
Abstract
Study design
Observational cohort study
Objectives
To investigate preoperative factors that predict fair outcomes following surgery in patients with proximal cervical spondylotic amyotrophy (CSA) using electrophysiological and neurological findings.
Setting
Yamaguchi University
Methods
54 patients with proximal CSA who underwent surgical treatment of the cervical spine were enrolled. Erb-point stimulated compound muscle action potentials (CMAP) were recorded from the deltoid and biceps brachii muscles. We computed the ratio of affected to normal side CMAP amplitudes in two muscles (deltoid and biceps brachii) and regarded the mean ratio (CMAP-R) as representing the severity of neural involvement. Pre- and postoperative strengths of the most atrophic muscles were evaluated using manual muscle testing. Improvements in strength were classified as excellent (5 grades recovered), good (more than one grade recovered), fair (no improvement), or poor (worsened).
Results
Surgical outcomes were excellent in 26 patients, good in five, fair in 16, poor in seven. Patients with fair outcomes had lower CMAP-R than those patients with excellent and good outcomes [P = 0.0099, odds ratio = 0.89 (95% confidence interval, 0.81−0.97; for a change of 10%)]. Eight patients (15%) had a C5 palsy.
Conclusions
CMAP-R could be used as a reliable predictive factor related to a fair surgical outcome. We must pay attention to the incidence of C5 palsy after surgery.
Similar content being viewed by others

Introduction
Cervical spondylotic amyotrophy (CSA) is a subtype of cervical spondylotic myelopathy characterized by muscle weakness and atrophy in the upper extremities with no or insignificant sensory deficit and gait disturbance [1]. Based on the affected muscles in the upper extremities, CSA is classified into the proximal (scapular, deltoid, and biceps brachii muscles) and distal (triceps, forearm, and hand muscles) types [2]. We have previously reported surgical outcomes and pathologies of proximal CSA using compound muscle action potentials (CMAP) for deltoid and biceps brachii muscles and central motor conduction time (CMCT) [3]. We have suggested that surgery of the cervical spine should be performed in patients in whom the mean ratio of affected to normal side CMAP amplitudes (CMAP-R) recorded in deltoid and biceps brachii muscles ranged from 30 to 50% [3]. When we chose surgical treatment for some patients, some patients still had fair or poor outcomes [3]. The preoperative factors related to fair outcomes remain unclear. We collected data on age, surgical approach, duration of clinical history (DCH), duration of postoperative follow-up (DPF), high intensity area on T2-weighted magnetic resonance imaging (MRI), the number of levels of spinal cord compression, electrophysiological findings, and neurological findings. The aim of this study were to evaluate surgical outcomes in patients with proximal CSA and to investigate preoperative factors that predict fair outcomes following surgery in patients with proximal CSA using electrophysiological examination and neurological findings. In our previous study using a univariate analysis, we have shown that the CMAP-R significantly correlated with postoperative recovery [3]. In the current study, we investigated the values of CMAP-R and other collected data in 54 patients with proximal CSA (to date, case series with the largest sample size) using a multivariate analysis to confirm the predictive factors of surgical outcome.
Methods
A retrospective study was performed for 54 patients with proximal CSA who underwent surgical treatment of the cervical spine between April 1997 and July 2016 at our hospital. Mean (SD) age was 61.4 ± 10.0 years and median DCH before electrophysiological examination was 8.5 months (Interquartile range, 4–13.5). Median DPF was 46 months (Interquartile range, 12.5–60). Anterior approach was the preferred method of treatment for multilevel cervical myelopathy when less than three surgical segments were involved. The posterior approach was the preferred method of treatment for multilevel cervical myelopathy when the involved surgical segments were equal to three or more. When the alignment of the cervical spine was kyphosis, we added fixation with instrumentation (Table 1). All 54 patients showed severe unilateral atrophy of the shoulder girdle muscles but the intrinsic muscles remained intact. We excluded patients with bilateral atrophy of the shoulder girdle muscles.
