
Abstract
The present study examined the effectiveness of a personalized remote video feedback parenting program to improve mother-child interactions and child behavior outcomes among mothers of children with behavior problems in comparison to counterparts with no behavior problems. The sample comprised 60 mothers and their 2-to-6-year-old children, including children with behavior problems (BP = 19) and children without behavior problems (NoBP = 41). The Strengthening Bonds program included one in-person group session and remote personalized video feedback about their mother-child interactions in a play situation via smartphone for six weeks. Mother-child interactions were the primary outcome, and children’s behaviors were the secondary outcome. Pre- and post-intervention assessments were performed. The mother-child interactions were recorded during free- and structured-play situations and were then analyzed by the Parenting Interactions with Children: Checklist of Observations Linked to Outcomes (PICCOLO) and the Dynamics of the dyad activity coding system. Additionally, the mothers answered the Strengths and Difficulties Questionnaire. The results showed that, in the post-intervention, the mother-child interaction pattern improved in the BP group, especially in the teaching dimension of the PICCOLO. Also, after the program, more children with normal classification were in the BP group.
Similar content being viewed by others


Introduction
Early childhood constitutes a sensitive period for child development; however, we have been facing a huge loss of potential human development in low-and medium-income countries (Engle et al., 2011). Within the multiple necessary investments during early childhood, nurturing care (Black et al., 2017) and parenting skills (Smetana, 2017) are key aspects that promote child development.
The nurturing care framework recommends sensitivity to children’s needs, responsiveness, emotional support, appropriate stimulation for playing and exploring, and protection from adversities (Black et al., 2017). Proximal relationships in the familial context provide nurturing care to promote mental and physical benefits for child development (Jeong et al., 2021; Leclère et al., 2014). Positive parent-child engagement reduces the impact of coercion and decreases child behavior problems during early childhood (Sitnick et al., 2015).
Positive parenting includes parenting behaviors aimed at the child’s best interest to ensure the satisfaction of their needs and their empowerment and involves the commitment to protect and guide the children on their way to maturity (Brooks, 2013). In positive parenting, mother-child interactions are a key component related to mutual dyadic regulations that promote child development through synchrony, dynamic adaptation, and temporal reciprocity of behaviors (Leclère et al., 2014). The secure base for child development depends on responsive relationships, including warmth, sensitivity, and adaptability (Juffer et al., 2018; McFadden & Tamis-Lemonda, 2013). Mothers’ sensitivity and responsiveness comprise the capacity to recognize, interpret, and respond assertively to the child’s demands (McFadden & Tamis-Lemonda, 2013) and the directiveness supporting child behaviors with orientation (Potharst et al., 2012). Parenting interventions centered on responsive care positively impact on parental knowledge, interactions, practices, and the child’s cognitive development (Jeong et al., 2021).
The responsiveness and sensitivity of mothers are strongly associated with cognitive and socioemotional development during early childhood (Scherer et al., 2019). Early childhood stimulation positively impacts cerebral circuits, cognitive, language, socioemotional development, and regulatory skills (Fisher et al., 2016). Consequently, the positive quality of mother-child interactions reduces the negative impact of risk factors on children’s development (Choe et al., 2013). However, child characteristics also influence the quality of interactions, such as behavior problems (Van Dijk et al., 2017).
According to a systematic review, existing parenting intervention programs have focused on parental knowledge and skills, promoting and strengthening parental practices, reducing stress levels and emotional and behavioral problems, and improving child development (Barlow & Coren, 2018). Moreover, parenting programs have shown positive effects on attachment relationships (Pro Kind Program; Sierau et al., 2016), maternal responsiveness and sensitivity, interactional behaviors detected through several programs presented in a meta-analysis study (Mountain et al., 2017), and management of children’s oppositional-defiant behaviors (Parental Emotional Coaching; Dunsmore et al., 2013).
According to meta-analysis studies, parenting-centered interventions effectively reduce child behavior problems through positive parent-child interactions and communication (Kaminski et al., 2008), positive reinforcement, and nonviolent discipline (Leijten et al., 2019). Parenting interventions focusing on attachment improve emotional and behavioral regulation and reduce internalized and externalized behavior problems (Grube & Liming, 2018). Even though universal parenting programs have focused on the general population (Leijten et al., 2019), these preventive programs can also reach at-risk populations without stigmatization (Altafim & Linhares, 2016).
In parenting programs, the video feedback or video coaching strategy has shown evidence to promote positive parenting and child development (Balldin et al., 2018; Fisher et al., 2016; Fukkink, 2008; Juffer et al., 2017, 2018). Video feedback constitutes a learning-centered process that includes guidance to promote positive parental interactions and strengthen attachment (Fisher et al., 2016; Juffer et al., 2017, 2018), maternal sensitivity (Alvarenga et al., 2020), and to reduce significantly intrusiveness in mother-child interactions (Crugnola et al., 2021). The guidance provided via video feedback strategy should be customized to meet the personal demands of families, avoiding the use of these orientations as prescriptions with informative content exclusively (Balldin et al., 2018; Steele et al., 2014).
Furthermore, the video feedback procedure allows parents to self-observe and reflect on the interactive behaviors with their children under the guidance of a facilitator. This strategy guarantees the support of constructive comments to strengthen parental self-competence, positive parental interactions (Balldin et al., 2018; Steele et al., 2014), and parental self-efficacy (Liu et al., 2021) and reduces child behavior problems (Grube & Liming, 2018). Evidence-based parenting interventions are still relatively scarce (Van IJzendoorn & Bakermans-Kranenburg, 2017), especially with regard to programs using personalized video feedback strategies (Corralejo & Rodríguez, 2018).
