Article Text

Abstract
Introduction Italian law mandates that every competitive athlete must undergo annual preparticipation evaluation (PPE) to identify cardiovascular (CV) diseases that pose a risk of sudden death (SD) during sport and other conditions that may threaten the athlete’s health. We investigated the diagnostic yield, rate of disqualification and costs of our PPE.
Methods We included 5910 consecutive apparently healthy athletes (61% males, mean age 15±4 years) who underwent annual PPE performed by a sports medicine specialist. The PPE included history, physical examination, weight, height and blood pressure measurement, test of visual acuity, spirometry, urine chemistry, resting 12-lead ECG and exercise testing with ECG monitoring. In cases of abnormal findings, we carried out second-line investigations.
Results During a 12-month study period, 5.326 (90.2%) athletes were cleared for competition after a normal first-line evaluation and 584 (9.8%) underwent one or more further examinations. Of those, 88 (1.5%) were diagnosed to have a CV disease (including 18 (0.3%) at-risk of SD) and 31 (0.5%) had a non-CV diagnosis. A total of 32 (0.5%) athletes were temporarily (n=15) or permanently (n=17) disqualified from competitive sports. The average cost per athlete was €79, which consisted of €64 (80%) for first-line evaluations and €15 (20%) for additional investigations.
Conclusion PPE according to the Italian model identified a range of diseases in 2.0% of apparently healthy athletes at an average cost of €79.
- athletes
- cost–benefit analysis
- preparticipation screening
- sports medicine
- sudden death
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What are the findings?
In Italy, 5910 athletes underwent preparticipation evaluation (PPE) and 10% were prescribed additional investigations. In 2% we identified a disease that was unknown to the athlete (such as ventricular arrhythmias and asthma); 0.3% of athletes screened were diagnosed with a condition that confers risk of sudden death (such as hypertrophic cardiomyopathy);
Only 0.5% of athletes were temporarily or permanently disqualified from competitive sports and the cost of PPE including first-line evaluation and additional investigations was less than €80 per athlete.
How might it impact on clinical practice in the future?
The value of PPE in asymptomatic athletes is debated. This paper provides data on the prevalence of diagnoses, disqualification rate and costs from the Italian setting.
Introduction
Since 1982, it has been mandatory for every Italian competitive athlete to undergo annual preparticipation evaluation (PPE)1 that includes the assessment of the cardiovascular (CV) system and non-CV investigations. In the Veneto region of Italy, there was a sharp decline (89%) in the incidence of sudden death (SD) of competitive athletes over the 21 years after annual screening legislation was enacted.2 These findings have led several organisations, including the European Society of Cardiology and the International Olympic Committee, to recommend implementation of CV screening of athletes.3 4 Many PPE programmes have been established worldwide,5–8 but whether competitive athletes should be systematically screened remains controversial. There is a school of thought that the costs of a nationwide PPE programme would be prohibitive and the benefits questionable given the low incidence of SD in the athletes, the potential for unnecessary disqualifications (false positives)9 10 and the fact that screening does not eliminate all cardiac deaths among young athletes.11 12
Although previous studies on the PPE have mainly focused on identifying CV diseases associated with SD,5–8 which is the most important goal of the PPE, additional benefits include early diagnosis of conditions that may pose a threat to the health of the athlete and require follow-up and treatment. Furthermore, identification of athletes with inherited diseases may prompt family screening. On the other hand, data on the percentage of disqualified athletes and costs are also needed to assess potential disadvantages. Despite the nationwide PPE programme being established in Italy more than 35 years ago, no previous study has reported its overall results and costs.
Therefore, we investigated the diagnostic yield, rates of disqualification and costs (per athlete and per diagnosis) of the PPE during 1 year of activity at a large sports medicine centre of the Italian National Health System.
