Blood Metabolites Associate with Prognosis in Endometrial Cancer

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Cohort Characteristics
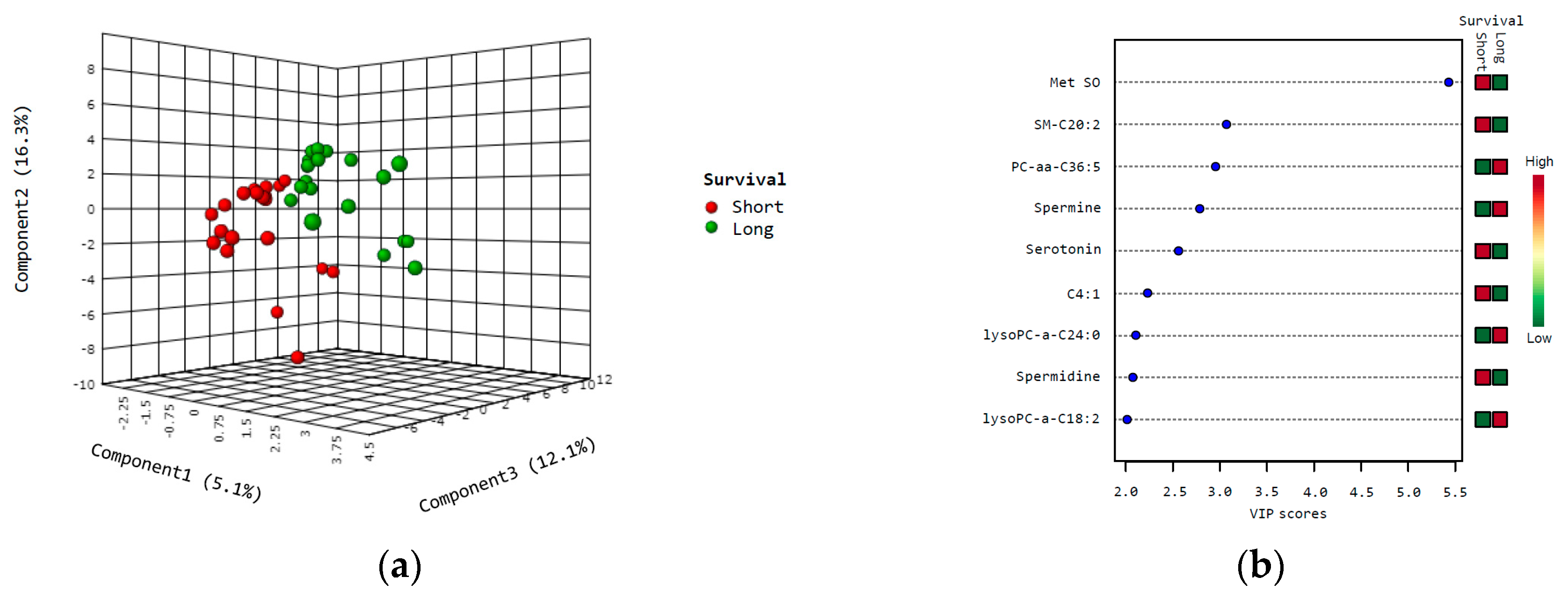
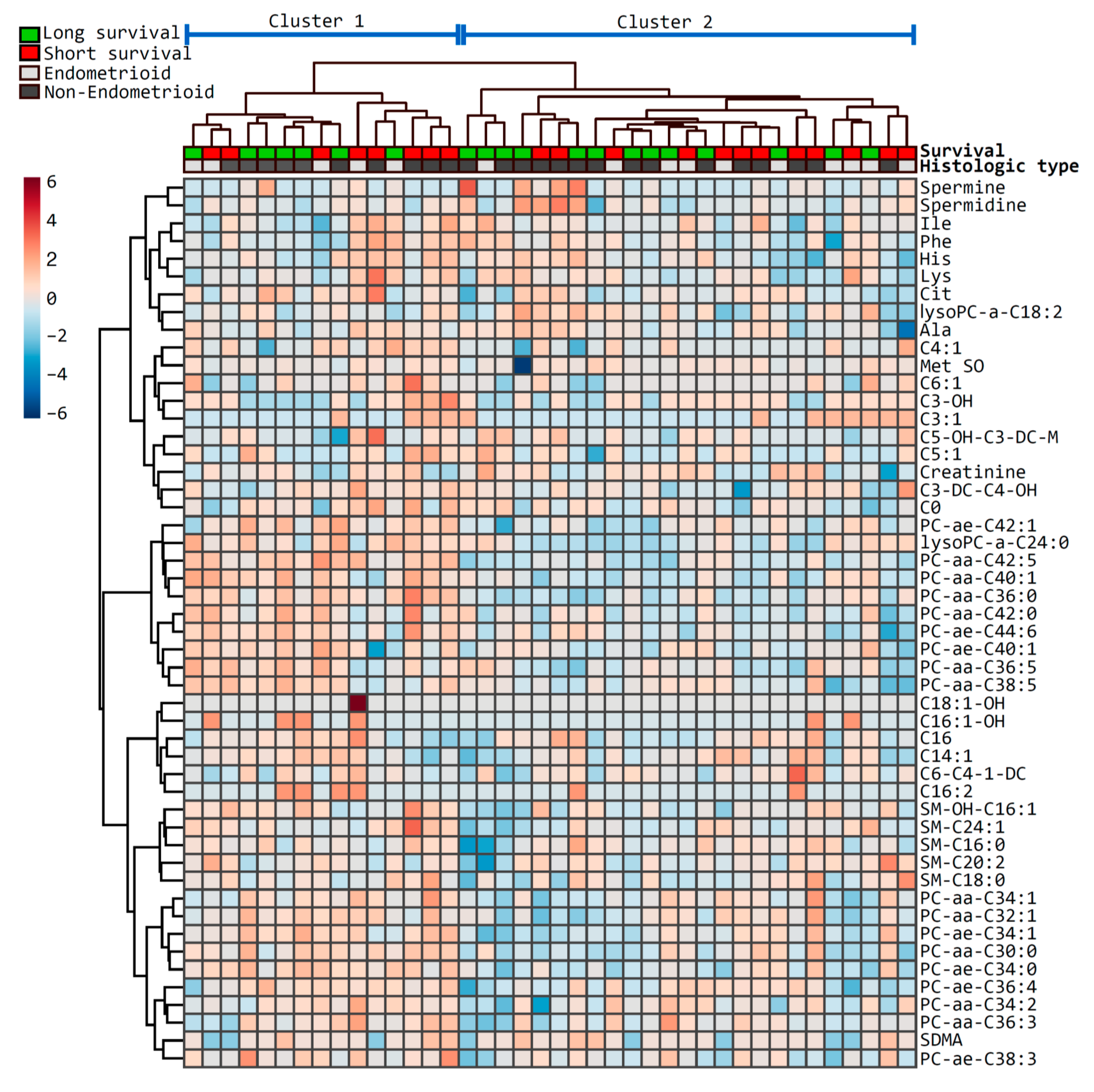
2.2. Metabolites Associate with Survival
2.3. Metabolite Signature Modeling
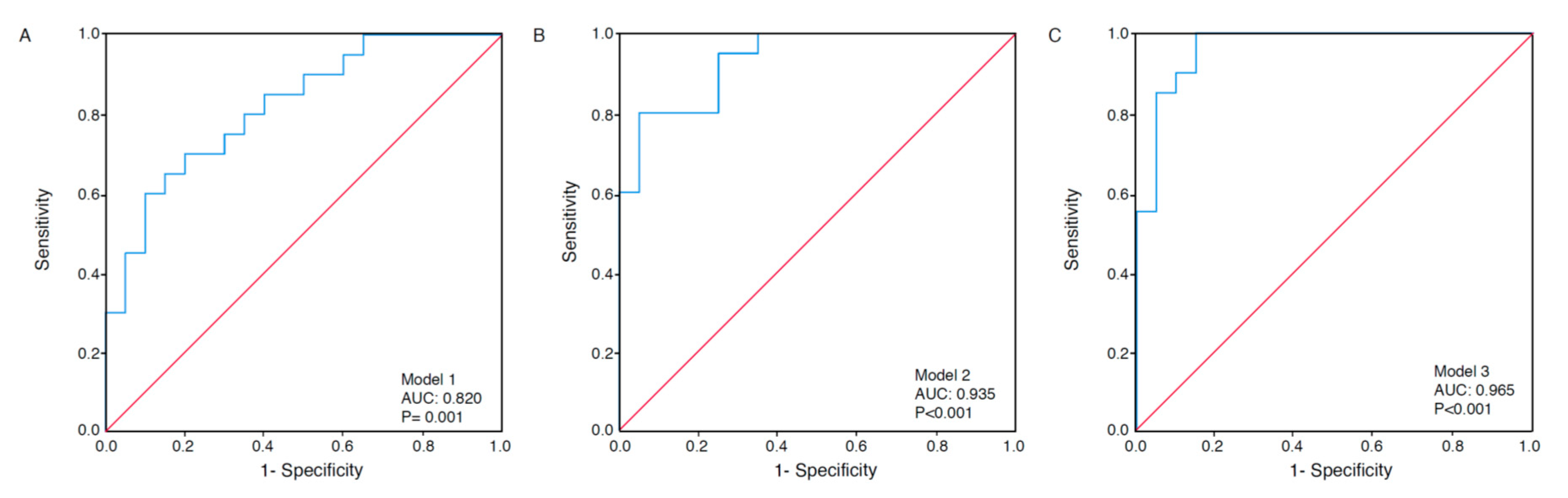
2.4. Receiver Operating Characteristics Analyses
2.5. Pathways Involved
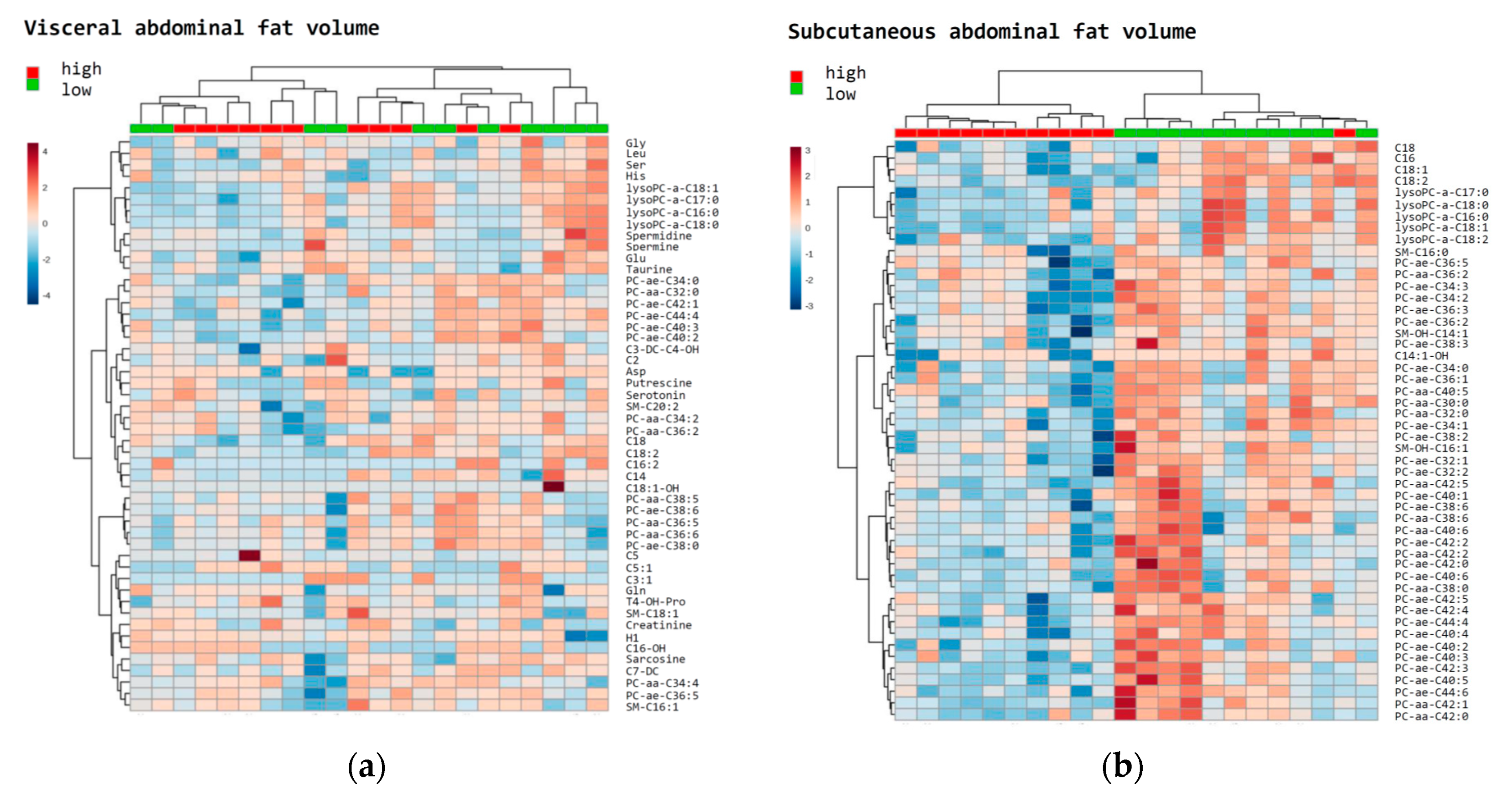
2.6. Metabolites Associated with Abdominal Fat Distribution
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Metabolomic Profiling
4.3. Transcriptomics
4.4. Image Analysis on CT Scans
4.5. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Amant, F.; Moerman, P.; Neven, P.; Timmerman, D.; Van Limbergen, E.; Vergote, I. Endometrial cancer. Lancet 2005, 366, 491–505. [Google Scholar] [CrossRef]
- Morice, P.; Leary, A.; Creutzberg, C.; Abu-Rustum, N.; Darai, E. Endometrial cancer. Lancet 2016, 387, 1094–1108. [Google Scholar] [CrossRef]
- Currie, E.; Schulze, A.; Zechner, R.; Walther, T.C.; Farese, R.V., Jr. Cellular fatty acid metabolism and cancer. Cell Metab. 2013, 18, 153–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlova, N.N.; Thompson, C.B. The Emerging Hallmarks of Cancer Metabolism. Cell Metab. 2016, 23, 27–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauland, K.K.; Eng, O.; Ytre-Hauge, S.; Tangen, I.L.; Berg, A.; Salvesen, H.B.; Salvesen, O.O.; Krakstad, C.; Trovik, J.; Hoivik, E.A.; et al. High visceral fat percentage is associated with poor outcome in endometrial cancer. Oncotarget 2017, 8, 105184–105195. [Google Scholar] [CrossRef] [PubMed]
- Tangen, I.L.; Fasmer, K.E.; Konings, G.F.; Jochems, A.; Delvoux, B.; Xanthoulea, S.; Stokowy, T.; Strand, E.; Berg, H.F.; Auriola, S.; et al. Blood steroids are associated with prognosis and fat distribution in endometrial cancer. Gynecol. Oncol. 2019, 152, 46–52. [Google Scholar] [CrossRef]
- Gowda, G.A.; Zhang, S.; Gu, H.; Asiago, V.; Shanaiah, N.; Raftery, D. Metabolomics-based methods for early disease diagnostics. Expert Rev. Mol. Diagn. 2008, 8, 617–633. [Google Scholar] [CrossRef] [Green Version]
- Chong, J.; Yamamoto, M.; Xia, J. MetaboAnalystR 2.0: From Raw Spectra to Biological Insights. Metabolites 2019, 9, 57. [Google Scholar] [CrossRef] [Green Version]
- Buss, J. Limitations of body mass index to assess body fat. Workplace Health Saf. 2014, 62, 264. [Google Scholar] [CrossRef]