Considering the delivery of parenting programs, the remote way, via mobile phones, video calls, or smartphone apps, represent a great advancement (Day et al., 2021; Harris et al., 2020). The parenting programs delivered remotely improved communication with high-risk families and reduced child behavior problems and maternal stress and depression (Carta et al., 2013). In despite of the advantages of the delivery of the programs remotely, there is a scarcity of parenting interventions using video feedback strategy in a remote way.
An innovative parenting program, named Strengthening Bonds, was delivered remotely (via WhatsApp) using a video feedback strategy with customized individual video clips of mothers interacting with their children in play-situation combined with animated video clips (standard examples of positive parenting that explain essential positive dimensions of mother-child interactions) (Linhares et al., 2022). A randomized controlled trial using the Strengthening Bonds program showed that the intervention-induced decrease in children’s behavior problems was mediated by a reduction in maternal coercive practices; also, there was a direct effect of the intervention to improve the parental sense of competence (Linhares et al., 2022). However, there were no effects of this program on mother-child interaction outcomes, which could be due to the high performance of mothers’ interactive behaviors at the baseline (“ceiling effect”).
The RCT study did not examine the effects of the Strengthening Bonds program on mother-child interactions considering, specifically, the children’s behavior characteristics. As seen in the literature, a parenting program in-group presented stronger effects for mothers with children with high levels of behavior problems at baseline (Altafim et al., 2021). Then, we need to advance to better understand the effects of child behaviors on mother-child interactions in the context of the remote video feedback Strengthening Bonds program.
The aim of the present study was to examine the effects of a personalized remote video feedback parenting program to improve mother-child interactions and child behavior outcomes among mothers of children with behavior problems in comparison to counterparts with no behavior problems. The hypotheses of the study were as follows: (i) the Strengthening Bonds program effectively improves mother-child interactions in a sample of children with behavior problems; (ii) the Strengthening Bonds program reduces child behavior problems and increases prosocial behaviors.
Method
Study design
The present study used a quasi-experimental design with between- and within-group comparisons.
Sample
The sample of the present study is a subsample of 60 participants from 92 participants of the RCT study performed in 2019-2020 (Linhares et al., 2022). The original sample of the previous RCT study comprised 92 mothers and their children, of which 50 were from the intervention group, and 42 were from the waiting-list control. In the RCT, after the post-intervention assessment, the mothers of the control group were also invited to participate in the intervention. Of the 42 mothers in the control group, 11 did not complete the intervention and the post-assessment. The samples of the intervention and waiting-list control groups were unified considering the evaluations that were carried out before and after participation in the Strengthening Bonds program. Overall, 81 mothers completed the intervention. The rate of retention in the intervention was 88%.
Of 81 mothers, 20 were excluded because the data collection was done during the COVID-19 pandemic period, leaving 61 mothers and their children eligible for the present study. Of them, one mother was excluded because the video recording of mother-child interactions was damaged. Thus, the final sample of the current study comprised 60 mothers and their children, including 19 children with indicators of behavior problems (BP group) and 41 children without behavior problems (No BP group).
In the present study, the inclusion criteria were primary female caregivers of children who might be biological mothers or have legal custody and had a 2-to-6-year-old child. The exclusion criteria, in turn, were as follows: children with disabling mental or physical illnesses; mothers with apparent cognitive impairment, which would lead to a poor understanding of assessment instructions; mothers who had already received some other type of specific intervention program aimed at strengthening mother-child interactions or parenting practices; mothers whose data collection was performed during the pandemic period.
The sample was recruited from public schools (three sites) and family health centers (two sites), comprising a sample of participants from the community population. In the schools, the recruitment of mothers was performed as follows: an invitation to mothers during parent-teacher meetings, consultation of the lists of children who met the inclusion criteria of the study in the schools and sending messages via children’s school schedules. In the family health center, eligible participants were recruited using the records of the families in the community area covered by the center. The family health centers’ and schools’ staff participated in one in-person sensitization session, mediated by the program’s facilitators (two psychologists), to explain the aim of the study and discuss the principal dimensions and examples of mother-child interactions.
Ethical aspects
The Research Ethics Committee of the Ethical Board of Hospital of Clinics of the Ribeirão Preto Medical School of the University of São Paulo approved this study. All mothers signed informed consent forms before participating in this study.
Instruments and measures
Observational assessment of mother-child interactions
Two psychologist researchers were trained by an expert researcher to apply observational coding systems to analyze the maternal and dyadic interactive behavior assessments.
Parenting Interactions with Children: A checklist of observations linked to outcomes – PICCOLO (Roggman et al., 2013). This tool measures parenting interactions in an observational play situation focusing on four domains: affection, responsiveness, encouragement, and teaching. The total score indicates the maternal global interactive skill, ranging from 0 to 58 points. Higher scores indicate more positive maternal interactive behaviors with their children. The PICCOLO guide was used with fidelity by two research assistants (psychologists) for coding the video recording of mother-child interactions. The coders were previously trained to analyze ten videos of mother-child dyads, which were not included in the sample study. Also, the reliability test (Kappa coefficient) of two independent coders was done prior to the analysis of video recordings of the final sample. The inter-rater agreement was calculated with eight mother-child dyads showing the following results in each dimension of the PICOLLO: Affection (91.50%; 𝛞 = 0.83), Responsiveness (91.10%; 𝛞 = 0.83), Encouragement (85.7%; 𝛞 = 0.72), and Teaching (88.25%; 𝛞 = 0.76).