When patients had muscle atrophy of the fore arm and/or hand in addition to the shoulder girdle muscles, we suspected amyotrophic lateral sclerosis (ALS) and other motor neuron diseases. To differentiate motor neuron diseases, such as ALS and CSA, we performed preoperative electromyography (EMG) in almost all patients. EMG features of chronic neurogenic change must be found in patients with ALS, for example. (A) Motor unit potentials of increased amplitude and increased duration, usually with an increased number of phases, as assessed by qualitative or quantitative studies. (B) Decreased motor unit recruitment, defined by rapid firing of a reduced number of motor units. (C) Using a narrow band pass filter (500 Hz to 5 kHz) unstable and complex motor unit potentials will be observed [4]. When ALS and other motor neuron diseases were suspected, we consulted neurologists preoperatively. We and the neurologists determined that patients with CSA did not suffer from these diseases preoperatively. This study was approved by the institutional review board at our hospital (H29-216).
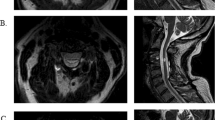
Assessment of the degree of spinal cord compression
Presence of high intensity area in the spinal cord and the number of levels of spinal cord compression were evaluated using axial and sagittal T2-weighted MRI.
Assessment of muscle strength
Pre- and postoperative strengths of the most atrophic muscles were evaluated using manual muscle testing (MMT). Four surgeons who were certificated by The Japanese Society for Spine Surgery and Related Research evaluated MMT at the first medical examination and the latest follow-up. Two of four surgeons (authors: YI, NN, MF, and HS) evaluated one patient. Improvements in strength were classified as excellent (5 grades recovered by MMT), good (more than one grade recovered by MMT), fair (no improvement by MMT), or poor (worsened by MMT).
Measurement of CMCT
Self-adhesive surface recording electrodes were placed on the abductor digiti minimi muscle using a standard belly–tendon method. Motor evoked potentials (MEP) from the abductor digiti minimi were recorded during voluntary contraction. Transcranial magnetic stimulation was delivered using a round 14-cm outer diameter coil (Magstim, Machida City, Tokyo). Magnetic stimulus intensity was set at 20% above the threshold of the MEP during voluntary contraction. Voluntary contraction of muscles enhanced MEP amplitudes and shortens the latencies [5]. The effect of increasing voluntary muscle contraction on the CMCT and MEP amplitudes to establish the importance of standardization of the facilitation of central motor conduction measured by magnetic stimulation [6]. Muscle force was indirectly assessed from the integrated electrical muscle activity and expressed as the root mean square and varied from 0 to 40% of maximal activity. The CMCT decreased during increasing muscle contraction, reaching constant values at ∼10–20% the root mean square max.
CMAP and F-waves were also recorded following supramaximal electric stimulation (square wave 0.2 ms) of the ulnar nerve at the wrist. Sixteen serial responses were obtained and the shortest latency of the F-waves was measured. All muscle responses were amplified, filtered by 5–5000 Hz, and recorded using standard EMG (Viking Select: Nicolet Biomedical Madison, WI, USA). The peripheral motor conduction time, excluding the turnaround time at the spinal motor neuron (1 ms), was calculated from the latencies of the CMAPs and F-waves as follows: (latency of CMAP + latency of F-waves − 1)/2 [7]. Conduction time from the motor cortex to the spinal motor neurons (i.e., CMCT) was calculated by subtracting the peripheral motor conduction time from the onset latency of MEP.
