rapid decline of FEV1 2 and mortality8 in patients with COPD. Furthermore, the spatial distribution of emphysema has been shown to have clinical and physiological impacts independently of the %LAV in the total lung.9 Therefore, evaluation of the severity and spatial pattern of emphysema is important when predicting long-term outcomes in patients with COPD.
Previous experimental research has identified many factors associated with the pathogenesis of emphysema, including inflammation, a protease–antiprotease imbalance, and oxidative stress.10 However, none of these factors can account for the large variation in the size distribution of emphysema. In contrast, CT and computational model simulation studies have suggested that mechanical stress, as a result of abnormal stretch around emphysematous regions, has a prominent role in the heterogeneous progression of emphysema.11–16 A study by Mishima et al 11 introduced the concept of the fractal dimension in CT imaging of COPD and showed that the size distribution of clusters of emphysematous regions follows a power law characterised by fractal dimension D. Those authors showed that the fractal D is decreased without a change in %LAV in early-stage COPD,11 and succeeded in linking the mechanical force-based destruction of the alveolar walls to the reduction in the fractal D on CT using elastic spring network simulation.
Moreover, a subsequent longitudinal study showed that patients who experienced exacerbations during follow-up showed both a decrease in the fractal D and an increase in %LAV.12 In that study, computer simulation revealed that a decrease in the fractal D is more sensitive to coalescence of neighbouring clusters of emphysematous regions than an increase in %LAV. Therefore, the change in D is not always parallel to that of %LAV and might be able to provide information additional to that provided by %LAV.
We hypothesised that %LAV and the fractal D, as assessed by CT, may have different roles in predicting the clinical outcomes of COPD, such as decline in FEV1, exacerbation and survival. The aims of this study were (1) to explore the associations between baseline %LAV and fractal D and the rates of decline in FEV1 and time to first exacerbation during 5 years of follow-up and 10-year mortality in the Hokkaido COPD cohort and (2) to confirm the results in another cohort from Kyoto University.
Materials and methods
Hokkaido COPD Cohort Study
Subjects
The present study is a part of the Hokkaido COPD Cohort Study, a multicentre observational prospective cohort that was started in 2003–2005 and completed in 2013–2015.2 3 All study participants had been diagnosed as having COPD before the enrolment. Chest CT scans were annually performed during an exacerbation-free stable period for the first 5 years.
To guarantee the length of the observation period, we only included subjects who had appropriate CT data obtained either at the first evaluation (visit 1) or 1 year later (visit 3). Information from the date of CT examination was taken for exacerbations and mortality.
The protocol for the Hokkaido COPD Cohort Study was approved by the Health Authority Research Ethics Committee of Hokkaido University School of Medicine (med 02-001) and performed in accordance with the amended Declaration of Helsinki. All participants provided written informed consent.
Clinical outcome measurements
Annual changes in post-bronchodilator FEV1 were calculated using a linear mixed effects model that included the original group of 279 patients with COPD in our previous study.2 Until year 5, information regarding exacerbations of COPD was collected every month by postcard (response rate >99%) as previously reported.17 18 Exacerbation was defined using both the antibiotic definition, that is, symptom criteria plus antibiotic treatment, and the prescription definition, that is, symptom criteria plus requiring a change in prescription. Symptom definition19 is worsening or new onset of two of the major symptoms (increased dyspnoea, change in sputum purulence or increased sputum volume) or any one major symptom plus any minor symptoms (fever, increased cough or wheezing) compared with baseline.