Dynamics of the dyad activity coding system (Klein, 2005). This system evaluates the dynamics of the activity developed by the mother-child dyad in the observed play situation. The categories of this system are as follows: (a) Shared activity by the mother-child dyad, the mother and child play together performing synchronized actions in the same time interval with the same nature of the task; (b) Activity performed by the child with mother’s partial participation, the child performs actions linked to an activity and the mother observes and becomes partially involved through verbal and/or motor participation in the activity, in a synchronized and tuned way; (c) Activity performed by the mother with child’s partial participation, the mother performs actions linked to an activity and the child observes and becomes partially involved through verbal and/or motor participation in the activity partially, in a synchronized and tuned way; (d) Activity performed by the child independently of the mother, the child performs actions linked to a play activity, while the mother does not engage in any activity performed by the child; (e) Activity performed by the mother independently of the child, the mother performs actions linked to an play activity, while the child does not engage in any activity performed by the mother; (f) Parallel activity of the mothers and child, the mother and child performs, independently of each other and in the same time period, actions linked to play activities that may be similar or different. The measure was performed in units of time (1-second interval), as proposed by (Klein, 2005). The agreement rate in the original study of this system by two independent judges was 85%.
Children’s behaviors
Children’s behaviors were reported by mothers using the Strengths and Difficulties Questionnaire - SDQ (Goodman, 1997, 2005). The SDQ questionnaire was validated for the Brazilian population (Woerner et al., 2004). The SDQ is a screening tool for overall behavioral problems (range score = 0–40), specifically internalizing problems (emotional symptoms and relationship problems; range score = 0–20), externalizing problems (conduct problems and hyperactivity; range score = 0–20), and prosocial behavior (range score = 0–10). Item responses are made on a 3-point Likert scale. Higher scores indicate more behavioral problems, except for the prosocial behavior scale, in which higher scores indicate greater capacity. Also, the SDQ includes a behavior classification of normal, borderline, and clinical, based on a cut-off score of 0 - 15, 16 - 19, and 20 - 40, respectively (Goodman, 2005; https://www.sdqinfo.org/). In the present study, we considered two classifications, normal and clinical (clinical and borderline jointed), to split the children into two groups. Also, the SDQ questionnaire requires that respondents give their perceptions about child behaviors in the last six months. However, in the post-intervention assessment of the current study, the mothers were asked about the child’s behaviors at the moment.
Maternal report questionnaires of sociodemographic variables
Sociodemographic Questionnaire (developed by the authors) included information about the children’s age, gender, and racial designation, and the mother’s age, racial designation, and schooling. The classification of race/ethnicity in the current study followed the official classification of the Brazilian Institute of Geography and Statistics (IBGE) that used the skin color classification as the following: white, black, brown, yellow, and indigenous. The mothers declared the skin color of them and their children by answering the sociodemographic characteristics questionnaire.
Criteria for Economic Classification of the Brazil Association of Market Research Companies (CECB). The score ranged from 0 to 100. The assessment of the socioeconomic level of the families was based on an ordinal scale that represented very low (D/E), low (C), medium (B), and high (A) levels.
Intervention procedure
The Strengthening Bonds is a personalized remote video feedback preventive parenting program that develops and strengthens positive parenting and reduces child behavior problems (Linhares et al., 2022). This is a universal prevention program. There is an implementation guide that includes the main steps of the program, aiming to guarantee the program’s fidelity. In Step 1, there was a systematic observational session in which the facilitator recorded a 10-min video of each mother playing with their children in two different situations, free-play and structured-play situations.
In Step 2, after the dyadic observational session, the mothers participated in one 90-min structured face-to-face in group-session performed in each data collection site. In this session, the facilitator explained the concepts of parenting, child development, and positive interactions with the mothers and clarified how they could avoid negative interactions with their children. The concepts addressed in this session included explanations about parenting, the negative impact of child maltreatment and coercive practices, and positive (responsiveness, reciprocity, and adaptive directivity) and intrusive interactions, illustrated with mock videos, facilitator explanations, group activities, and role plays. In each session, three mothers were, on average.
In Step 3, personalized video feedback was customized for each mother using the recorded videos of the mother-child interactions by a team of three editors using the iMovie software in the laboratory. In this process, six videos were edited, including two composite parts, such as (i) an animated part with characters explaining the positive dimensions of mother-child interactions, which was standard for all mothers; (ii) personalized video feedback, including clips of the recorded videos with positive feedback messages presented through subtitles and emojis. Personalized video feedback focused on the mother-child interaction dimensions of responsiveness, reciprocity, and adaptive directivity. For each of these three dimensions, there were two edited videos. In the edition, the researchers chose the subtitles from a standard potential list described in the Implementation Guide of the program. The entire process of editing the videos took around 15 minutes.
In Step 4, the edited videos were uploaded to YouTube using the unlisted option. Each mother received six videos edited with personalized feedback via WhatsApp (each one per week). During the six weeks that the mothers received the videos, all the contact between the facilitator and participants was carried out remotely through standard messages forwarded via WhatsApp. The facilitator’s messages were to ensure that they watched the videos and obtained their spontaneous opinions and comments about the program. Furthermore, YouTube statistics were used to monitor whether the videos had been watched.
The Strengthening Bonds program constitutes a short intervention to improve parenting outcomes through a responsive and supportive approach using remote video feedback via WhatsApp. The intervention recognizes and encourages mothers’ responsive interactions, identifies the parents’ everyday activities with their children, and encourages them to use those interactions to support their children’s development. The emphasis on maternal responsiveness, reciprocity, and adaptive directivity strengthens parental practices and beliefs and observes and offers contingent comments using subtitles and emojis in personalized videos. The personalized video feedback follows the “feedforward strategy,” in which the feedback is focused only on positive behaviors that are reinforced. Ineffective parenting behaviors are not mentioned in the personalized feedback.
Data collection procedure
The data collection of the present study was carried out from April 2019 to January 2020, prior to the pandemic period. The procedure was performed by three trained research assistants (psychologists) supervised by three expert principal investigators and developers of the study.
The mothers participated in three phases: pre-intervention assessment, intervention with the Strengthening Bonds program, and post-intervention assessment. Figure 1 shows the data collection schedule of the present study.