Measurement of CMAP
Two authors (YI and MF) who were certificated by The Japanese Society of Clinical Neurophysiology tested CMAP. One of two authors evaluated one patient. Erb-point stimulated CMAP were recorded in the deltoid and biceps in all patients preoperatively. A disc electrode (diameter, 11 mm) was placed over the middle of the deltoid as an active electrode, on the acromion as a reference electrode in the deltoid, over the middle of the biceps brachii muscle, and on the lateral epicondyle of the humerus in the biceps brachii muscle. The underlying skin had been treated with an abrasive solution to reduce impedance and a ground strap was wrapped around the elbow. The bipolar stimulator probe provided a pair of bare metal contacts (diameter, 3 mm) with an adjustable interelectrode distance of 25 mm in our study. Stimulus intensity was gradually increased until the size of the recorded response was no longer altered. Measurement of CMAP included the negative peak amplitude from baseline to peak. The percent amplitude of CMAP was calculated in comparison with the contralateral side.
Statistical analysis
Statistical analyses were performed using general purpose statistical software (StatFlex version 6.0; Artech Co, Ltd, Osaka, Japan; http://www.statflex.net/).
Preoperative parameters examined as possibly associated with the surgical outcomes, included surgical approaches (anterior approach versus posterior approach), CMAP-R, a ratio of affected to normal side CMAP amplitudes in deltoid muscle (CMAP-RD), a ratio of affected to normal side CMAP amplitudes in biceps brachii muscle (CMAP-RB), age, DCH, DPF, MMT of the deltoid on the affected and normal sides, MMT of the biceps brachii on the affected (MMT-BA) and normal (MMT-BN) sides, CMAP amplitudes of the deltoid and the biceps brachii on the affected and normal sides, high intensity area on T2-weighted MRI, and the number of levels of spinal cord compression. Univariate statistical analyses were performed using the Mann–Whitney U test for the comparison of numerical parameters, and the chi-square test for the categorical parameters. To identify the preoperative factors associated with fair versus good/excellent outcomes, multivariate logistic regression analysis (MLRA) was performed by a stepwise parameter selection procedure by setting P < 0.1 as a criterion for inclusion in the regression model. The probability of patients belonging to the fair group (p) was computed from the following formula using the partial regression coefficients (β0, β1, β2, ..., βk) for explanatory variables (X1, X2, ..., Xk), where k represents the number of explanatory parameters included in the regression model.
In this study, a dummy variable indicating the occurrence of fair outcome was set as the objective variable and all the above parameters as the explanatory variables. Sensitivity, specificity, and area under curve (AUC) of the receiver operating characteristic (ROC) curve were calculated for assessing the utility of explanatory parameters for the prediction.
Results
Surgical outcomes were excellent in 26 patients, good in five, fair in 16, and poor in seven.
MRI
22 patients [excellent, nine; good, two; fair, eight; poor, three] showed high intensity area on T2- weighted MRI. The mean number of levels of spinal cord compression was 2.0 (range, 0–4) [excellent, 1.8 (range, 0–3); good, 2.0 (range, 1–3); fair, 2.1 (range, 0–3); and poor, 3.0 (range, 2–4)].
CMAP
CMAP was performed for all 54 patients (Fig. 1). CMAP-R was significantly higher for patients with excellent, good, and poor outcomes than with fair outcomes (p < 0.05). CMAP-RD and CMAP-RB were significantly higher in patients with excellent and poor outcomes than with fair outcomes (P < 0.05). CMAP amplitudes of the deltoid on the affected side was significantly higher for patients with excellent and poor outcomes than with fair outcomes (P < 0.05). CMAP amplitudes of the biceps brachii on the affected side was significantly higher for patients with excellent and poor outcomes than with fair outcomes (P < 0.05). CMAP amplitudes of the deltoid on the normal side were not significantly different among the groups (P > 0.05). CMAP amplitudes of the biceps brachii on the normal side were significantly lower in patients with excellent and fair outcomes than with poor outcomes (P < 0.05).