Methods
The study included all consecutive competitive athletes undergoing annual PPE in 2017 at the Center for Sports Medicine of Treviso, ULSS2 Marca Trevigiana, Italian National Health System. The age at which competitive activity starts ranges from 8 to 17 years according to the sports disciplines and is established by each sport federation. The analysis included all conditions diagnosed during the PPE and requiring treatment or follow-up, regardless of the competitive sport eligibility decision. Diseases known to the athlete before the PPE were not included in the analysis. Only second-line investigations needed to reach a diagnosis were considered, but not those that were prescribed after the diagnosis (for risk stratification and management) or for a condition that was already known.
Protocol of PPE
The PPE protocol for competitive non-professional athletes is established by the Italian law1 and regional regulations. It is carried out by a physician with a specialty degree in sports medicine obtained after 4 years of full-time training and in-depth instruction in ECG interpretation. The first-line evaluation included history, physical examination, visual acuity test with Snellen chart, resting 12-lead ECG, ECG stress testing, spirometry and urine dipstick. History focused on family background, lifestyle (ie, training level, smoking …), previous medical history and cardiac symptoms (chest pain, shortness of breath, palpitations, syncope). Physical examination included cardiac, pulmonary and abdominal examination, bend test to check for scoliosis, weight, height and blood pressure measurement. In athletes >40 years, the CV risk was calculated with the Systematic COronary Risk Evaluation (SCORE) risk charts.13 Resting 12-lead ECG was acquired before stress testing, with the athlete supine at standard speed (25 mm) and gain (0.1 mV/mm) and interpreted according to the international recommendation for ECG interpretation in athletes.14 According to the law, the protocol of stress testing was age-dependent and justified by the different prevalence of at-risk CV diseases, namely inherited arrhythmogenic disorders in young athletes and coronary artery disease in masters athletes. Young competitive athletes <35 years underwent a bicycle stress test with a constant load, that is, 2 or 3 W/kg (depending on gender) increase per 3 min or until >85% of the maximal heart rate was achieved, plus 3 min of postexercise monitoring, with the main aim of assessing for ventricular arrhythmias. Masters athletes aged ≥35 years underwent a standard maximal exercise test with an incremental protocol, that is, 50 W increment increase every 2 min until exhaustion, plus 6 min of recovery, with attention to exercise-induced myocardial ischaemia or arrhythmias. Spirometry measured flow and volume changes during forced breathing manoeuvres. Particular attention was given to flow volume curve and to measurements of forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1) and FEV1/FVC ratio. Urine dipstick is a basic diagnostic tool that allows to analyse the presence of proteins, glucose, ketones, haemoglobin, bilirubin, urobilinogen, acetone, nitrite and leucocytes using a test strip immersed in a urine sample.
Further examinations and eligibility
Further examinations were conducted for abnormal findings at first-line evaluation. In particular, when a CV disease was suspected, second-line investigations included ECG monitoring of 24-hour with a training session and echocardiography. Third-line examinations such as cardiac magnetic resonance or coronary angiography/computed tomography were reserved for selected cases. At the end of the diagnostic work-up, all cases were discussed by a multidisciplinary team including a cardiologist to determine management and eligibility.
Athletes who received a new diagnosis were treated as appropriate by the sports physician or referred to a specialist. Management of CV diseases including eligibility to competitive sports followed the recommendations of the Italian Society of Sports Cardiology.15 If the condition was deemed incompatible with safe competitive sports participation, the athlete was disqualified, either temporarily (if a curative treatment was available) or permanently. According to the law, the decision is binding but the athlete has the right to appeal to a regional multidisciplinary commission. All disqualified subjects were given a clinical report which included tailored advice on leisure time exercise activities with details on type (including both aerobic and strength exercises), intensity (range of heart rate based on cardiopulmonary test or heart rate reserve), duration and frequency and were offered to enrol in a follow-up programme. Moreover, in case of diagnosis of a genetically determined cardiomyopathy, first-degree family members were offered CV evaluation.
