
Abstract
It has been recently established that laser treatment can be combined with topical or intralesional medications to enhance the delivery of drugs and improve overall results in a variety of different dermatological disorders. The aim of this review is to evaluate the use of laser and energy-assisted drug delivery (LEADD) for the treatment of alopecia with a specific focus on ablative fractional lasers (AFL), non-ablative fractional lasers (NAFL), and radiofrequency microneedling (RFMN). A comprehensive PubMed search was performed in December 2022 for “laser-assisted drug delivery” as well as “laser” and “alopecia.” The evidence regarding LEADD for alopecia treatment is limited to two specific alopecia subtypes: alopecia areata (AA) and androgenetic alopecia (AGA)/pattern hair loss (PHL). LEADD with minoxidil and platelet-rich plasma (PRP) were evaluated for efficacy in both treatments of AA and AGA. LEADD with topical corticosteroids and intralesional methotrexate were studied for the treatment of AA, while LEADD with growth factors and stem cells were studied for the treatment of AGA. Multiple RCTs evaluated LEADD for topical corticosteroids with ablative fractional lasers for the treatment of AA. There is evidence in the literature that supports the use of topical minoxidil in combination with all devices for the treatment of AGA/PHL. All the reviewed studies show a positive treatment effect with LADD; however, some trials did not find LEADD to be superior to monotherapy or microneedling-assisted drug delivery. LEADD is a rapidly emerging treatment modality for the treatment of AGA and AA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
It has been recently established that laser treatment can be combined with topical or intralesional medications to enhance the delivery of drugs and improve overall results in a variety of different dermatological disorders [1]. This treatment is often referred to as laser-assisted drug delivery (LADD). However, there are other devices that can be used to enhance drug delivery like radiofrequency microneedling (RFMN). We propose a new term—laser and energy-assisted drug delivery (LEADD)—to include other forms of energy-based devices not included in LADD.
There are many types of alopecia with different treatment algorithms, but most rely on topical medications to the scalp. These topical medications such as topical minoxidil and triamcinolone acetonide (TAC) have been used with laser and energy-based devices for LEADD treatment for alopecia. The aim of this review is to evaluate the use of LEADD for the treatment of alopecia with a specific focus on ablative fractional lasers (AFL), non-ablative lasers (NAFL), and RFMN.
Methods
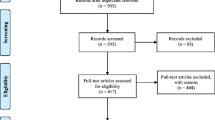
A comprehensive PubMed search was performed in December 2022 for “laser-assisted drug delivery” as well as “laser” and “alopecia.” Articles were then screened for eligibility with the inclusion criteria as the article focused on LEADD for alopecia treatment, focused on human subjects, and was in English. The results were further refined to only include articles involving AFLs, NAFLs, and RFMN. Review articles were excluded. Ultimately, 18 articles were included in this review spanning from 2018 to 2022. Articles were evaluated for laser type and setting, drug, study design, selected outcomes, and study type. Randomized controlled trials (RCTs) were assessed for quality by the Jadad scale which is a five-point scale that addresses randomization (2 points), blinding (2 points), and accounting for all subjects including dropouts (1 point) [2].
Results
Currently, the evidence regarding LEADD for alopecia treatment is limited to two specific alopecia subtypes: alopecia areata (AA) and androgenetic alopecia (AGA)/pattern hair loss (PHL) (Table 1).
Minoxidil
Minoxidil is a mainstay topical therapy for AGA. Several studies investigated the efficacy of topical minoxidil as a LEADD treatment. A split-scalp RCT examined monthly RFMN with twice daily topical 5% minoxidil vs. topical minoxidil only for PHL. The study found a significant increase in hair count (p < 0.01) and hair thickness (p = 0.02) in the LEADD side after 5 months [6]. Another split-scalp RCT examined LEAAD using bimonthly NAFL laser with twice daily topical 5% minoxidil vs. topical minoxidil alone for AGA. This study found increased hair density and hair diameter in the LEADD group compared to monotherapy (p = 0.001) [5]. An open-labeled non-randomized clinical study examined the use of AFL (CO2) for AGA with a laser only group receiving treatment every 2 weeks, a twice daily topical minoxidil group, and a combination group receiving the topical and laser treatments. After treatment, hair thickness increased significantly only in the LEADD (p = 0.001) and the laser only group (p = 0.001), while hair count increased significantly in all groups: LEADD group (p = 0.001), laser group (p = 0.005), and minoxidil group (p = 0.007) [4]. All groups saw significant improvement in the LEADD group; however, different laser and energy devices were used, making it difficult to draw larger conclusions on the best device type for LEADD with topical minoxidil for AGA/PHL.