Relationship between surgical outcome and electrophysiological examination. CMAP-R a mean of affected to normal side CMAP amplitudes ratios recorded in two muscles (deltoid and biceps brachii), CMAP-RD a ratio of affected to normal side CMAP amplitudes in deltoid muscle, CMAP-RB a ratio of affected to normal side CMAP amplitudes in biceps brachii muscle, CMAP compound muscle action potentials, CMCT central motor conduction time
Surgical outcome and CMAP-R are shown in Fig. 2. Apart from seven patients with poor outcomes, 16, 3, and 2 among those with CMAP-R >30% showed excellent, good, and fair outcomes, respectively, compared with 10, 2, and 14, respectively, among those with CMAP-R from 15 to 30%. All patients with CMAP-R of <15% displayed fair outcomes.

The relationship between surgical outcome and CMAP-R. CMAP-R a mean of affected to normal side CMAP amplitudes ratios recorded in two muscles (deltoid and biceps brachii), CMAP compound muscle action potentials, the box plots represented the mean value (vertical line) ± SE
CMCT on the affected side
CMCT was evaluated in 49 patients (Fig. 1). No significant difference was seen among the categories of surgical outcomes. Surgical outcome and CMCT are shown in Fig. 3.

The relationship between surgical outcome and CMCT on the affected side. The thick line showed CMCT was 6.8 ms. CMCT central motor conduction time, the box plots represented the mean value (vertical line) ± SE
Association between fair outcome and preoperative factors
We classified surgical outcomes into two groups after excluding patients with poor outcomes. Patients with excellent and good outcomes were classified as Group EG, and those with a fair outcome as Group F. We used univariate analyses to compare the preoperative parameters listed in the Methods between the two groups. CMAP-R, CMAP-RD, CMAP-RB, DCH, MMT-BA, and BN, and CMAP amplitude of the biceps brachii on the affected side differed significantly between Group F and Group EG (P < 0.05; Table 2). No significant difference between two groups was seen in the number of the compressed levels and the presence of high intensity area.
Preoperative factors in Group F
In the MLRA, the dummy variable representing Group F was set as the objective variable and all preoperative factors were set as explanatory variables. Using the stepwise method, patients with fair outcomes had lower CMAP-R than those patients with excellent and good outcomes [P = 0.0099, odds ratio (OR) = 0.89 (95% confidence interval, 0.81–0.97; for a change of 10%)], but DCH and MMT-BA did not show significances of P = 0.2203 and P = 0.0643, respectively (Table 3).
Based on the predicted probabilities, ROC analysis was performed together with individual parameters of CMAP-R, MMT-BA, and DCH for comparison. The AUC of the predicted probability was 0.887, while those of individual parameters were 0.853, 0.734, and 0.666, respectively (Fig. 4). The cutoff value computed for CMAP-R was computed as 25%, at which sensitivity of detecting Group EG gets equal to specificity of detecting Group F.

ROC curves for CMAP-R, DCH, and MMT-BA in predicting Group F status postoperatively. The AUC of the predicted probability was 0.887, while those of individual parameters were 0.853 for CMAP-R, 0.734 for DCH, and 0.666 for MMT-BA, respectively. ROC receiver operating characteristic, CMAP-R a mean of affected to normal side CMAP amplitudes ratios recorded in two muscles (deltoid and biceps brachii), PP predicted probability, DCH duration of clinical history, MMT-BA MMT of biceps brachii on the affected side, AUC area under curve
Patients with poor outcomes
Eight patients (15%) had a C5 palsy. Paralysis was noted after a mean of 5.6 days (range, 0–18) postoperatively. Five patients underwent anterior decompression with spinal fusion (C4–C6), three laminoplasty (C3–C7) with foraminotomy (C5/6: 2, C4/5 and C5/6: 1). One patient could get full recovery after 2 years. This patient was categorized in the excellent group. But seven patients with C5 palsy could not improve enough after >3 years postoperatively. These patients were categorized in the poor group.