Costs in the Veneto region
In the Veneto region (northeastern Italy), the cost for each PPE in public medical centres at the time of the study was €62 for athletes <35 years and €102 for athletes ≥35 years. Costs for second-line investigations were calculated according to the rate tables of the Veneto region for medical investigations and procedures within the National Health System. PPE is provided for free by the National Health System (funded with taxes) for athletes under 18 years and Paralympic athletes, while older athletes have to pay full fares. The cost of second-line investigations is co-paid by the athlete and the National Health System. The part paid by the athlete depends on his/her family income (free for athletes belonging to a family with an annual income up to €12 000, a maximum of €41.15 for family income up to €29 000 and a maximum of €46.15 in the other cases).
Statistical analysis
Data are expressed as n (%) or mean (±SD). The difference in the rates of second-line investigations, diagnosis and disqualifications among age groups was evaluated with the χ2 test. A p-value <0.05 was considered significant. Data were analysed with SPSS V.23 (IBM). Anonymised study data were collected and managed using REDCap electronic data capture tools (https://www.project-redcap.org) hosted at University of Padova.
Results
During the 12-month study period, 5910 athletes (3627 males, 61%; mean age 15±4 years) were evaluated at our centre: 1911 for the first time and 3999 for renewal of the certificate of eligibility. Of those, 1037 (18%) were children aged 7–11 years, 4424 (75%) teenagers aged 12–18 years, 235 (4%) young athletes aged 19–34 years and 214 (4%) senior athletes aged 35–58 years. This distribution reflects the fact that the evaluation is free for athletes under 18 years. The vast majority (97%) of athletes were of Caucasian ethnicity.
Screening and second-line investigations
During a 12-month study period, 5.326 (90.2%) athletes were cleared for competitive sports activity after a normal first-line evaluation. Second-line investigations were prescribed to 584 (9.8%) athletes because of abnormalities at first-line examination (figure 1 and table 1).

Summary of main study findings.
Number and costs of first-line evaluations and second-line investigations prescribed to confirm or exclude the suspicion of a disease
Diseases detected
Overall, 88 athletes (1.5%) received a new CV diagnosis (table 2) including 18 (0.3%) cases of CV diseases at risk of SD (table 3). Cascade family screening of 21 relatives of athletes with genetically determined heart diseases led to the identification of three affected parents (with long QT syndrome, arrhythmogenic cardiomyopathy and left ventricular non-compaction) who were unaware of their disease. The remaining 70 athletes were found to be affected with other CV diseases that are not traditionally associated with SD but that require follow-up or treatment. Finally, 31 (0.5%) athletes received a non-CV diagnosis.
List of cardiovascular diseases and non-cardiovascular conditions identified for the first time during preparticipation evaluation
Characteristics of athletes diagnosed with a cardiovascular disease at risk of sudden death
Treatment and sports eligibility
Among the 18 athletes with CV diseases at risk of SD, the patient with ventricular pre-excitation was referred for catheter ablation; the patient with Brugada syndrome was referred for eletrophysiological study; the two athletes with major coronary anomalies were evaluated for possible surgical correction; the patient with obstructive coronary artery disease underwent percutaneous myocardial revascularisation; and the patient with bicuspid aortic valve complicated by aortic dilation was prescribed strict follow-up. The other 13 patients were prescribed drug therapy according to current guidelines and offered an individualised non-competitive exercise programme.
Among the 70 athletes with other CV diseases, all patients with congenital heart diseases were temporarily disqualified and recommended percutaneous or surgical correction. In four of five athletes, the congenital defect was corrected and, after 3 months without complications, they were allowed to resume competitive sports activity. Lifestyle and drug therapy were prescribed to patients with hypertension, dyslipidaemia and diabetes: in severe cases, eligibility for competitive sports activity was suspended until the treatment proved to be effective. The other athletes were only recommended follow-up.
Among the 31 athletes with non-CV disease, 29 required treatment such as bronchodilators (n=15), glasses prescription (n=9), orthopaedic bracing (n=3), orthopaedic surgery (n=1) and therapy with ACE inhibitors (n=1).