- Ferlay, J.; Shin, H.R.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int. J. Cancer 2010, 127, 2893–2917. [Google Scholar] [CrossRef]
- Bro, R.; Kamstrup-Nielsen, M.H.; Engelsen, S.B.; Savorani, F.; Rasmussen, M.A.; Hansen, L.; Olsen, A.; Tjonneland, A.; Dragsted, L.O. Forecasting individual breast cancer risk using plasma metabolomics and biocontours. Metabolomics 2015, 11, 1376–1380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budczies, J.; Brockmoller, S.F.; Muller, B.M.; Barupal, D.K.; Richter-Ehrenstein, C.; Kleine-Tebbe, A.; Griffin, J.L.; Oresic, M.; Dietel, M.; Denkert, C.; et al. Comparative metabolomics of estrogen receptor positive and estrogen receptor negative breast cancer: Alterations in glutamine and beta-alanine metabolism. J. Proteome. 2013, 94, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Lin, C.C.; Spasojevic, I.; Iversen, E.S.; Chi, J.T.; Marks, J.R. A joint analysis of metabolomics and genetics of breast cancer. Breast Cancer Res. 2014, 16, 415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, S.; Chong, N.; Lewis, N.E.; Jia, W.; Xie, G.; Garmire, L.X. Novel personalized pathway-based metabolomics models reveal key metabolic pathways for breast cancer diagnosis. Genome Med. 2016, 8, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willmann, L.; Schlimpert, M.; Halbach, S.; Erbes, T.; Stickeler, E.; Kammerer, B. Metabolic profiling of breast cancer: Differences in central metabolism between subtypes of breast cancer cell lines. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2015, 1000, 95–104. [Google Scholar] [CrossRef]
- Playdon, M.C.; Ziegler, R.G.; Sampson, J.N.; Stolzenberg-Solomon, R.; Thompson, H.J.; Irwin, M.L.; Mayne, S.T.; Hoover, R.N.; Moore, S.C. Nutritional metabolomics and breast cancer risk in a prospective study. Am. J. Clin. Nutr. 2017, 106, 637–649. [Google Scholar] [CrossRef]
- Wei, S.; Liu, L.; Zhang, J.; Bowers, J.; Gowda, G.A.; Seeger, H.; Fehm, T.; Neubauer, H.J.; Vogel, U.; Clare, S.E.; et al. Metabolomics approach for predicting response to neoadjuvant chemotherapy for breast cancer. Mol. Oncol. 2013, 7, 297–307. [Google Scholar] [CrossRef] [Green Version]
- Yang, K.; Xia, B.; Wang, W.; Cheng, J.; Yin, M.; Xie, H.; Li, J.; Ma, L.; Yang, C.; Li, A.; et al. A Comprehensive Analysis of Metabolomics and Transcriptomics in Cervical Cancer. Sci. Rep. 2017, 7, 43353. [Google Scholar] [CrossRef]