Discussion
In general, CMAP amplitude reflects the number of alive axons. Erb-point-stimulated CMAP in the deltoid are useful to predict the natural history of proximal CSA [8]. Two authors (YI and MF) examined Erb-point stimulating CMAP for 28 patients with compressive cervical myelopathy and 88 able-bodied participants in our previous study [9]. There were few intraobserver variations. The reproducibility of these CMAP is sufficient [9,10,11]. Therefore, CMAP by repetitive Erb stimulation provide a simple, valid, and noninvasive supplementary test for distinguishing CSA from motor neuron diseases including ALS [10, 11]. Particularly, patients with CMAP exceeding 50% of the normal side showed the most complete return of function, despite severe weakness. Patients in whom the percentage amplitude of CMAP in the most severely atrophic muscle was >10% on the affected side than that on the normal side were able to recover muscle function [12]. We performed cervical surgery for patients with CMAP-R values of 10–50%. Of these patients, 16 patients resulted fair outcomes. Group F showed significant positive correlations with CMAP-R, CMAP-RD, CMAP-RB, DCH, and MMT-BA, and CMAP amplitude of the deltoid and biceps brachii on the affected side compared with Group EG (P < 0.05). This study used MLRA to determine factors related to Group F. We demonstrated that patients in Group F tended to have lower CMAP-R values (P = 0.0099; OR, 0.89). Tauchi et al. reported risks factors for a poor outcome following surgical treatment of CSA [13]. Symptom duration and preoperative MMT grade were associated with an increased risk of a poor surgical outcome based on MLRA. In addition, they recommended surgical intervention for patients with proximal CSA within about 4 months after the onset of symptoms if conservative treatment has not been successful [14]. By our univariate analyses, DCH and MMT-BA were significantly different between Group F and Group EG. Therefore, we agreed with their view. However, there were no electrophysiological findings in their data. In the MLRA including the electrophysiological findings, CMAP-R was the only significant preoperative factor related to a fair outcome after surgical treatment for patients with proximal CSA. Uchida et al. reported that the percent voltage of Erb-point or wrist-stimulated MEP correlated with surgical outcome [15]. Our results were consistent with their results.
It is difficult to determine whether surgery of the cervical spine should be recommended for patients with proximal CSA because some patients had fair or poor outcomes. Conversely, some patients had full recovery with conservative therapy. We determined a strategy for the treatment of proximal CSA patients using electrophysiological examination [3]. We should perform cervical surgery for patients with CMAP-R values of 10–30% and CMCT values of <6.8 ms and patients with CMAP-R values of 30–50% regardless of CMCT [3].
CMCT is used to electrophysiologically evaluate the corticospinal tract function and for diagnosing disorders of the corticospinal tract [16,17,18]. We reported the normative value of the CMCT to be 5.2 ± 0.8 ms (mean ± SD) for participants exerting a slight effort regardless of age and body height [18]. These measurements were considered to be abnormal when they exceeded the normal mean value by >2.0 standard deviations. We suggested that patients with CMCT values ≥6.8 ms have compressive cervical myelopathy and those with CMCT values <6.8 ms have only the ventral nerve root disorder. Therefore, we considered it necessary to perform surgery in patients with a CMCT value ≥6.8 ms to prevent the deterioration of myelopathy. Seventeen of twenty-four patients with excellent, one of three patients with good, seven of sixteen patients with fair, and four of six patients with poor outcomes had a value <6.8 ms in the current study. Many patients with excellent outcomes did not have myelopathy. We recommend cervical surgery for myelopathic patients to prevent the deterioration of myelopathy and nonmyelopathic patients to improve muscle strength.