Data collection schedule
As seen in Fig. 1, first, the mothers were invited to participate in the study. After they signed the informed consent form, a pre-intervention assessment was performed to collect the maternal report measures. Then, an observational 10-min session was performed to record the mother-child interactions using a tablet, equally divided into free-play situations (i.e., toys, such as small animals, cooking toys, and building blocks) and structured-play situations (i.e., puzzles). The recorded video was used for the baseline evaluation of the mother-child’s interactive behavior (pre-intervention assessment). Finally, one week after the intervention, a post-intervention assessment was conducted. This evaluation comprised a second observational session of mother-child interactions (free- and structured-play situations, with the same instructions and toys) and maternal responses to the same questionnaires used in the pre-intervention assessment. The pre-and post-intervention assessments were performed individually. It is important to highlight that the 10-minute video recording of the mother-child interaction pre-intervention session was used to evaluate the mothers’ interactive behaviors and select clips for editing the personalized videos of the intervention.
Data analysis
The observational data of maternal interactive behaviors were coded using all the coding systems by one expert researcher (third author) and one assistant researcher. The coders received the videos in a mixed order aiming to guarantee that they were blinded to the characteristics of the participants (BP and No BP groups) and the time points (pre-intervention and post-intervention moments). The Observer XT software (9.0 version; Noldus Information Technology, USA) was used to encode the system of dynamics of dyad activity in units of time (1-second interval), as proposed by Klein (2005). In the data analysis, the participants were distributed according to the children’s behavior problems identified through SDQ in the pre-intervention assessment. Thus, the No-BP group included 41 mothers, and the BP group included 19 mothers.
The dataset was organized and double-checked. First, descriptive statistical analysis was performed using median, minimum, and maximum values for continuous variables and frequency and percentages for categorical variables. Second, the between-group comparisons (BP vs. No BP) were made using the Mann-Whitney test for continuous variables and the Chi-square test for categorical variables. Third, within-group comparisons (pre-intervention vs. post-intervention assessments) were made for each group, respectively, using the Wilcoxon test for continuous variables and the McNemar test for categorical variables. All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS, 23.0 version; II, Chicago, USA), and the statistical significance was set at 5% (p ≤ 0.05).
Results
Characteristics of the study sample
Table 1 shows the main sociodemographic characteristics of the No BP and BP groups. In both groups, there was a similar distribution between boys and girls, aged predominantly between 2 and 3 years old. A statistically significant difference was observed regarding the children’s and mothers’ skin color; more children and mothers in the BP with brown and black skin color than in the No BP group. Regarding maternal characteristics, the groups were mainly composed of young adult women with 12 years of schooling from medium socioeconomic levels (B and C). Regarding the groups that were different in skin color characteristics, this variable was considered in the analyses in the between-group comparisons.
Additionally, in the pre-intervention, there were statistically significant differences between groups in the total behavior problems score (BP group, median score = 17 [14-25] and No BP = 9 [2-13]; p ≤ 0.0001), externalizing score (BP group, median score = 12 [4-16] and No BP = 6 [0-10]; p ≤ 0.0001), and internalizing score (BP group, median score = 6 [2-12] and No BP = 3 [0-9]; p ≤ 0.0001). As expected, the BP group had higher scores in all dimensions of behavior in comparison to the No BP group. Regarding prosocial behavior, the groups showed similar scores (BP group, median score = 9 [4-10] and No BP = 9 [5-10]; p ≤ 0.95).
Mother-child interactions
Dynamics of dyadic interactions in the play activities
In the dynamic of dyadic interactions, the play activities were predominantly shared between mother and child in the 300 seconds of the observational session, in both groups and time points (pre-and post-intervention assessments). In the free-play situation, the No BP group presented a median of 300 seconds (132–300) in the pre-intervention and 282 seconds (134–300) in the post-intervention (p = 0.08). The BP group, in turn, showed a median of 281 seconds (79–300) in the pre-intervention and 300 seconds (12–300) in the post-intervention (p = 0.83). In the structured-play situation, the No BP group presented a median of 300 seconds (87–300) in the pre-intervention and 300 seconds (15–300) in the post-intervention (p = 0.06). The BP group showed a median of 300 seconds (153–300) in the pre-intervention and 300 seconds (16–300) in the post-intervention (p = 0.89).
Mothers’ interactive behaviors in the play situation
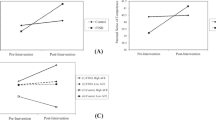
Concerning the free-play situation, Table 2 shows that there were no statistically significant differences between the BP and No BP groups; the scores of both groups were similar at the pre-intervention and post-intervention moments in all dimensions of maternal interactive behaviors, as assessed by the PICCOLO. Additionally, the within-group comparisons found no statistically significant differences between the pre-and post-intervention PICCOLO scores of the BP and No BP groups.
Regarding the structured-play situation, Table 3 reveals that the comparison between groups showed a marginal statistical trend of differences between groups in the responsiveness domain in the pre-intervention period. The BP group had lower scores in these domains than the No BP group. However, in the post-intervention period, differences between groups were not maintained; the groups showed a similar maternal interactive behavior pattern in all PICCOLO domains.
In the within-group comparison, the BP group had statistically significantly higher scores in the total maternal interactive behaviors and teaching behavior in the post-intervention compared to the pre-intervention, regardless of the skin color of both mothers and children. Additionally, there was a statistical trend of improvement in the mothers’ responsiveness domain. The other dimensions of mothers’ interactive behaviors in both groups did not show statistically significant differences between the pre-and post-intervention time points.
Children’s behaviors at post-intervention
As seen in Table 4, the differences between groups of the children’s behaviors remained at the post-intervention. The BP group had significantly higher SDQ total score and higher percentage of children with clinical behaviors in comparison to the No BP. Additionally, there were no significant differences between groups considering the skin colors of mothers and children.