- Hou, Y.; Yin, M.; Sun, F.; Zhang, T.; Zhou, X.; Li, H.; Zheng, J.; Chen, X.; Li, C.; Ning, X.; et al. A metabolomics approach for predicting the response to neoadjuvant chemotherapy in cervical cancer patients. Mol. Biosyst. 2014, 10, 2126–2133. [Google Scholar] [CrossRef] [Green Version]
- Porcari, A.M.; Negrao, F.; Tripodi, G.L.; Pitta, D.R.; Campos, E.A.; Montis, D.M.; Martins, A.M.A.; Eberlin, M.N.; Derchain, S.F.M. Molecular Signatures of High-Grade Cervical Lesions. Front. Oncol. 2018, 8, 99. [Google Scholar] [CrossRef] [Green Version]
- Fan, L.; Zhang, W.; Yin, M.; Zhang, T.; Wu, X.; Zhang, H.; Sun, M.; Li, Z.; Hou, Y.; Zhou, X.; et al. Identification of metabolic biomarkers to diagnose epithelial ovarian cancer using a UPLC/QTOF/MS platform. Acta Oncol. 2012, 51, 473–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plewa, S.; Horala, A.; Derezinski, P.; Klupczynska, A.; Nowak-Markwitz, E.; Matysiak, J.; Kokot, Z.J. Usefulness of Amino Acid Profiling in Ovarian Cancer Screening with Special Emphasis on Their Role in Cancerogenesis. Int. J. Mol. Sci. 2017, 18, 2727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, H.; Hou, Y.; Cheng, J.; Openkova, M.S.; Xia, B.; Wang, W.; Li, A.; Yang, K.; Li, J.; Xu, H.; et al. Metabolic profiling and novel plasma biomarkers for predicting survival in epithelial ovarian cancer. Oncotarget 2017, 8, 32134–32146. [Google Scholar] [CrossRef] [PubMed]
- Kyriakides, M.; Rama, N.; Sidhu, J.; Gabra, H.; Keun, H.C.; El-Bahrawy, M. Metabonomic analysis of ovarian tumour cyst fluid by proton nuclear magnetic resonance spectroscopy. Oncotarget 2016, 7, 7216–7226. [Google Scholar] [CrossRef]
- Bharti, S.K.; Wildes, F.; Hung, C.F.; Wu, T.C.; Bhujwalla, Z.M.; Penet, M.F. Metabolomic characterization of experimental ovarian cancer ascitic fluid. Metabolomics 2017, 13, 113. [Google Scholar] [CrossRef]
- Altadill, T.; Dowdy, T.M.; Gill, K.; Reques, A.; Menon, S.S.; Moiola, C.P.; Lopez-Gil, C.; Coll, E.; Matias-Guiu, X.; Cabrera, S.; et al. Metabolomic and Lipidomic Profiling Identifies the Role of the RNA Editing Pathway in Endometrial Carcinogenesis. Sci. Rep. 2017, 7, 8803. [Google Scholar] [CrossRef]
- Troisi, J.; Sarno, L.; Landolfi, A.; Scala, G.; Martinelli, P.; Venturella, R.; Di Cello, A.; Zullo, F.; Guida, M. Metabolomic Signature of Endometrial Cancer. J. Proteom. Res. 2018, 17, 804–812. [Google Scholar] [CrossRef]