Patients with poor outcomes
Eight patients (15%) had a C5 palsy. The mean reported incidence of C5 palsy following surgery for cervical compression myelopathy using the anterior approach is 4.3% (range, 1.6–12.1%) [19]. The incidence of C5 palsy for proximal CSA was very high compared with that for other diseases. Kaneko et al. reported the pathology of C5 palsy [20]. The C5 nerve root was innervated predominantly for the deltoid compared with those at other cervical intervertebral lesions, probably due to the segmental gray matter lesions of the C6 spinal cord in patients with cervical myelopathy at the C4–5 level. Weakness of the deltoid must be clinically apparent if postoperative C5 radiculopathy has occurred in patients whose C5 nerve root is innervated predominantly for deltoid muscles. We considered this pathology as a sure indication of proximal CSA. The outcome of patients with C5 palsy was not good, because they had severe C5 and /or C6 anterior horn and/or ventral root disorders preoperatively. Imagama et al. reported that 67% of patients with C5 palsy achieved complete recovery [21]. We therefore think there is an increased risk of persistent C5 palsy in patients with proximal CSA. CMAP-R, CMAP-RD, CMAP-RB, and CMAP amplitude of deltoid on the affected and normal sides, CMAP amplitude of biceps on the affected side, age, DCH, and high intensity area on T2-weighted MRI did not differ significantly between patients with excellent outcomes and those with poor outcomes. CMAP amplitude of biceps brachii on the normal side of patients with poor outcomes was significantly higher than that of patients with excellent outcomes (P < 0.05). Patients with poor outcomes should have achieved excellent outcomes as a result of the electrophysiological findings. We could not find differences between patients with excellent and poor outcomes in our data.
Limitations to our study should be kept in mind when interpreting the results. The sample size was relatively small. The study may have been underpowered to identify any significant difference regarding surgical outcomes. However, to the best of our knowledge this represents the first report to identify preoperative factors related to patients with fair outcomes using electrophysiological examinations and the current study had the largest patients with proximal-type CSA.
In conclusion, CMAP-R could be used as a reliable predictive factor related to a fair surgical outcome following surgery in patients with proximal CSA. The incidence of C5 palsy for proximal CSA was very high compared with that for other diseases. We must pay attention to the incidence of C5 palsy after surgery.
Data availability
The datasets generated and /or analyzed during the current study are available from the corresponding author on reasonable request.
References
Sobue I, Kato H, Yanagi T. Clinical characteristics and classification of cervical spondylotic amyotrophy. Rinsho Shinkeigaku. 1975;10:999–1006.
Jiang SD, Jiang LS, Dai LY. Cervical spondylotic amyotrophy. Eur Spine J. 2011;20:351–7.
Imajo Y, Kato Y, Kanchiku T, Suzuki H, Yoshida Y, Funaba M, et al. Prediction of surgical outcome for proximal-type cervical spondylotic amyotrophy novel mode of assessment using compound action potentials of deltoid and biceps brachii and central motor conduction time. Spine. 2012;37:E1444–E1449.
De Carvalho M, Dengler R, Eisen A, England JD, Kaji R, Kimura J, et al. Electrodiagnostic criteria for diagnosis of ALS. Clin Neurophysiol. 2008;119:497–503.
Barker AT, Jalinous R, Freeston IL, Jarratt JA. Clinical evaluation of conduction time measurements in central motor pathways using magnetic stimulation of the human brain. Lancet. 1986;7:1325–6.
Ranvnborg M, Blinkenberg M, Dahl K. Standardization of facilitation of compound muscle action potentials evoked by magnetic stimulation of the cortex. Results in healthy volunteers and in patients with multiple sclerosis. Electroencephalogr Clin Neurophysiol. 1991;81:195–201.
Kaneko K, Taguchi T, Morita H, Yonemura H, Fujimoto H, Kawai S. Mechanism of prolonged central motor conduction time in compressive cervical myelopathy. Clin Neurophysiol. 2001;112:1035–40.
Tani T, Kishimoto H, Tsuboya H, Kimura J. Electrophysiologic assessment of shoulder girdle weakness in patients with cervical spondylosis: prognostic value of supraclavicular stimulation. J Clin Neuromuscul Dis. 2002;4:11–18.
