
Abstract
Data sources The following electronic databases were searched with no language restrictions: MEDLINE, EMBASE and Cochrane library. Reference lists of included studies were searched, alongside the Open Grey database and hand searches in Journal of Dental Research, Journal of Periodontology, Journal of Clinical Periodontology and Journal of Periodontal Research. The editor of each journal was contacted to enquire about relevant accepted and forthcoming articles.
Study selection Two independent reviewers screened for randomised controlled trials (RCTs) with a follow-up of at least six months. The main outcome was the change in periodontal pocket depths (PPD) and clinical attachment level (CAL) six months after treatment, where patients were divided according to adjunctive treatment (antimicrobial vs placebo) as well as the pre-treatment detection of periodontopathogenic bacteria.
Data extraction and synthesis Data was extracted from all selected papers using a standardised form, including treatment methods, antimicrobial regime and bacterial detection methods. The Cochrane Collaborations tool was used to assess risk of bias. The weighted mean difference (WMD) of treatment effects between bacterial detection groups was obtained and pooled. A two-stage, fixed-effects meta-analysis was performed, and statistical heterogeneity was described using the Q-statistic and I2 index.
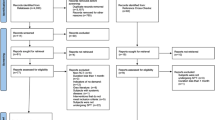
Results Following the screening of 643 papers and author contact, five placebo-controlled studies were included in the systematic review. All had a low risk of bias. They varied in patient sample sizes, periodontal diagnoses, subgingival debridement protocols, antimicrobial regimes, as well as baseline microbial analysis methods. The meta-analysis of four studies, using amoxicillin and metronidazole as adjuncts, revealed a significant increase in the reduction of PPDs compared to placebo. It also showed no significant difference in the clinical effect on PPDs ≥5 mm when prescribing adjunctive amoxicillin and metronidazole based on the pre-treatment detection of A. actinomycetemcomitans (WMD = 1.16, 95% CI [-5.37, 7.68], I2 = 37.8%).
Conclusions Although data on baseline periodontopathogenic bacteria was limited to A. actinomycetemcomitans, this systematic review suggests that there is not enough evidence to support the use of pre-treatment analysis of subgingival bacteria as a criterion for prescribing adjunctive antibiotics.
Similar content being viewed by others

A Commentary on
Nibali L, Koidou V P, Hamborg T, Donos N.
Empirical or microbiologically-guided systemic antimicrobials as adjuncts to non-surgical periodontal therapy? a systematic review. J Clin Periodontol 2019; DOI: 10.1111/jcpe.13164.
Commentary
This paper supports existing evidence, that in certain cases systemic antimicrobials improve the clinical benefits of non-surgical periodontal management.1 Side effects of systemic antibiotics, including risk of allergy/hypersensitivity and rising antibiotic resistance, limit their widespread use as adjunctive periodontal therapy. Personalised medicine, where patients are selected for this treatment according to baseline microbial profiles, could theoretically provide a targeted antimicrobial approach. However, the meta-analysis of the papers included in this review found no support for this approach.2
The authors acknowledge the small number of included studies despite an extensive search of the literature alongside contacting individual authors and journal editors. Sixty-four articles qualified for full text reading but 41 were excluded as no clinical response divided by microbial detection was reported. Although 33 authors were contacted about obtaining relevant data, no response was found for 27 of these potentially relevant studies. The authors stress the value of open access databases to provide more data for secondary analyses such as in this review.
Differences in study methodologies may have had an impact on the overall findings of the systematic review. None of the included studies used differences in clinical response by baseline microbial profile as the main study outcome. Furthermore, subgingival debridement regimes ranged from full-mouth approaches in one session to staged approaches over 14 days, and although metronidazole and amoxicillin were used in four of the studies, dose and duration varied.
Furthermore, target populations included patients with generalised aggressive periodontitis in three studies, and chronic periodontitis in the remaining two studies. Tonetti et al.'s new classification of periodontitis would support pooling together aggressive and chronic periodontitis in the meta-analysis.3 Results seemed consistent even when cases were separated according to disease severity, as is now recommended (mild-moderate-severe). Data was only available on A. actinomycetemcomitans, preventing any conclusions being drawn about other periodontopathogenic bacteria, such as P. gingivalis and T. forsythia. The authors highlight the heterogeneity and lack of sophistication of microbiological analysis impacting on conclusions drawn.
Despite the drive for effective diagnostic microbial testing as we enter the era of personalised medicine, this systematic review suggests there is insufficient evidence to support using baseline detection of periodontopathogenic bacteria to determine the prescription of adjunctive antibiotics.
References
Jepsen K, Jepsen S. Antibiotics/antimicrobials: systemic and local administration in the therapy of mild to moderately advanced periodontitis. Periodontol 2000 2016; 71: 82-112.
Nibali L, Koidou V P, Hamborg T, Donos N. Empirical or microbiologically-guided systemic antimicrobials as adjuncts to non-surgical periodontal therapy? A systematic review. J Clin Periodontol 2019; 46: 999-1012.
Tonetti M S, Greenwell H, Kornman K S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Periodontol 2019; 89 (Suppl 1): S159-S172.
Author information
Authors and Affiliations
Rights and permissions
About this article

Cite this article
Shelswell, J. The clinical benefit of adjunctive antibiotics alongside non-surgical periodontal therapy with respect to periodontopathogenic bacteria?. Evid Based Dent 20, 121–122 (2019). https://doi.org/10.1038/s41432-019-0061-2
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41432-019-0061-2