- Gaudet, M.M.; Falk, R.T.; Stevens, R.D.; Gunter, M.J.; Bain, J.R.; Pfeiffer, R.M.; Potischman, N.; Lissowska, J.; Peplonska, B.; Brinton, L.A.; et al. Analysis of serum metabolic profiles in women with endometrial cancer and controls in a population-based case-control study. J. Clin. Endocrinol. Metab. 2012, 97, 3216–3223. [Google Scholar] [CrossRef]
- Audet-Delage, Y.; Villeneuve, L.; Gregoire, J.; Plante, M.; Guillemette, C. Identification of Metabolomic Biomarkers for Endometrial Cancer and Its Recurrence after Surgery in Postmenopausal Women. Front. Endocrinol. 2018, 9, 87. [Google Scholar] [CrossRef] [Green Version]
- Jove, M.; Gatius, S.; Yeramian, A.; Portero-Otin, M.; Eritja, N.; Santacana, M.; Colas, E.; Ruiz, M.; Pamplona, R.; Matias-Guiu, X. Metabotyping human endometrioid endometrial adenocarcinoma reveals an implication of endocannabinoid metabolism. Oncotarget 2016, 7, 52364–52374. [Google Scholar] [CrossRef] [Green Version]
- Eritja, N.; Jove, M.; Fasmer, K.E.; Gatius, S.; Portero-Otin, M.; Trovik, J.; Krakstad, C.; Sol, J.; Pamplona, R.; Haldorsen, I.S.; et al. Tumour-microenvironmental blood flow determines a metabolomic signature identifying lysophospholipids and resolvin D as biomarkers in endometrial cancer patients. Oncotarget 2017, 8, 109018–109026. [Google Scholar] [CrossRef] [PubMed]
- Knific, T.; Vouk, K.; Smrkolj, S.; Prehn, C.; Adamski, J.; Rizner, T.L. Models including plasma levels of sphingomyelins and phosphatidylcholines as diagnostic and prognostic biomarkers of endometrial cancer. J. Steroid. Biochem. Mol. Biol 2018, 178, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Shao, X.; Wang, K.; Liu, X.; Gu, C.; Zhang, P.; Xie, J.; Liu, W.; Sun, L.; Chen, T.; Li, Y. Screening and verifying endometrial carcinoma diagnostic biomarkers based on a urine metabolomic profiling study using UPLC-Q-TOF/MS. Clin. Chim. Acta Int. J. Clin. Chem. 2016, 463, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Siskos, A.P.; Jain, P.; Romisch-Margl, W.; Bennett, M.; Achaintre, D.; Asad, Y.; Marney, L.; Richardson, L.; Koulman, A.; Griffin, J.L.; et al. Interlaboratory Reproducibility of a Targeted Metabolomics Platform for Analysis of Human Serum and Plasma. Anal. Chem. 2017, 89, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Riekeberg, E.; Powers, R. New frontiers in metabolomics: From measurement to insight. F1000Res 2017, 6, 1148. [Google Scholar] [CrossRef] [Green Version]