Mortality until year 10 in the original cohort study
The majority of the study participants (85.6%, 167/195) consented to the extension of the follow-up programme. Their survival were confirmed by regular check-ups by year 5, and then confirmed by telephone interview and/or medical chart review by year 10.17
Quantitative chest CT
This study used the data for subjects in whom inspiratory CT scans with a 1.25 mm slice thickness were acquired at Hokkaido University Hospital using a Somatom plus Volume Zoom scanner (Siemens AG, Berlin, Germany) at 140 kVp, 150 mA, 4×1 mm detector collimation and helical pitch 6 or 7. The raw data were reconstructed with a soft algorithm (standard kernel, FC30).2
CT assessment of emphysema
All the CT images were assessed at Shiga University of Medical Science using Apollo software (VIDA Diagnostics, Coralville, Iowa, USA). For calculation of the fractal D, neighbouring voxels less than −950 HU were three-dimensionally identified as low attenuation cluster (LAC) and the volume of each LAC was measured. The fractal property of the size distribution of the LACs was tested by plotting the log-transformed volume of the LACs on the x-axis and the log-transformed cumulative count of LACs that were larger than the given volume on the y-axis. Linear regression was performed on this log-log plot, and goodness of fit was confirmed for all the data, indicating that the cumulative count (Y) of the LACs larger than the volume (X) is governed by the equation, Y=K×X−D. The fractal dimension D is obtained as the absolute slope of the regression line.11 12
Pulmonary function tests
Pulmonary function tests and CT scans were performed on the same day, except when a patient attended twice within 1 week. Spirometry, lung volumes and diffusion capacity (assessed as diffusing capacity of the lung for carbon monoxide (DLco) and DLco/alveolar volume) were measured using a rolling seal Chestac-33 spirometer (Chest MI, Tokyo, Japan) according to the Japanese Respiratory Society guidelines,20 which are similar to the American Thoracic Society guidelines.21 22
Kyoto University cohort
The Kyoto University cohort has been well described elsewhere.23 Briefly, 130 male subjects underwent chest inspiratory CT scans and pulmonary function tests and were originally followed up for a median of 2542 days. For the present study, the follow-up was extended as of December 2017 and the final follow-up duration was 3530 (378–4429) days. All-cause mortality and moderate to severe exacerbations that required antibiotics and/or systemic steroids were recorded. All CT images with a 0.5 mm slice thickness at full inspiration in the Kyoto University cohort were obtained using an Aquilion 64 scanner (Toshiba, Tokyo, Japan) at 0.5 mm collimation, a scan time of 500 ms, 120 kVp and autoexposure control, and reconstructed using a sharp algorithm (FC56). The %LAV and fractal D were calculated using a Synapse Vincent volume analyser (Fujifilm Medical Systems, Tokyo, Japan).24
Statistical analyses
The relationships between the pulmonary function indices and CT parameters were analysed using a bivariate correlation analysis. Multivariable linear regression analyses were performed using baseline FEV1, age, sex, height, smoking status and either %LAV or the fractal D as independent variables and annual decline in FEV1 as the dependent variable. The Student’s t-test, Mann-Whitney U test or χ2 test were applied for the group comparisons. The subjects were categorised into those with mild or severe emphysematous changes on CT using either %LAV or D. The cut-off values for the categorisation were as follows: the median of %LAV and the fractal D for the Hokkaido COPD cohort and the first quantile of %LAV and the third quantile of the fractal D for the Kyoto University cohort. Different cut-off values were used because of a difference in the severity of COPD between the two cohorts. Exacerbation-free survival and mortality were compared between subjects with mild emphysematous change and those with severe emphysematous change on CT using the Kaplan-Meier method with the log-rank test. We used univariate and multivariable Cox proportional hazards models that evaluated the effects of covariates on the time to the first exacerbation and death after enrolment. To avoid the problem of collinearity, a separate model including either %LAV or the fractal D was made for the multivariable models. All statistical analyses were performed using JMP 12.0 (SAS Institute, Cary, North Carolina, USA) and R version 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria).25 A p-value <0.05 was considered statistically significant.
Results
Study population
One hundred and twenty-one of the 279 patients in the original Hokkaido COPD Cohort Study were recruited at Hokkaido University Hospital. Ninety-one patients underwent CT scans at visit 1; however, 21 patients were excluded because their CT scans were not reconstructed with the standard reconstruction kernel (n=19) or abnormal chest shadows such as giant bullae or pleural thickening were found (n=2). A further 26 patients who underwent CT scans at visit 3 were also included. Therefore, a total of 96 patients were included for the present analyses. Table 1 shows the characteristics of the subjects in the Hokkaido COPD cohort in comparison with the Kyoto University cohort that was used to validate the results of the Hokkaido COPD cohort. CONSORT (Consolidated Standards of Reporting Trials)-style diagrams for the Hokkaido COPD and the Kyoto University cohorts are shown in online supplementary figures E1 and E2, respectively. Pulmonary function, fractal D and %LAV differed between the two cohorts. There were no significant differences in the anthropomorphometric data or pulmonary function test results between the 96 patients included in the present study and the 279 patients considered eligible for the original cohort (online supplementary table E1).
Supplemental material
Supplemental material
Supplemental material
Characteristics of subjects in the Hokkaido COPD and Kyoto University cohorts
Relationships between %LAV, fractal D and pulmonary function indices in the Hokkaido COPD cohort
There was a significant negative correlation between %LAV and D (r=−0.54 (95% CI −0.37 to 0.66), p<0.01; online supplementary figure E3). Table 2 summarises the correlations of %LAV and D with pulmonary function.