While topical minoxidil is not traditionally used for the treatment of AA, one case series examined the use of LEADD with bimonthly NAFL and twice daily topical minoxidil 5% for 8 patients. Hair regrowth of greater than 50% of lesions was seen in five patients with one patient seeing no hair regrowth [3].
Platelet rich plasma
A RCT with three groups—LEADD with monthly NAFL, followed by intralesional PRP, monthly NADL only, and intralesional PRP only—found no significant differences between groups with some improvements in 80% of LEADD group, 65% of laser group, and 70% of PRP group [7]. A pilot study examining LEADD with AFL (CO2), followed by intralesional PRP for AGA tested low vs. high pulse settings with the high pulse group showing significantly increased mean total hair density compared to low pulse group (p = 0.023) [9]. A retrospective study of patients treated with NAFL (Er:YAG) monotherapy or in combination with PRP at every other session. This study did not find a significant difference between groups, and all showed improvement; however, most patients were also on topical minoxidil and oral cosmeceuticals [8]. LEADD with PRP for AGA is an emerging therapy with currently limited evidence on whether it is superior to monotherapy.
Topical corticosteroids
Topical and intralesional corticosteroids are used to treat AA but can be combined with laser or energy devices for combination therapy. A RCT assigned patients to monthly microneedling or AFL (CO2), both followed by application of triamcinolone acetonide (TAC) for six sessions or resolution of lesions. Both groups had a statistically significant reduction in severity of alopecia Tool (SALT) score (p < 0.001) with a significant difference between groups favoring the microneedling group (p = 0.013) [14]. Another comparative study for treatment resistant AA compared microneedling or AFL (CO2), both followed by application of triamcinolone acetonide (TAC). Both groups had significant improvement at each follow-up with the only significant difference between groups being the presence of black dot dermoscopy sign which was more present in the laser group (46.7 vs. 13.3%) [13]. Two small case series of LEADD with TAC for AA using AFL (CO2), and RFMN saw positive results [11, 12].
One RCT directly compared microneedling-assisted drug delivery and LEADD using PRP and TAC. The sixty-person study randomized participants to four groups: AFL (CO2) and TAC, microneedling and TAC, AFL (CO2) and PRP, and microneedling and PRP. Each group had treatments every 3 weeks for four treatments. All treatment groups showed improvement; however, regrowth scales showed microneedling to be more effective than laser for drug delivery (p = 0.023) with TAC working better than PRP (p = 0.015) [10]. LEADD with TAC is an effective treatment for AA, but it may not be superior to microneedling-assisted drug delivery.
Other topical corticosteroids have been used for LEADD in AA. A trial comparing AFL (Er:YAG) followed by clobetasol and topical clobetasol alone found significant improvement in SALT score in both groups with the combination therapy showing a greater effect [15]. Another study using betamethasone compared LEADD using AFL (CO2) with betamethasone, AFL (CO2) alone, and betamethasone alone. All groups showed statistically significant decrease in SALT score after treatment (all p = 0.005) with LEADD group and laser group reducing SALT compared to topical group (LEADD: p = 0.003; laser p = 0.002) [16].
Other topicals: growth factors and methotrexate
A split-scalp RCT for AGA had one half of the scalp treated with AFL (CO2) with growth factors (GFs) applied to the full scalp every 2 weeks for 6 weeks. Mean hair density was significantly increased in both groups (p < 0.001) with a significant difference between groups favoring the LEADD group (p = 0.003) [18]. A similar split-scalp study for PHL performed weekly full-scalp NAFL (Thulium), followed by application of GFs to one half of the scalp. Both groups showed significantly increased hair counts (LEADD p = 0.001; laser p < 0.001) at 1 month post-final treatment session [19].
A split-scalp study for AGA investigated adipocyte-derived mesenchymal stem cell-conditioned media (ADSC-CM). The full scalp was treated with NAFL (Er:Glass) once followed by ADSC-CM to one half and placebo solution to the other. This study provided with an at-home microneedling device that participants used to the full scalp once a week along with weekly topical treatment application. The ADSC-CM group had significantly higher final densities compared to placebo (p < 0.05) [20]. The at-home microneedling device likely contributed more than the sole laser session in this study.
A case series of two patients with AA found a good response after treatment with AFL (CO2) and intralesional methotrexate (MTX). The first case saw regrowth of white hairs at 16 weeks after sessions of AFL followed by MTX every 2 weeks along with a pulse treatment of dexamethasone. The second case after failed therapy received AFL followed by MTX every 20 days along with 3-day prednisone treatment with complete response by week 22 [17]. While this case report provides limited evidence to the efficacy of AFL with MTX, it explores a new treatment option for patients who have failed intralesional and systemic corticosteroids.