In the BP group, the within-group comparisons showed statistically significant differences. In spite of there being no significant differences in the total behavior score, the percentage of children with behavior problems decreased in the post-intervention assessment in comparison to the pre-intervention assessment. Then, after the intervention, the BP group had 37% of the children presenting normal behaviors in the SDQ assessment. In the No BP group, in turn, the total score decreased significantly from pre-intervention to post-intervention; however, the pattern of the low percentage of children with clinical behavior problems was maintained.
Discussion
The present study examined the effectiveness of the strengthening bonds program to promote positive interactions between mothers and their children in groups differentiated by the presence of behavior problems. Regarding the dynamics of the activities performed by the mother-child dyad, in both groups, most dyads remained in shared activity during most of the observation of playing. These results demonstrate that, even before the intervention, most dyads showed a pattern of synchrony and reciprocity that remained after the intervention, showing a “ceiling effect.” The support provided by the caregiver during the first years of life is essential for the child to feel encouraged and safe to explore the environment (Jeong et al., 2021). In the interactional experiences context, children learn and internalize the skills and competencies relevant to child development (Fisher et al., 2016).
The present study broadens the understanding of the Strengthening Bonds mechanisms of action, and for whom the program works. The findings showed that mothers of children with no behavior problems at baseline already present positive interactive behaviors; therefore, they do not present changes from the pre- to post-intervention, showing a “ceiling effect”. However, mother-child dyads with child behavior problems improved their general maternal interactive behaviors and teaching behaviors post-intervention compared to pre-intervention moments. Therefore, the hypothesis of the present study was confirmed.
A previous randomized controlled trial showed the efficacy of the Strengthening Bonds program in decreasing child behavior problems after the mothers participated in the program, which was mediated by the decrease in mothers’ coercive practices (Linhares et al., 2022). Also, the program directly impacted mothers’ sense of competence. However, no changes in the mother-child interaction were observed in the RCT. Thus, considering the findings of the previous RCT and the present study, the Strengthening Bonds improve mothers’ parenting practices in general, regardless of maternal or child characteristics, and increase mother-child interactions of mothers with children with behavior problems.
Interestingly, the Strengthening Bonds program is more sensitive in promoting changes in the interactive behaviors of mothers in the group of children with behavioral problems at baseline. These data are in accordance with the findings of Altafim et al. (2021) and Leijten (2019), which indicated that children with higher levels of behavior problems tend to have higher positive impacts after participating in parenting programs, even in universal preventive parenting interventions.
Additionally, the mothers who perceive greater risk indicators, such as behavior problems in children, show greater motivation for change and become more involved with the strategies taught and the activities proposed during the program.
Specifically, the teaching dimension assessed by the PICCOLO involves cognitive stimulation through questions asked to the child, explanations, and clear demonstrations during the activity (Roggman et al., 2013). This dimension of maternal interactive behavior can be related to adaptive directivity, in which the mother supports the child during the activity while respecting their autonomy (Potharst et al., 2012).
The results that indicated an improvement in the global interactive pattern after the mother’s participation in the intervention showed that the mothers started to present a set of increased positive behaviors compared to the baseline assessment. Different domains of the mother-child interaction were addressed and discussed throughout the Strengthening Bonds program, both in the face-to-face group session and at the time of remote video feedback, which reinforced the value of affective relationships for the child’s development and offered a space for discussion and reflection to facilitate learning. Adaptive directivity is one of the key concepts addressed by the program. In the face-to-face session, the facilitators presented the concept of directivity through explanations, modeling videos, and discussions so that the mother could understand the concept and think about how it could be applied in their daily life with the child.
The findings of the present study are consistent with the previous literature indicating that video feedback programs can be effective in promoting different aspects of mother-infant interaction, leading to more responsive parenting and more harmonious relationships (Balldin et al., 2018). Studies using this methodology have also shown improvement in maternal responsiveness and attachment relationships (Crugnola et al., 2021) and increased maternal sensitivity combined with less intrusiveness (Alvarenga et al., 2020).
The interactive changes in the BP group occurred during the structured play situation, which involved problem-solving game activities. Unlike the free play situation, guided play implies greater participation and subtle guidance by an adult to ensure specific learning, which can provide clues for the child to reach the goals in the activity, thereby preserving the child’s autonomy (Weisberg & Zosh, 2018). These characteristics are similar to the structured play activity used in the present study. It is possible that, after the intervention, the environment of the structured play activity has favored the use of maternal teaching behavior using strategies to assist and guide the child in problem-solving games.
We confirmed the hypothesis of reducing children’s behavior problems. After the program, it was found that there was a significant increase in the percentage of children (zero to 37%) in the BP group whose behavior was classified as normal. Concurrently, children in the No BP group showed a significant improvement in behavior after the intervention concerning the total SDQ score. The findings of the present study confirm the results of other previous studies using video feedback strategies that indicated the effectiveness of this type of intervention in promoting improvements in children’s behaviors (Juffer et al., 2017), decreasing externalizing and internalizing problems, and improving children’s emotional regulation (Grube & Liming, 2018).
Parenting programs focusing on mother-child interactions and sensitive communication components effectively promote changes in children’s practices and behaviors (Kaminski et al., 2008). Through parenting programs, learned maternal behavioral and emotional regulation can mediate the effect of interventions on children’s behavior problems (Altafim et al., 2021).