Supplemental material
Correlation coefficients between CT measures of emphysema and pulmonary function tests (n=96)
Associations of baseline %LAV and fractal D with FEV1 decline, exacerbation and survival
Hokkaido COPD cohort
Figure 1 shows that a higher %LAV and lower D were associated with a greater annual decline in FEV1 (r=−0.31 (95% CI −0.48 to 0.12), p<0.01 and r=0.22 (95% CI 0.02 to 0.41), p=0.03). In multivariable regression analysis (table 3), %LAV, but not D, was independently correlated with the annual FEV1 decline after adjusting for baseline FEV1, age, sex, height and smoking status.

Associations of baseline per cent low attenuation volume (%LAV) and the fractal dimension (D) with FEV1 decline in the Hokkaido COPD Cohort Study. High %LAV and low D predicted accelerated decline in FEV1.
Multivariable linear regression analysis exploring factors independently associated with the annual decline in FEV1 in the Hokkaido COPD cohort
Twenty-four of the 96 subjects with COPD experienced exacerbations and 37 died during a median follow-up of 3352 (range 770–3864) days. The 96 patients were divided into low and high D groups based on the median D value (1.474) as well as into low and high %LAV groups based on the median %LAV (18.95); the characteristics in these groups are shown in table 4. Time to first exacerbation was shorter in the low D group than in the high D group (p<0.01 using the antibiotic definition; p=0.01 using the prescription definition; figure 2A and online supplementary figure E4). There was no significant difference in the time to first exacerbation between the high and low %LAV groups (p=0.60 using antibiotic definition; p=0.75 using the prescription definition; figure 2A and online supplementary figure E4). The prognosis was poorer in the high %LAV group than in the low %LAV group (p<0.01) but did not differ between the low and high D groups (p=0.30; figure 2B). The univariable Cox proportional hazards analyses showed that lower D, but not %LAV, was associated with shorter time to first exacerbation (HR 0.04 (95% CI 0.00 to 0.85), p=0.04, and HR 1.03 (95% CI 0.99 to 1.06), p=0.12), whereas higher %LAV, but not D, was associated with mortality (HR 0.14 (95% CI 1.02 to 1.07), p<0.01, and HR 0.11 (95% CI 0.01 to 1.35), p=0.08, online supplementary table E2). The multivariable Cox proportional hazard analyses in the Hokkaido COPD cohort (online supplementary table E2) did not show an association between lower D or high %LAV and time to first exacerbation or mortality.
Supplemental material
Time to first exacerbation according to the antibiotic definition and mortality categorised by baseline fractal dimension (D) or per cent low attenuation volume (%LAV/pLAV) in the Hokkaido COPD cohort. The patients were divided into those with mild and severe emphysematous changes based on either the median of D or median of %LAV. Patients with a median D value <1.474 were categorised as a low D group (n=46) and those with a median %LAV value of 18.95 were categorised as a low %LAV group (n=46). (A) More subjects in the low D group experienced exacerbations than those in the high D group (p<0.01). The frequency of exacerbations did not differ between the high and low %LAV groups (p=0.49). (B) The high %LAV group was associated with a poor prognosis compared with the low %LAV group (p<0.01). The prognosis did not differ between the low D and high D groups (p=0.31).