- Gunther, U.L. Metabolomics Biomarkers for Breast Cancer. Pathobiology 2015, 82, 153–165. [Google Scholar] [CrossRef]
- Clish, C.B. Metabolomics: An emerging but powerful tool for precision medicine. Cold Spring Harb. Mol. Case. Stud. 2015, 1, a000588. [Google Scholar] [CrossRef] [Green Version]
- Buhtoiarova, T.N.; Brenner, C.A.; Singh, M. Endometrial Carcinoma: Role of Current and Emerging Biomarkers in Resolving Persistent Clinical Dilemmas. Am. J. Clin. Pathol. 2016, 145, 8–21. [Google Scholar] [CrossRef]
- Ussher, J.R.; Elmariah, S.; Gerszten, R.E.; Dyck, J.R. The Emerging Role of Metabolomics in the Diagnosis and Prognosis of Cardiovascular Disease. J. Am. Coll. Cardiol. 2016, 68, 2850–2870. [Google Scholar] [CrossRef]
- Martinez, Y.; Li, X.; Liu, G.; Bin, P.; Yan, W.; Mas, D.; Valdivie, M.; Hu, C.A.; Ren, W.; Yin, Y. The role of methionine on metabolism, oxidative stress, and diseases. Amino. Acids 2017, 49, 2091–2098. [Google Scholar] [CrossRef]
- Zhang, N. Role of methionine on epigenetic modification of DNA methylation and gene expression in animals. Anim. Nutr. 2018, 4, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Koc, A.; Gladyshev, V.N. Methionine sulfoxide reduction and the aging process. Ann. N. Y. Acad. Sci. 2007, 1100, 383–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, B.; Cavigiolio, G.; Brot, N.; Oda, M.N.; Heinecke, J.W. Methionine oxidation impairs reverse cholesterol transport by apolipoprotein A-I. Proc. Natl. Acad. Sci. USA 2008, 105, 12224–12229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, B.; Moskovitz, J. The Functions of the Mammalian Methionine Sulfoxide Reductase System and Related Diseases. Antioxidants 2018, 7, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vander Heiden, M.G.; Cantley, L.C.; Thompson, C.B. Understanding the Warburg effect: The metabolic requirements of cell proliferation. Science 2009, 324, 1029–1033. [Google Scholar] [CrossRef] [Green Version]
- Dash, P.K.; Hergenroeder, G.W.; Jeter, C.B.; Choi, H.A.; Kobori, N.; Moore, A.N. Traumatic Brain Injury Alters Methionine Metabolism: Implications for Pathophysiology. Front. Syst. Neurosci. 2016, 10, 36. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Saito, T.; Tanaka, R.; Satohisa, S.; Adachi, K.; Horie, M.; Akashi, Y.; Kudo, R. Hypermethylation in promoter region of retinoic acid receptor-beta gene and immunohistochemical findings on retinoic acid receptors in carcinogenesis of endometrium. Cancer Lett. 2005, 219, 33–40. [Google Scholar] [CrossRef]