Our results contribute to the literature by demonstrating that technology-based programs improve mother-child interactions of mothers of children with behavior problems. A previous intervention study on parents of children with disruptive problems combined content delivered on a digital platform with weekly calls provided by a coach (Sourander et al., 2016). At the 12-month follow-up, the intervention group showed significantly more significant improvements than the control group in the total scores and both externalizing and internalizing axes. Digital technologies for delivering parenting interventions are being used increasingly (Day et al., 2021). Programs based on self-administered technologies (e.g., smartphone apps) and remote delivery allow parents more flexibility, besides reducing delivery costs and logistical barriers to program access (Sanders et al., 2019). A review by Corralejo and Rodríguez (2018), which included feasibility studies of technology-based programs, found positive results regarding the satisfaction, adaptation, and engagement of participating parents, even in groups with different ethnic origins and educational levels, showing the potential of the remote approach.
It should be noted that although most of the Strengthening Bonds Program is conducted remotely through videos and has a self-administered character, the videos sent to the mothers offer specific feedback related to the interactive moment of the dyad itself. Thus, the program has important elements: the personalization of content and constant contact with a facilitator. Some studies have shown that using technologies in parenting programs that include direct contact with a coach can help them engage in the interventions to enable significant and sustainable changes in parenting behaviors and promote changes in children’s behaviors (Sanders et al., 2019). The Strengthening Bonds program is a universal parenting program that does not focus on the target population of mothers of children with behavior problems. This advantage can benefit mothers of all children, reducing exposure to stigmatization, as highlighted by Branco et al. (2021).
The opportunity to watch one’s interactive behavior objectively on a screen mobilizes self-reflective processes, which are essential for strengthening the process of learning and acquiring new skills offered by video feedback programs (Fukkink, 2008; Steele et al., 2014). In this process, content personalization is also highlighted, adapting to the needs of mother-child dyads. The Strengthening Bonds program is not only prescriptive and informative but offers, through the process of remote video feedback, contingent comments that value positive aspects already perceived and observed in the interaction (Linhares et al., 2022). The findings of the present study confirm that interventions mediated by technological and digital resources strengthen affective relationships between mothers and children.
As highlighted in the literature, even short video feedback interventions can positively impact mother-child relationships (Fukkink, 2008). The Strengthening Bonds program is a short-term remote video feedback intervention with only one face-to-face meeting and makes six short videos with personalized content for mothers available remotely. According to Harris et al. (2020), shorter approaches can be even more beneficial for groups that experience some potential risk since longer interventions can become an obstacle to the engagement and completion of programs by these families. Technological approaches can be more flexible, reaching many families (Corralejo & Rodríguez, 2018; Harris et al., 2020). It is important to note that the retention rate of 88% observed in the present study was higher than the 61% obtained in a previous study of parenting programs conducted in groups by face-to-face meetings with a similar population (Altafim et al., 2016). It is possible that the combination of a single face-to-face meeting with videos delivered remotely via a smartphone contributed to the participants’ engagement and adherence.
The present study presented some strengths. The Strengthening Bonds program promoted positive maternal interactive behaviors in the dyads with children with behavior problems. As highlighted by Shonkoff and Fisher (2013), evidence-based parenting programs show intergenerational impact when strengthening positive parenting and consequently minimizing risks for child development. The Strengthening Bonds program is flexible and mostly digital and can be implemented together with other standard services already available in public services. Other digital programs have used similar strategies, in which mothers not only received standard health appointments but also participated in an online parenting program run by a nurse trained in child development (Sawyer et al., 2017). The results suggested that the standard support offered to mothers by the clinic, combined with the online group intervention, can achieve results comparable to those achieved through home visiting programs (Sawyer et al., 2017). Then, the Strengthening Bonds present practical value to improve the mother-child interactions in services centered on parents of children at early ages in health, educational, or social assistance settings. The program delivered remotely showed high adherence from the participants. Finally, it is important to highlight that currently, an app was developed to perform the entire video editing process that facilitates the transition to a large scale (Vale et al., 2022).
The present study has some limitations. Despite the good adherence rate of participants, there was a drop-out of participants, which is one of the biggest challenges in intervention studies. As expected in a community population, there was a small sample of children with behavior problems in the current study; however, the percentage is similar to previous studies using no target population. Then non-parametric tests were then performed, which are limited in simultaneously performing the mixed model analysis of between- and within-group comparisons. The mothers were the unique informant in the report measures in two moments, pre- and post-intervention assessments.
Future studies should include large samples with replication of the Strengthening Bonds intervention in different contexts with children at early ages (e.g., educational, health, and social assistance services) and conduct follow-up evaluations to assess the impacts of the intervention in the medium- and long-term. In addition, the current study sample was recruited in the community using a screening tool to detect indicators of behavior problems. Future studies could examine how the Strengthening Bond program works for the target population of children with behavioral clinical diagnoses.
Data availability
The datasets generated during and analyzed during the current study are available from the corresponding author upon reasonable request.