Characteristics of patients in the Hokkaido COPD cohort with mild or severe emphysematous change on CT
Kyoto University cohort
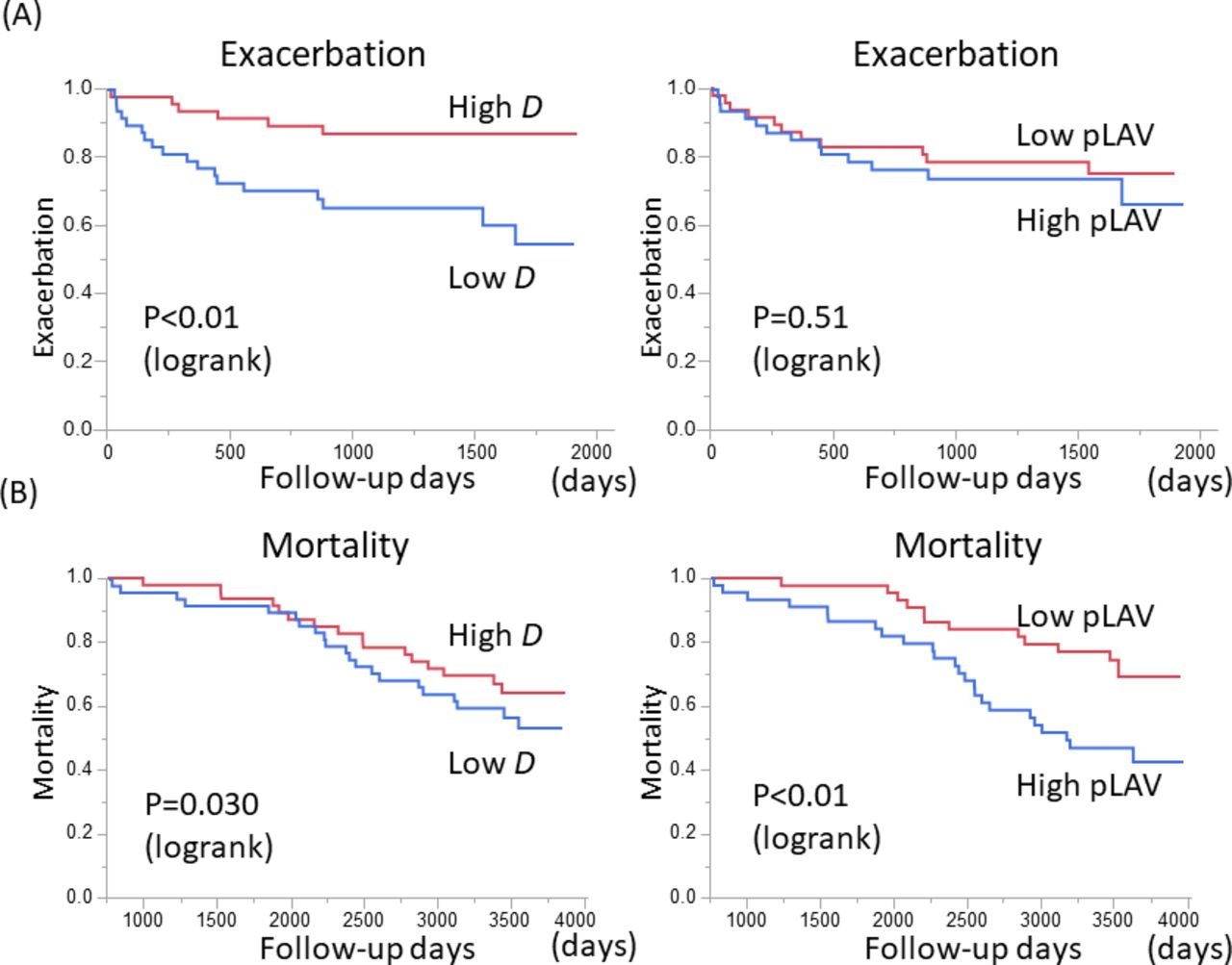
The Kyoto University cohort23 was also evaluated to confirm the results of the Hokkaido COPD cohort Study. Ninety-eight of 130 men with COPD in the Kyoto University cohort experienced moderate to severe exacerbations and 34 died during a median follow-up of 3530 (range 378–4429) days (table 1). To evaluate the difference in disease severity, the distribution of %FEV1 was compared between the two cohorts (online supplementary figure E5). The median %FEV1 in the Hokkaido COPD cohort was equivalent to the 68th percentile of %FEV1 in the Kyoto University cohort. Because the 68th percentile was closer to the third quantile than the median (second quantile), the patients in the Kyoto University cohort were divided into those with mild or severe emphysematous changes based on either the first quantile of %LAV (low, n=33; high, n=97) or the third quantile of D (high, n=33; low, n=97). Figure 3A shows that time to first exacerbation was shorter in the low D group than in the high D group but did not differ between the low and high %LAV groups. In contrast, Figure 3B shows that the mortality rate was higher in the high %LAV group than in the low %LAV group but did not differ between the low and high D groups. Furthermore, the multivariable Cox proportional hazards analysis (table 5) showed significant associations of lower D with shorter time to first exacerbation and a poor prognosis (HR 0.11 (95% CI 0.16 to 0.87), p=0.032 and HR 0.01 (95% CI 0.00 to 0.71), p=0.029, respectively), whereas a higher LAV% was associated with a poor prognosis (HR 1.05 (95% CI 1.00 to 1.10), p=0.048) but not with exacerbation (HR 1.02 (95% CI 0.99 to 1.05), p=0.11).