- Wolf, G. Retinoic acid activation of peroxisome proliferation-activated receptor delta represses obesity and insulin resistance. Nutr. Rev. 2010, 68, 67–70. [Google Scholar] [CrossRef]
- Ryall, J.G.; Cliff, T.; Dalton, S.; Sartorelli, V. Metabolic Reprogramming of Stem Cell Epigenetics. Cell Stem Cell 2015, 17, 651–662. [Google Scholar] [CrossRef] [Green Version]
- Kamphorst, J.J.; Cross, J.R.; Fan, J.; de Stanchina, E.; Mathew, R.; White, E.P.; Thompson, C.B.; Rabinowitz, J.D. Hypoxic and Ras-transformed cells support growth by scavenging unsaturated fatty acids from lysophospholipids. Proc. Natl. Acad. Sci. USA 2013, 110, 8882–8887. [Google Scholar] [CrossRef] [Green Version]
- Nieman, K.M.; Kenny, H.A.; Penicka, C.V.; Ladanyi, A.; Buell-Gutbrod, R.; Zillhardt, M.R.; Romero, I.L.; Carey, M.S.; Mills, G.B.; Hotamisligil, G.S.; et al. Adipocytes promote ovarian cancer metastasis and provide energy for rapid tumor growth. Nat. Med. 2011, 17, 1498–1503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rysman, E.; Brusselmans, K.; Scheys, K.; Timmermans, L.; Derua, R.; Munck, S.; Van Veldhoven, P.P.; Waltregny, D.; Daniels, V.W.; Machiels, J.; et al. De novo lipogenesis protects cancer cells from free radicals and chemotherapeutics by promoting membrane lipid saturation. Cancer Res. 2010, 70, 8117–8126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wajchenberg, B.L. Subcutaneous and visceral adipose tissue: Their relation to the metabolic syndrome. Endocr. Rev. 2000, 21, 697–738. [Google Scholar] [CrossRef] [PubMed]
- Trovik, J.; Wik, E.; Stefansson, I.M.; Marcickiewicz, J.; Tingulstad, S.; Staff, A.C.; Njolstad, T.S.; MoMaTec Study, G.; Vandenput, I.; Amant, F.; et al. Stathmin overexpression identifies high-risk patients and lymph node metastasis in endometrial cancer. Clin. Cancer Res. 2011, 17, 3368–3377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramsay, S.L.; Stoeggl, W.M.; Weinberger, K.M.; Graber, A.; Guggenbichler, W. Apparatus and method for analyzing a metabolite profile. In United States Patent; US. Biocrates Life Sciences AG: Innsbruck, Austria, 2012. [Google Scholar]
- Berg, A.; Fasmer, K.E.; Mauland, K.K.; Ytre-Hauge, S.; Hoivik, E.A.; Husby, J.A.; Tangen, I.L.; Trovik, J.; Halle, M.K.; Woie, K.; et al. Tissue and imaging biomarkers for hypoxia predict poor outcome in endometrial cancer. Oncotarget 2016, 7, 69844–69856. [Google Scholar] [CrossRef] [PubMed]