Discussion
LEADD for alopecia is an emerging field as 50% of the studies reviewed were published in 2022 reflecting a rapidly growing interest in treating alopecia with LEADD techniques. These studies only focus on treatment for AGA and AA with room for expansion into other types of alopecias in the future. All the studies noted in this review saw a positive treatment effect for the LEADD groups. The strongest evidence for LEADD in alopecia is for the use of AFL with topical corticosteroids. Minoxidil was combined with all devices, AFL, NAFL, and RFNM for a positive effect. The results were mixed on whether LEADD is superior to monotherapy or microneedling. Two of the RCTs for AGA comparing LEADD to microneedling-assisted drug delivery found the microneedling to be the superior treatment modality [10, 14]. Larger studies with different drugs are needed to directly compare treatment methods, various settings and depths of devices for treatment of the scalp.
Many articles compared the LEADD treatment to topical therapy only; however, three articles directly compared LEADD to device alone. All three studies did not find any difference between LEADD treatment and laser only. These studies investigated AFL and topical minoxidil 5% for AGA, NAFL, and injected PRP for AGA, and AFL and betamethasone for AA [4, 7, 16]. This may indicate that laser monotherapy may be an effective treatment for hair growth, as all studies showed improvement in alopecia.
It is important to note that the topical minoxidil studies may not be a true LEADD effect, as most studies had the participants continue to apply the minoxidil twice daily for the duration of the study. LADD works through fractional photothermolysis via a variety of mechanisms including dermal remodeling [21]. When using AFLs, channels are created within the skin to drive the drug delivery deeper; however, these channels close as reepithelization occurs which occurs up to 48 h after the AFL treatment [22, 23]. In these studies, the LEADD that occurs immediately post-treatment is synergistic with the daily application of the topical drug. This is relevant to clinical practice as patients with AGA participating in LEADD treatments should continue their topical regimens to achieve maximal results.
The LEADD was relatively well-tolerated in all studies with most studies reporting transient side effects related to laser procedures most commonly pain and erythema.
There is a lack of large, high-quality RCTs relating to LEADD treatment of alopecia which is evident by the low Jadad scores ascribed to most of the RCTs evaluated. It is difficult to conduct double-blinded studies, as it would be challenging to use a sham laser device. Only one of the articles utilized a topical placebo.
Conclusion
LEADD is a rapidly emerging treatment modality for the treatment of AGA and AA. Traditional drug modalities can be combined with laser treatments for an augmented effect. Larger, well-designed studies are needed to draw more definitive conclusions.
References
Alegre-Sánchez A, Jiménez-Gómez N, Boixeda P (2018) Laser-assisted drug delivery. Actas Dermosifiliogr (Engl Ed) 109(10):858–867
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ et al (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 17(1):1–12
Wang W, Gegentana G, Tonglaga T, Bagenna B, Li Y (2019) Treatment of alopecia areata with nonablative fractional laser combined with topical minoxidil. J Cosmet Dermatol. 18(4):1009–1013
Salah M, Samy N, Fawzy MM, Farrag AR, Shehata H, Hany A (2020) The effect of the fractional carbon dioxide laser on improving minoxidil delivery for the treatment of androgenetic alopecia. J Lasers Med Sci 11(1):29–36
Suchonwanit P, Rojhirunsakool S, Khunkhet S (2019) A randomized, investigator-blinded, controlled, split-scalp study of the efficacy and safety of a 1550-nm fractional erbium-glass laser, used in combination with topical 5% minoxidil versus 5% minoxidil alone, for the treatment of androgenetic alopecia. Lasers Med Sci 34(9):1857–1864
Yu AJ, Luo YJ, Xu XG, Bao LL, Tian T, Li ZX et al (2018) A pilot split-scalp study of combined fractional radiofrequency microneedling and 5% topical minoxidil in treating male pattern hair loss. Clin Exp Dermatol 43(7):775–781
Haddad N, Arruda S, Sadick N (2022) Evaluating the efficacy of platelet rich plasma and 1550 nm fractional laser in combination and alone for the management of androgenetic alopecia. J Drugs Dermatol 21(11):1166–1169