Supplemental material

{kind=link}
{kind=link}
{kind=link}
Time to first exacerbation and mortality categorised by baseline fractal dimension (D) and by per cent low attenuation volume (%LAV/pLAV) in the Kyoto University cohort. The patients were divided into those with mild or severe emphysematous changes based on either the first quantile of %LAV (low LAV, n=33; high LAV, n=97) or the third quantile of D (low D, n=97; high D, n=33). (A) More subjects in the low D group experienced exacerbations than those in the high D group. The time to first exacerbation did not differ between the low and high %LAV groups. (B) In contrast, there were more deaths during follow-up in the high %LAV group than in the low %LAV group. There was no significant difference in mortality between the low and high D groups.
Multivariable Cox proportional hazards analysis of exacerbation and all-cause mortality in the Kyoto university cohort (n=130)
Discussion
The present study shows that exacerbations of COPD can be sensitively predicted by the baseline fractal dimension D but not by %LAV, whereas an accelerated decline in FEV1 and long-term mortality over 10 years can be sensitively predicted by the baseline %LAV. To the best of our knowledge, this is the first research to clarify the different prognostic roles of %LAV and D in COPD. The strength of the study is that the main findings from the Hokkaido COPD Cohort Study were confirmed in another independent cohort, that is, the Kyoto University cohort.
In general, as emphysema progresses, %LAV is increased and the fractal D is decreased on CT.11 12 However, the changes in %LAV and fractal D are not always synchronised. Previous studies have shown that a reduction in D is not accompanied by a change in %LAV in the early stages of COPD11 and that %LAV increases with hyperinflation of the lung without a change in the fractal D in asthma.26 In our present study, %LAV was associated with %TLC (total lung capacity), %FRC (functional residual capacity), %RV (residual volume) and RV/TLC more closely than the fractal D, while the correlation between %LAV and the fractal D remained statistically significant.
The difference between %LAV and the fractal D is further highlighted by the present finding that a reduced D, but not an increased %LAV, is associated with a higher risk of exacerbations over time. This result is consistent with a previous report that showed an association between exacerbations and reduction in D in patients with COPD.12 The reduced fractal D is closely associated with the parenchymal destruction induced by increased mechanical force, and the propagation of this force-based destruction leads to conjoining of emphysematous regions that is characterised by a few large clusters of emphysematous regions and many small clusters of emphysematous regions.11 16 27
The COPD in the subjects enrolled in the Kyoto University cohort was more severe than that in the Hokkaido COPD cohort (mean and SD %FEV1, 57.6±20.3 vs 66.0±19.4, respectively). However, given that use of different reconstruction kernels and slice thickness can affect quantitative measurement of emphysema,28 we could not directly compare %LAV and D between the two cohorts. Indeed, the mean %LAV was lower in the Hokkaido COPD cohort than in the Kyoto University cohort, which might reflect differences in the scanning conditions as well as disease severity.
To determine an appropriate cut-off value to dichotomise patients for the Kaplan-Meier analyses, we compared the distribution of %FEV1 and estimated the difference in disease severity. We found that the median %FEV1 in the Hokkaido COPD cohort was equivalent to the 68th percentile of %FEV1 in the Kyoto University cohort; because the 68th percentile was closer to the third quantile (75th percentile) than the median, we used the third quantile of D and the first quantile of %LAV to divide patients into mild and severe emphysema groups. Furthermore, the findings were the same even when the patients were dichotomised based on the 68th percentile as shown in online supplementary figure 6. It should also be noted that despite the differences in the CT scanners, reconstruction algorithms and slice thicknesses between the two cohorts, the major findings regarding exacerbations and mortality in the Hokkaido COPD cohort was replicated by data from the Kyoto University cohort, indicating good reproducibility of the results.
Supplemental material
Although the univariate analysis showed an association of the baseline %LAV and fractal D with annual decline in FEV1, the multivariable analysis showed that only the %LAV was associated with the decline in FEV1. This finding is in line with previous reports of an association between emphysema on CT and a decline in FEV1.2 29 Given the association of airflow obstruction with a combination of small airways disease and emphysema30 and the resolution of CT not being high enough to separate these two entities, we speculate that although both %LAV and the fractal D are affected by the small airways and emphysema, the influence of small airway disease may be greater for %LAV than for the fractal D. The data from the Hokkaido COPD cohort show that mortality in patients with COPD can be predicted by %LAV but not by fractal D, whereas the data from the Kyoto University cohort show that both %LAV and fractal D predict mortality. These findings confirm previous reports of an association between the baseline %LAV and future mortality.8 However, the role of fractal D as a predictor of long-term mortality needs further investigation in a larger study population.