- Maurovich-Horvat, P.; Massaro, J.; Fox, C.S.; Moselewski, F.; O’Donnell, C.J.; Hoffmann, U. Comparison of anthropometric, area- and volume-based assessment of abdominal subcutaneous and visceral adipose tissue volumes using multi-detector computed tomography. Int. J. Obes. 2007, 31, 500–506. [Google Scholar] [CrossRef] [Green Version]
- Xia, J.; Wishart, D.S. Using MetaboAnalyst 3.0 for Comprehensive Metabolomics Data Analysis. Curr. Protoc. Bioinform. 2016, 55, 14.10.11–14.10.91. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Cohort (n = 40) | Long Survival (n = 20) | Short Survival (n = 20) | p† |
|---|---|---|---|---|
| Age (years) | 72.0 (61.0, 78.5) | 67.0 (56.0, 77.0) | 75.0 (63.5, 81.5) | 0.10 |
| Body Mass Index (BMI, kg/m2) | 24.0 (23.0, 27.0) | 24.0 (22.0, 26.5) | 26.0 (23.0, 27.0) | 0.20 |
| Recurrence Free Survival (months) | 28.5 (9.5, 66.0) | 66.0 (60.0, 70.5) | 9.5 (3.50, 14.5) | <0.001 |
| Recurrence, n (%) | 21 (52.5) | 1 (5.0) | 20 (100) | <0.001 |
| Follow-up Time (months) | 36.0 (16.5, 66.0) | 66.0 (60.0, 70.5) | 16.5 (8.5, 27.0) | <0.001 |
| Myometrial Infiltration ≥50%, n (%) | 19 (47.5) | 6 (30.0) | 13 (65.0) | 0.03 |
| Histologic Type, n (%) | ||||
| Endometrioid Type | 15 (37.5) | 7 (35.0) | 8 (40.0) | 0.74 |
| Non-endometrioid Type | ||||
| Clear Cell | 3 (7.5) | 3 (15.0) | 0 (0) | 0.07 |
| Serous Papillary | 8 (20.0) | 3 (15.0) | 5 (25.0) | 0.43 |
| Carcinosarcoma | 11 (27.5) | 6 (30.0) | 5 (25.0) | 0.72 |
| Other non-endometrioid | 3 (7.5) | 1 (5.0) | 2 (10.0) | 0.55 |
| Histologic Grade, n (%) # | ||||
| Grade 1 | 6 (15.0) | 3 (15.0) | 3 (15.0) | 1.00 |
| Grade 2 | 4 (10.0) | 2 (10.0) | 2 (10.0) | 1.00 |
| Grade 3 | 5 (12.5) | 2 (10.0) | 3 (15.0) | 1.00 |
| FIGO Stage, n (%) | ||||
| Stage I | 36 (90.0) | 18 (90.0) | 18 (90.0) | 1.00 |
| Stage II | 4 (10.0) | 2 (10.0) | 2 (10.0) | 1.00 |
| Metabolite | Total Cohort (n = 40) | Long Survival (n = 20) | Short Survival (n = 20) | p† | VIP Score # |
|---|---|---|---|---|---|
| Amino Acids and Biogenic Amines (µM) | |||||
| Asp 3 | 7.1 (5.9, 8.5) | 6.8 (6.1, 7.9) | 7.6 (5.8, 9.1) | 0.76 | 5.32 |
| ADMA 3 | 0.55 (0.30, 0.70) | 0.50 (0.30, 0.80) | 0.60 (0.30, 0.65) | 0.90 | 2.93 |
| Met SO 1 | 1.20 (1.00, 1.50) | 1.05 (0.90, 1.25) | 1.40 (1.10, 1.55) | 0.01 | 5.43 |
| Serotonin 1 | 0.75 (0.45, 1.25) | 0.65 (0.45, 1.35) | 0.90 (0.45, 1.25) | 0.78 | 2.67 |
| Spermidine 2 | 0.30 (0.30, 0.40) | 0.30 (0.20, 0.40) | 0.40 (0.30, 0.40) | 0.17 | 2.08 |