Day D, McCarthy M, Talaber I (2022) Non-ablative Er:YAG laser is an effective tool in the treatment arsenal of androgenetic alopecia. J Cosmet Dermatol 21(5):2056–2063
Hanthavichai S, Archavarungson N, Wongsuk T (2022) A study to assess the efficacy of fractional carbon dioxide laser with topical platelet-rich plasma in the treatment of androgenetic alopecia. Lasers Med Sci 37(4):2279–2286
El Mulla KF, Elmorsy EH, Halwag DI, Hassan EM (2022) Transepidermal delivery of triamcinolone acetonide or platelet rich plasma using either fractional carbon dioxide laser or micro-needling in treatment of alopecia areata. Dermatol Pract Concept 12(4):e2022196
Issa MCA, Pires M, Silveira P, Xavier de Brito E, Sasajima C (2015) Transepidermal drug delivery: a new treatment option for areata alopecia? J Cosmet Laser Ther. 17(1):37–40
Majid I, Jeelani S, Imran S (2018) Fractional carbon dioxide laser in combination with topical corticosteroid application in resistant alopecia areata: a case series. J Cutan Aesthet Surg 11(4):217–221
Omar MM, Obaid ZM, Sayedahmed OME (2022) Comparative study between topical application of triamcinolone acetonide after fractional carbon dioxide laser versus microneedling in the treatment of resistant alopecia areata. Dermatol Ther 35(12):e15913
Abd ElKawy FAE, Aly SHM, Ibrahim SMA (2022) Fractional CO2 laser versus microneedling as a transepidermal drug delivery system for the treatment of alopecia areata: a clinical dermoscopic evaluation. Dermatol Ther 35(7):e15553
Shokeir HA, Yousry A, Ibrahim SMA (2022) Comparative study between topical steroid alone versus combined fractional Erbium:YAG laser with topical steroid in treatment of alopecia areata. Arch Dermatol Res 315(2):241–247. https://doi.org/10.1007/s00403-022-02417-0
Halim DA, Nayer M, El-Samanoudy SI, Raheem HMA, Ragab N (2022) Evaluation of fractional carbon dioxide laser alone versus its combination with betamethasone valerate in treatment of alopecia areata, a clinical and dermoscopic study. Arch Dermatol Res 315(3):505–511. https://doi.org/10.1007/s00403-022-02393-5
Rodríguez-Villa Lario A, Aguado-García Á, Andrés-Lencina JJ, Corredera C, García-Legaz Martínez M, Alonso de Celada RM et al (2022) Successful response to a combination of intralesional methotrexate and fractional CO2 laser in refractory alopecia areata: case report. Skin Appendage Disord. 8(6):486–91
Huang Y, Zhuo F, Li L (2017) Enhancing hair growth in male androgenetic alopecia by a combination of fractional CO2 laser therapy and hair growth factors. Lasers Med Sci 32(8):1711–1718
Cho SB, Goo BL, Zheng Z, Yoo KH, Kang JS, Kim H (2018) Therapeutic efficacy and safety of a 1927-nm fractionated thulium laser on pattern hair loss: an evaluator-blinded, split-scalp study. Lasers Med Sci 33(4):851–859
Lee YI, Kim J, Kim J, Park S, Lee JH (2020) The effect of conditioned media from human adipocyte-derived mesenchymal stem cells on androgenetic alopecia after nonablative fractional laser treatment. Dermatol Surg 46(12):1698–1704
Zaleski-Larsen LA, Fabi SG (2016) Laser-assisted drug delivery. Dermatol Surg 42(8):919–931
Wenande E, Anderson RR, Haedersdal M (2020) Fundamentals of fractional laser-assisted drug delivery: an in-depth guide to experimental methodology and data interpretation. Adv Drug Deliv Rev 1(153):169–184
DeBruler DM, Blackstone BN, Baumann ME, McFarland KL, Wulff BC, Wilgus TA et al (2017) Inflammatory responses, matrix remodeling, and re-epithelialization after fractional CO2 laser treatment of scars. Lasers Surg Med 49(7):675–685
Author information
Authors and Affiliations
Contributions
E. B. and K. K. conceptualized the study. E. B., A. M., and Y. K. performed the research. E. B. wrote the paper. A. M., Y. K, J. C., and K. K. performed essential edits. J. C. and K. K. supervised the research.
Corresponding author
Ethics declarations
Informed consent
Not applicable.
Competing interests
Related to the subject of this manuscript, in the past 2 years, Dr Cohen has done clinical research and/or consulting for Sciton and Acclaro (laser) (Palo Alto, CA), InMode (RF) (Irvine, CA), and Eclipse/ Crown (microneedling) (The Colony, TX). The other authors have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Balazic, E., Muskat, A., Kost, Y. et al. The role of laser and energy-assisted drug delivery in the treatment of alopecia. Lasers Med Sci 39, 73 (2024). https://doi.org/10.1007/s10103-024-04015-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10103-024-04015-0