Building risk prediction models for long-term clinical outcomes remains an unmet need to improve the personalised management of COPD.31 32 Especially, discovering predictors to identify patients with a high risk of exacerbations and providing maximised, long-term preventive care is important. Although a subgroup of patients has consistently high risk of frequent exacerbation,33 34 the proportion of this frequent exacerbator phenotype is small and the exacerbation frequency of most patients may vary from year to year.35 Thus, predicting future exacerbations is still challenging. Furthermore, hospitalisation due to COPD exacerbations imposes an economic burden and increases mortality,36 and the increased mortality remains problematic, even after hospital discharge.37 Therefore, the present finding that reduced fractal D predicts exacerbation in the long-term could help build sensitive predicting tools for exacerbations, and suggests that patients with low fractal D should receive long-term intensive care to prevent exacerbations. In contrast, we found that increased %LAV is associated with higher 10-year mortality rather than exacerbation. Because lung cancer, in addition to respiratory disease including exacerbations and pneumonia and cardiovascular disease, is a major cause of death in patients with COPD,38 our finding suggests that a comprehensive care regimen including lung cancer screening should be implemented in patients with high %LAV.
This study has some limitations. First, the sample size was relatively small, which might explain the discordant results of the multivariable Cox proportional hazards analysis of exacerbation and all-cause mortality between the two cohorts. However, we at least confirmed the major finding that low fractal D predicts exacerbation and high %LAV predicts mortality in these two independent cohorts. This strategy increases the validity of our study. Second, the subjects in both cohorts were predominantly male, which reflects the sex distribution of patients with COPD in Japan.39 Given the sex-related difference in severity of emphysema,40 it is unclear whether our findings can be generalised to female patients with COPD.
In conclusion, these two well-established Japanese cohorts clearly demonstrated the distinct predictive roles of %LAV and D, whereby a lower D predicts future exacerbation and a higher %LAV predicts rapid decline in lung function and a poor prognosis in patients with COPD. Further morphological assessment of emphysema using a combination of %LAV and the fractal D may identify more appropriate subtypes that have distinct risks for major clinical outcomes and hopefully facilitate the development of personalised medicine for patients with COPD.
Acknowledgments
The authors thank the Hokkaido COPD Cohort Study investigators for patient recruitment and follow-up, as well as Hideka Ashikaga, Ayako Kondo and Yuko Takagi of the Central Office of the Hokkaido COPD Cohort Study (Sapporo, Japan) and the staff of Exam Co., Ltd. (Sapporo, Japan) for data management, Tsukasa Sasaki in the Division of Radiology, Department of Diagnosis and Treatment Support, the staff in the Division of Pulmonary Function, Department of Laboratory Medicine, Hokkaido University Hospital for technical support and Yoichi M Ito in Department of Biostatistics, Faculty of Medicine and Graduate School of Medicine, Hokkaido University for advice on the statistical analysis.
References
Footnotes
KS and NT contributed equally.
Contributors KS: study concept and design, statistical analysis, interpretation of data and drafting the manuscript; NT: acquisition of data, statistical analysis, interpretation of data and editing the manuscript; NVT: CT analysis and interpretation of data; MS: interpretation of data and critical revision of the manuscript; HM: acquisition of data and interpretation of data; SS: acquisition of data and interpretation of data and editing the manuscript; SM: acquisition of data and interpretation of data; MM: interpretation of data; TH: interpretation of data; EO, YN: interpretation of data; SK, MN: interpretation of data and finalising of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests The Hokkaido COPD Cohort Study is supported by a scientific research grant to the Hokkaido COPD Cohort Study from the Ministry of Education, Science, Culture and Sports of Japan (17390239 and 2139053 to MN), Nippon Boehringer Ingelheim, Pfizer, and a grant to the Respiratory Failure Research Group from the Ministry of Health, Labour and Welfare, Japan. MS reports grants from GlaxoSmithKline, grants from Novartis and grants from AstraZeneca outside the current work. None of these companies had a role in the design or analysis of the study or in the writing of the manuscript. The Kyoto University Cohort Study was supported by the Japan Society for the Promotion of Science (JSPS) (No 16390234, No 21590964 and No 17H06807) and a grant to the Respiratory Failure Research Group from the Ministry of Health, Labour and Welfare, Japan. NT, SS and TH report a grant from Fujifilm Medical outside the current work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.