Overall, 17 (0.3%) athletes were permanently disqualified (including 15 with at-risk CV diseases and 2 with hypertension with organ damage) and 15 (0.3%) athletes were temporarily disqualified from competitive sports activity.
Costs
The costs of first-line evaluation and second-line investigations that were prescribed are detailed in table 1. The overall cost of the PPE was €466 660 including €407 490 (87%) paid by the National Health System (funded with taxes) and €59 170 (16.7%) paid by the athletes. The cost for each athletes was €79 (including €63 (80%) for first-line evaluation and €16 (20%) for additional investigations) or €5290 for each disease diagnosis (including €4250 for first-line evaluation and €1040 for additional investigations) or €25 870 for each diagnosis of a CV disease at risk of SD (including €20 790 for first-line evaluation and €5080 for additional investigations).
Age groups
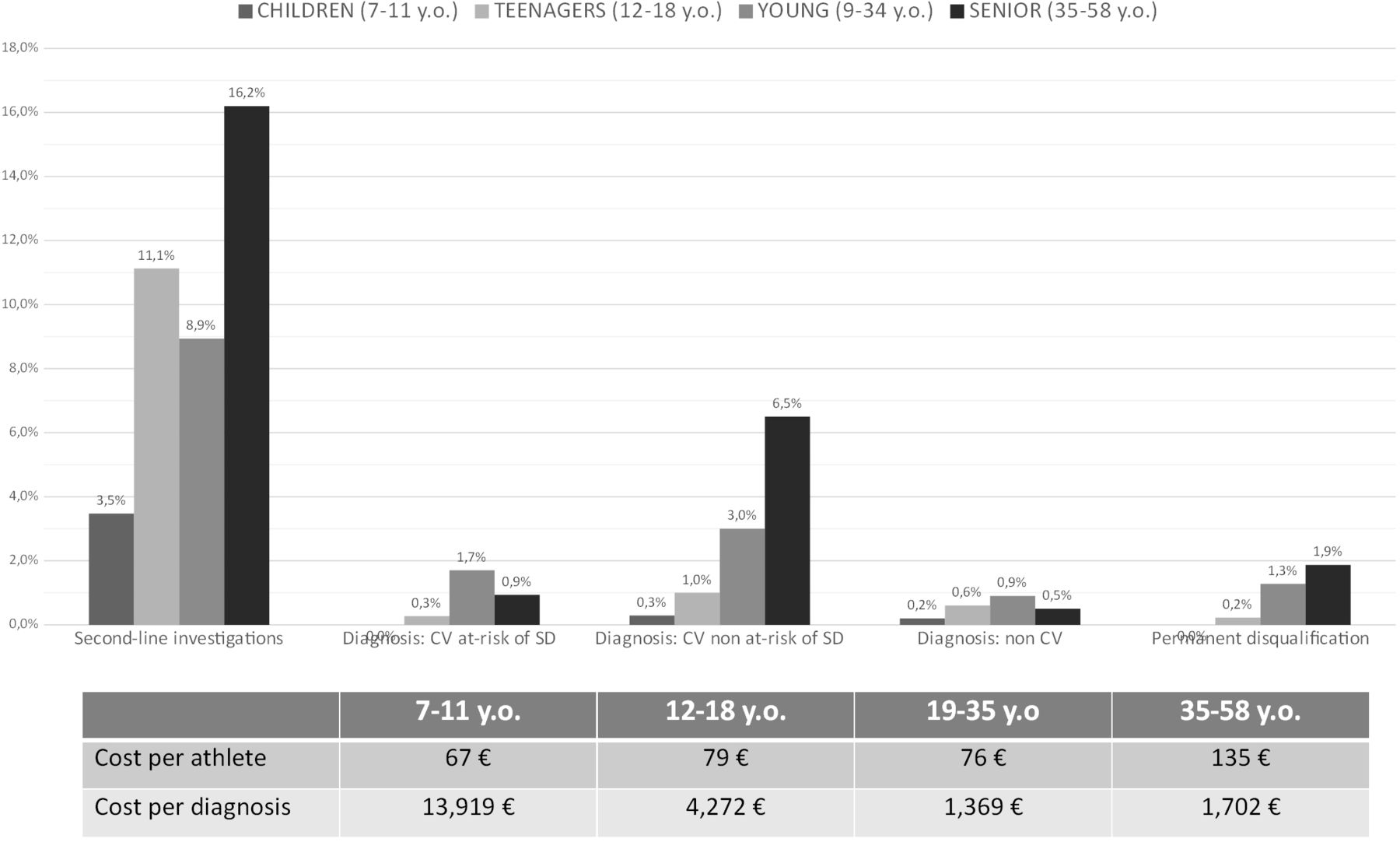
Figure 2 shows the rates of second-line investigations, new diagnosis, permanent disqualification and costs according to age group. There was a statistically significant higher number of total diagnoses with increasing age (0.5% among children aged 7–11 years, 1.9% among teenagers aged 12–18 years, 5.5% among young athletes aged 19–35 years and 7.9% among senior athletes aged 35–58 years, p<0.001). The cost per athlete was highest in the senior athletes group (€135) as a result of the higher cost of first-line evaluation (€102 vs €62 in younger athletes), whereas children showed the highest cost per diagnosis (€13 920) because of the low disease prevalence in this age group.

{kind=link}
{kind=link}
Rates of prescription of second-line investigations prescription, disease diagnosis, permanent disqualification and costs according to age group.
Discussion
We evaluated the results of a PPE protocol applied to almost 6000 athletes over a 1 year study period that aimed to rule out potential CV and non-CV conditions that may preclude safe participation in competitive sports activity. The main results were the following: (1) 119 (2.0%) athletes received a new disease diagnosis, including 18 (0.3%) cardiac diseases at risk of SD during sports; (2) 32 (0.5%) athletes were temporarily or permanently disqualified from competitive sports activity and (3) the cost of the entire screening programme was €79 per athlete.
Benefits of PPE for the athlete