References
Altafim, E. R. P., & Linhares, M. B. M. (2016). Universal violence and child maltreatment prevention programs for parents: A systematic review. Psychosocial Intervention, 25(1), 27–38. https://doi.org/10.1016/j.psi.2015.10.003
Altafim, E. R. P., Pedro, M. E. A., & Linhares, M. B. M. (2016). Effectiveness of ACT raising safe kids parenting program in a developing country. Children and Youth Services Review, 70, 315–323. https://doi.org/10.1016/j.childyouth.2016.09.038
Altafim, E. R. P., McCoy, D. C., & Linhares, M. B. M. (2021). Unpacking the impacts of a universal parenting program on child behavior. Child Development, 92(2), 626–637. https://doi.org/10.1111/cdev.13491
Alvarenga, P., Cerezo, M. A., Wiese, E., & Piccinini, C. A. (2020). Effects of a short video feedback intervention on enhancing maternal sensitivity and infant development in low-income families. Attachment & Human Development, 22(5), 534–554. https://doi.org/10.1080/14616734.2019.1602660
Balldin, S., Fisher, P. A., & Wirtberg, I. (2018). Video feedback intervention with children: A systematic review. Research on Social Work Practice, 28(6), 682–695. https://doi.org/10.1177/104731516671809
Barlow, J., & Coren, E. (2018). The effectiveness of parenting programs: A review of Campbell reviews. Research on Social Work Practice, 28(1), 99–102. https://doi.org/10.1177/1049731517725184
Black, M. M., Walker, S. P., Fernald, L. C., Andersen, C. T., DiGirolamo, A. M., Lu, C., McCoy, D. C., Fink, G., Shawar, Y. R., Shiffman, J., Devercelli, A. E., Wodon, Q. T., Vargas-Barón, E., Grantham-McGregor, S., & Lancet Early Childhood Development Series Steering Committee. (2017). Early childhood development coming of age: Science through the life course. The Lancet, 389(10064), 77–90. https://doi.org/10.1016/S0140-6736(16)31389-7
Branco, M. S. S., Altafim, E. R. P., & Linhares, M. B. M. (2021). Universal intervention to strengthen parenting and prevent child maltreatment: Updated systematic review. Trauma, Violence, & Abuse. https://doi.org/10.1177/15248380211013131
Brooks, J. (2013). The process of parenting. McGraw Hill.
Carta, J. J., Lefever, J. B., Bigelow, K., Borkowski, J., & Warren, S. F. (2013). Randomized trial of a cellular phone-enhanced home visitation parenting intervention. Pediatrics, 132(Suppl. 2), S167–S173. https://doi.org/10.1542/peds.2013-1021Q
Choe, D. E., Olson, S. L., & Sameroff, A. J. (2013). Effects of early maternal distress and parenting on the development of children's self-regulation and externalizing behavior. Developmental Psychology, 25(2), 437–453. https://doi.org/10.1017/S0954579412001162
Corralejo, S. M., & Rodríguez, M. M. D. (2018). Technology in parenting programs: A systematic review of existing interventions. Journal of Child and Family Studies, 27(9), 2717–2731. https://doi.org/10.1007/s10826-018-1117-1
Crugnola, C. R., Ierardi, E., Peruta, V., Moioli, M., & Albizzati, A. (2021). Video-feedback attachment-based intervention aimed at adolescent and young mothers: Effectiveness on infant-mother interaction and maternal mind-mindedness. Early Child Development and Care, 191(3), 475–489. https://doi.org/10.1080/03004430.2019.1652172
Day, J. J., Baker, S., Dittman, C. K., Franke, N., Hinton, S., Love, S., Sanders, M. R., & Turner, K. M. (2021). Predicting positive outcomes and successful completion in an online parenting program for parents of children with disruptive behavior: An integrated data analysis. Behaviour Research and Therapy, 146, 103951. https://doi.org/10.1016/j.brat.2021.103951
Dunsmore, J. C., Booker, J. A., & Ollendick, T. H. (2013). Parental emotion coaching and child emotion regulation as protective factors for children with oppositional defiant disorder. Social Development, 22(3), 1–35. https://doi.org/10.1111/j.1467-9507.2011.00652.x
Engle, P. L., Fernand, L. C., Alderman, H., Behrman, J., O’Gara, C., Yousafzai, A., Mello, M. C., Hidrobo, M., Ulkuer, N., Ertem, I., Iltus, S., & Global Child Development Steering Group. (2011). Strategies for reducing inequalities and improving developmental outcomes for young children in low-income and middle-income countries. The Lancet, 378(9799), 1339–1353. https://doi.org/10.1016/S0140-6736(11)60889-1
Fisher, P., Frenkel, T. I., Noll, L. K., Berry, M., & Yockelson, M. (2016). Promoting healthy child development via two-generation translational neuroscience framework: The filming interactions to nurture development video coaching program. Child Development Perspectives, 10(4), 251–256. https://doi.org/10.1111/cdep.12195
Fukkink, R. G. (2008). Video feedback in widescreen: A meta-analysis of family programs. Clinical Psychology Review, 28(6), 904–916. https://doi.org/10.1016/j.cpr.2008.01.003
Goodman, R. (1997). The strengths and difficulties questionnaire a research note. Journal Child Psychology and Psychiatry, 38(5), 581–586. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x
Goodman, R. (2005). Questionário de Capacidades e Dificuldades (SDQ-Por) [Strengths and Difficulties Questionnaire (SDQ-Por)]. Retrieved January 03, 2019, from https://www.sdqinfo.org/
Grube, W. A., & Liming, K. W. (2018). Attachment and biobehavioral catch-up: A systematic review. Infant Mental Health Journal, 39(6), 656–673. https://doi.org/10.1002/imhj.21745
Harris, M., Andrews, K., Gonzalez, A., Prime, H., & Atkinson, L. (2020). Technology-assisted parenting interventions for families experiencing social disadvantage: A meta-analysis. Prevention Science, 21(5), 714–727. https://doi.org/10.1007/s11121-020-01128-0
Jeong, J., Franchett, E. E., Oliveira, C. V. R., Rehmani, K., & Yousafzai, A. K. (2021). Parenting interventions to promote early child development in the first three years of life: A global systematic review and meta-analysis. PLoS Medicine, 18(5), e1003602. https://doi.org/10.1371/journal.pmed.1003602
Juffer, F., Bakermans-Kranenburg, M. J., & Van IJzendoorn, M. H. (2017). Pairing attachment theory and social learning theory in video-feedback intervention to promote positive parenting. Current Opinion in Psychology, 15, 189–194. https://doi.org/10.1016/j.copsyc.2017.03.012
Juffer, F., Bakermans-Kranenburg, M. J., & Van IJzendoorn, M. H. (2018). Video-feedback intervention to promote positive parenting and sensitive discipline: Development and meta-analytic evidence and effectiveness. In H. Steele & M. Steele (Eds.), Handbook of attachment-based interventions (pp. 1–26). Guilford.