| Spermine 1** | 0.20 (0.20, 0.30) | 0.20 (0.20, 0.30) | 0.20 (0.20, 0.30) | 0.62 | 2.79 |
| Acylcarnitines (µM) | |||||
| C3-OH 1** | 0.027 (0.023, 0.030) | 0.026 (0.023, 0.028) | 0.028 (0.025, 0.034) | 0.04 | 1.63 |
| C4:1 2** | 0.023 (0.018, 0.026) | 0.022 (0.017, 0.025) | 0.023 (0.020, 0.027) | 0.22 | 2.23 |
| Sugar (µM) | |||||
| Hexose H1 3 | 4051 (2915, 4868) | 3776 (2915, 4714) | 4098 (3014, 5385) | 0.75 | 2.62 |
| Glycerophospholipids and Sphingolipids (µM) | |||||
| lysoPC-a-C18:2 2 | 27.0 (21.5, 35.6) | 32.1 (22.3, 36.0) | 25.3 (18.7, 35.3) | 0.29 | 2.01 |
| lysoPC-a-C24:0 2 | 0.38 (0.20, 0.54) | 0.42 (0.20, 0.59) | 0.36 (0.20, 0.52) | 0.33 | 2.11 |
| PC-aa-C36:5 1 | 39.4 (27.7, 56.9) | 42.7 (38.2, 57.0) | 30.2 (24.4, 55.0) | 0.07 | 2.95 |
| PC-ae-C30:1 3 | 0.026 (0.00, 0.12) | 0.025 (0.00, 0.098) | 0.026 (0.00, 0.15) | 0.69 | 2.16 |
| SM-C20:2 1 | 0.59 (0.43, 0.69) | 0.57 (0.33, 0.65) | 0.60 (0.47, 0.77) | 0.16 | 3.07 |
| Abdominal Fat Estimates | Total Cohort (n = 22) | Long Survival (n = 10) | Short Survival (n = 12) | p† |
|---|---|---|---|---|
| TAV (cm3) | 6933 (5654, 8746) | 7131 (6534, 8746) | 6758 (5373, 8683) | 0.64 |
| VAV (cm3) | 2388 (1920, 3916) | 2666 (2086, 3461) | 2219 (1905, 3919) | 0.74 |
| SAV (cm3) | 4151 (3329, 5389) | 4437 (3916, 5923) | 3980 (3263, 5252) | 0.55 |
| VAV% | 37.4 (33.4, 43.5) | 37.1 (31.3, 40.3) | 38.0 (35.0, 45.7) | 0.45 |
| Waist Circumference (cm) | 93.2 (86.2, 99.1) | 91.6 (86.0, 95.9) | 97.3 (87.0, 99.2) | 0.34 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strand, E.; Tangen, I.L.; Fasmer, K.E.; Jacob, H.; Halle, M.K.; Hoivik, E.A.; Delvoux, B.; Trovik, J.; Haldorsen, I.S.; Romano, A.; et al. Blood Metabolites Associate with Prognosis in Endometrial Cancer. Metabolites 2019, 9, 302. https://doi.org/10.3390/metabo9120302
Strand E, Tangen IL, Fasmer KE, Jacob H, Halle MK, Hoivik EA, Delvoux B, Trovik J, Haldorsen IS, Romano A, et al. Blood Metabolites Associate with Prognosis in Endometrial Cancer. Metabolites. 2019; 9(12):302. https://doi.org/10.3390/metabo9120302
Chicago/Turabian StyleStrand, Elin, Ingvild L. Tangen, Kristine E. Fasmer, Havjin Jacob, Mari K. Halle, Erling A. Hoivik, Bert Delvoux, Jone Trovik, Ingfrid S. Haldorsen, Andrea Romano, and et al. 2019. "Blood Metabolites Associate with Prognosis in Endometrial Cancer" Metabolites 9, no. 12: 302. https://doi.org/10.3390/metabo9120302