The ethics, feasibility, economic sustainability and best protocol of an athlete’s PPE is debated.16–18 Previous studies mainly focused on SD prevention and reported that PPE allowed to identify a CV disease at-risk of malignant ventricular arrhythmias in 0.25%–0.5% of screened athletes, a figure that is consistent with the 0.3% of the present investigation.5–8 Although the most important aim of medical evaluation of athletes is to prevent SD, we argue that there are also other benefits too as the Italian protocol of PPE is multidisciplinary—it is not limited to excluding CV diseases alone.
In our centre, PPE allowed us to identify 70 CV diseases not considered to be at risk of SD but that require treatment or follow-up, and 31 relevant non-CV conditions such as asthma, visual impairment or scoliosis. Note that as we followed up with family screening of athletes with genetically determined heart diseases, we identified three affected relatives who were unaware of the disease.
Implications for sports eligibility
There is concern that the PPE may lead to a high number of unnecessary disqualifications as a result of false positive findings or overestimation of the risk associated with certain diseases.19 20 Restricting or prohibiting competitive sport may have psychological and physical consequences that may theoretically outweigh the potential risk.21
In the past 20 years, the Italian Sports Cardiology Association has refined the screening protocols and eligibility criteria. In particular, early recommendations on CV assessment of the athlete were more conservative (ie, included more false positives), while the latest version (2017, available at http://www.sicsport.com/pubblicazioni/cocis-protocolli-cardiologici-idoneita-sportiva) took into consideration more recent scientific evidence and limited the cases where athletes were advised against playing sport.15 22 23 For example, compared with previous recommendations, competitive sports activity is no longer contraindicated in case of frequent ventricular arrhythmias with no underlying structural heart disease or asymptomatic Brugada syndrome and in selected pacemaker or implantable cardioverter defibrillator carriers. The recommended time of temporary disqualification after catheter ablation of arrhythmias or surgical correction of congenital defects has been shortened to 1–6 months. In the present study, only 0.5% of screened individuals were disqualified (either temporarily or definitively) from competitive sports activity. These young individuals were not deprived of the many benefits (physical and psychological) offered by physical activity but were offered a tailored moderate-intensity exercise prescription programme developed in the Veneto region.