Funaba M, Kanchiku T, Imajo Y, Suzuki H, Yoshida Y, Taguchi T. Preoperative diagnosis of the responsible level in CCM using CMAPs: comparison with SCEPs. Spinal cord. 2014;52:191–6.
Iwanami T, Sonoo M, Hatanaka Y, Hokkoku K, Oishi C, Shimizu T. Decremental responses to repetitive nerve stimulation (RNS) in motor neuron disease. Clin Neurophysiol. 2011;122:2530–6.
Zheng C, Jin X, Zhu Y, Lu F, Jiang J, Xia X. Repetitive nerve stimulation as a diagnostic aid for distinguishing cervical spondylotic amyotrophy from amyotrophic lateral sclerosis. Eur Spine J. 2017;26:1929–36.
Fujiwara Y, Tanaka N, Fujimoto Y, Nakanishi K, Kamei N, Ochi M. Surgical outcome of posterior decompression for cervical spondylosis with unilateral upper extremity amyotrophy. Spine. 2006;31:E728–E732.
Tauchi R, Imagama S, Inoh H, Yukawa Y, Kanemura T, Sato K, et al. Risk factors for a poor outcome following surgical treatment of cervical spondylotic amyotrophy: a multicenter study. Eur Spine J. 2013;22:156–61.
Tauchi R, Imagama S, Inoh H, Yukawa Y, Kanemura T, Sato K, et al. Appropriate timing of surgical intervention for the proximal type of cervical spondylotic amyotrophy. Eur J Orthop Surg Traumatol. 2015;25(Suppl 1):S107–S113.
Uchida K, Nakajima H, Yayama T, Sato R, Kobayashi S, Kokubo Y, et al. Anterior and posterior decompressive surgery for progressive amyotrophy associated with cervical spondylosis: a retrospective study of 51 patients. J Neurosurg Spine. 2009;11:330–7.
Nakanishi K, Tanaka N, Sasaki H, Kamei N, Hamasaki T, Yamada K, et al. Assessment of central motor conduction time in the diagnosis of compressive thoracic myelopathy. Spine. 2010;35:E1593–E1598.
Claus D. Central motor conduction: method and normal results. Muscle Nerve. 1990;13:1125–32.
Imajo Y, Kanchiku T, Suzuki H, Yoshida Y, Funaba M, Nishida N, et al. Effects of differences in age and body height on normal values of central motor conduction time determined by F-waves. J Spinal Cord Med. 2017;40:181–7.
Sakaura H, Hosono N, Mukai Y, Ishii T, Yoshikawa H. C5 palsy after decompression surgery for cervical myelopathy. Spine. 2003;28:2447–51.
Kaneko K, Hashiguchi A, Kato Y, Kojima T, Imajo Y, Taguchi T. Investigation of motor dominant C5 paralysis after laminoplasty from the results of evoked spinal cord responses. J Spinal Disord Tech. 2006;19:358–61.
Imagama S, Matsuyama Y, Yukawa Y, Kawakami N, Kamiya M, Kanemura T, et al. C5 palsy after cervical laminoplasty: a multicenter study. J Bone Jt Surg. 2010;92:393–400.
Acknowledgements
The authors acknowledge Prof. Kiyoshi Ichihara, Department of Clinical Laboratory Sciences, Faculty of Health Sciences, Yamaguchi University Graduate School of Medicine, who performed all of the statistical analysis and supported paper preparation.
Author information
Authors and Affiliations
Contributions
YI was responsible for designing and conducting the search. NN, MF, HS, and TS were responsible for extracting and analyzing data, interpreting results.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
We certify that all applicable institutional regulations concerning the ethical use of human volunteers were followed during the course of this research.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Imajo, Y., Nishida, N., Funaba, M. et al. Preoperative factors that predict fair outcomes following surgery in patients with proximal cervical spondylotic amyotrophy. A retrospective study. Spinal Cord 58, 348–355 (2020). https://doi.org/10.1038/s41393-019-0365-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-019-0365-2