Costs
Economic cost of the PPE has been cited as a barrier to implementing screening programme similar to ours in other countries.24 The cost including second-line investigations in our study performed in Italy was essentially €80 per athlete. This compares with the $87 (€76) per athlete needed to evaluate an athlete in the United Kingdom with history, physical examination and resting ECG only, and the $97.5 (€85) needed to perform the same protocol in Canada.5 6 In Qatar, the cost per athlete of PPE for CV diseases with baseline ECG and additional investigations in case of abnormal findings was $265 (€230) per athlete.25
The relatively low cost of PPE in Italy is mainly the result of the fact that first-line evaluation is carried out entirely by a single physician with a specialist degree in sport and exercise medicine. This specialty training requires 4 years of full-time training after the basic medical (MD equivalent) degree. Because of the multidisciplinary skills of sports medicine specialists, the same physician carries out different investigations on several body systems (such as spirometry, resting ECG and stress testing). Because of continuous refinements in interpretation of PPE findings,14 26 only 9.8% of athletes were prescribed second-line investigations. Second-line costs accounted for 20% of the overall screening costs. It is of note that the 9.8% rate of athletes undergoing further examinations is similar to the 7.4% reported by a recent study which focused only on the CV system and already included echocardiography among first-line examinations.11
The cost of each diagnosis was on average ≈€4000 (or ≈€25 000 considering only the diagnosis of diseases at risk of SD). An early diagnosis of a CV disorder in a young individual has a potentially high impact on life expectancy, especially because diseases such as coronary artery anomalies or cardiomyopathies can lead to SD if left untreated but are associated with a very good prognosis if appropriately managed. The early diagnosis of other diseases such as simple congenital heart disease, hypertension, dyslipidaemia, asthma or scoliosis may not reduce the risk of SD during sports activity but may also impact on the health of a young individual.
Because of the lower disease prevalence, the cost per diagnosis was more than three times higher among children (7–11 years) than among adolescents (12–18 years). This finding, together with the very low risk of SD before puberty,27 28 raises the question whether PPE at such a young age should be performed.
Study limitations
Results of this study may not apply to other countries with different health systems, costs or PPE protocols. By law, athletes have the right to undergo PPE with the same protocol in private centres, where diagnostic yield and costs (entirely paid by the athlete) may be different. Moreover, the study sample mostly comprised Caucasian adolescent athletes, while other ethnicities were poorly represented. Athletes were examined by different sports physicians, and no interobserver variability analysis was performed. We could not compare the prognosis of athletes with CV diseases who did and did not continue competitive sports activity because the Italian law mandates disqualification of athletes with at-risk conditions: therefore, a cost–benefit analysis could not be performed. Finally, as the study focused only on new diagnoses made at the time of PPE and conditions that were already known to the athlete were not considered, our study does not illuminate disease prevalence in the athletic population.
Conclusions
We underscore that the Italian PPE model is comprehensive—it is not limited to only CV screening for conditions associated with risk of SD. We identified and managed a variety of diseases, both CV and non-CV, in 2% of apparently healthy athletes at a cost of around €80 per athlete.
References
Footnotes
TV and AZ are joint first authors.
TV and AZ contributed equally.
Contributors All authors have significantly contributed in at least two of the following points: study design, data collection, data analysis, manuscript drafting and critical revision of the manuscript.
Funding This research received fundings from the preventive healthcare directorate of the Veneto region of Italy (Direzione Prevenzione, sicurezza alimentare e veterinaria, Regione Veneto, Rio Novo - Dorsoduro 3493, Venezia, Italy)
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Ethical committee of the Treviso province (No 643). Consent form was not required as data are completely anonymised.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.