Kaminski, J. W., Valle, L. A., Filene, J. H., & Boyle, C. L. (2008). A meta-analytic review of components associated with parent training program effectiveness. Journal of Abnormal Child Psychology, 36(4), 567–589. https://doi.org/10.1007/s10802-007-9201-9
Klein, V. C. (2005). Interação entre mães e crianças pré-escolares nascidas pré-termo e com muito baixo peso em situação lúdica e de ensino [Interaction between mothers and preschool children born preterm and with very low birth weight in a playful and educational situation; Unpublished master’s thesis]. University of Sao Paulo.
Leclère, C., Viaux, S., Avril, M., Achard, C., Chetouani, M., Missonnier, S., & Cohen, D. (2014). Why synchrony matters during mother-child interactions: A systematic review. PLoS One, 9(12), e113571. https://doi.org/10.1371/journal.pone.0113571
Leijten, P., Gardner, F., Melendez-Torres, G. J., Van Aar, J., Hutchings, J., Schulz, S., Knerr, W., & Overbeek, G. (2019). Meta-analyses: Key parenting program components for disruptive child behavior. Journal of the American Academy of Child & Adolescent Psychiatry, 58(2), 180–190. https://doi.org/10.1016/j.jaac.2018.07.900
Linhares, M. B. M., Altafim, E. R., de Oliveira, R. C., & Gaspardo, C. M. (2022). A personalized remote video-feedback universal parenting program: A randomized controlled trial. Psychosocial Intervention, 31(1), 21–32. https://doi.org/10.7440/res64.2018.03
Liu, S., Phu, T., Dominguez, A., Hurwich-Reiss, E., McGee, D., Watamura, S., & Fisher, P. (2021). Improving caregiver self-efficacy and children's behavioral outcomes via a brief strength-based video coaching intervention: Results from a randomized controlled trial. Prevention Science, 1-14. https://doi.org/10.1007/s11121-021-01251-6
McFadden, K. E., & Tamis-Lemonda, C. S. (2013). Maternal responsiveness, intrusiveness, and negativity during play with infants: Contextual associations and infant cognitive status in a low-income sample. Infant Mental Health Journal, 34(1), 80–92. https://doi.org/10.1002/imhj.21376
Mountain, G., Cahill, J., & Thorpe, H. (2017). Sensitivity and attachment interventions in early childhood: A systematic review and meta-analysis. Infant Behavior and Development, 46, 14–32. https://doi.org/10.1016/j.infbeh.2016.10.006
Potharst, E. V., Schuengel, C., Last, B. F., Wassenaer, A. G., Kok, J. H., & Houtzager, B. A. (2012). Difference in mother-child interaction between preterm- and term-born preschoolers with and without disabilities. Acta Paediatrica, 101(6), 597–603. https://doi.org/10.1111/j.1651-2227.2012.02599.x
Roggman, L. A., Cook, G. A., Innocenti, M. S., Norman, V., & Christiansen, K. (2013). Parenting interactions with children: Checklist observations linked to outcomes. Brookes.
Sanders, M. R., Turner, K. M. T., & Metzler, C. W. (2019). Applying self-regulation principles in the delivery of parenting interventions. Clinical Child and Family Psychology Review, 22(1), 24–42. https://doi.org/10.1007/s10567-019-00287-z
Sawyer, M. G., Reece, C. E., Bowering, K., Jeffs, D., Sawyer, A. C., Mittinty, M., & Lynch, J. W. (2017). Nurse-moderated internet-based support for new mothers: Non-inferiority, randomized controlled trial. Journal of Medical Internet Research, 19(7), e258. https://doi.org/10.2196/jmir.6839
Scherer, E., Hagaman, A., Chung, E., Rahman, A., O’Donnell, K., & Maselko, J. (2019). The relationship between responsive caregiving and child outcomes: Evidence from direct observations of mother-child dyads in Pakistan. BMC Public Health, 19(1), 1–10. https://doi.org/10.1186/s12889-019-6571-1
Shonkoff, J. P., & Fisher, P. A. (2013). Rethinking evidence-based practice and two-generation programs to create the future of early childhood policy. Development and Psychopathology, 25(4 Pt 2), 1635–1653. https://doi.org/10.1017/S0954579413000813
Sierau, S., Dähne, V., Brand, T., Kurtz, V., Von Klitzing, K., & Jungmann, T. (2016). Effects of home visitation on maternal competencies, family environment, and child development: A randomized controlled trial. Prevention Science, 17(1), 40–51. https://doi.org/10.1007/s11121-015-0573-8
Sitnick, S. L., Shaw, D. S., Gill, A., Dishion, T., Winter, C., Waller, R., Gardner, F., & Wilson, M. (2015). Parenting and the family check-up: Changes in observed parent-child interaction following early childhood intervention. Journal of Clinical Child & Adolescent Psychology, 44(6), 970–984. https://doi.org/10.1080/15374416.2014.940623
Smetana, J. G. (2017). Current research on parenting styles, dimensions, and beliefs. Current Opinion in Psychology, 15, 19–25. https://doi.org/10.1016/j.copsyc.2017.02.012
Sourander, A., McGrath, P. J., Ristkari, T., Cunningham, C., Huttunen, J., Lingley-Pottie, P., Hinkka-Yli-Salomäki, S., Kinnunen, M., Vuorio, J., Sinokki, A., Fossum, S., & Unruh, A. (2016). Internet-assisted parent training intervention for disruptive behavior in 4-year-old children: A randomized clinical trial. JAMA Psychiatry, 73(4), 378–387. https://doi.org/10.1001/jamapsychiatry.2015.3411
Steele, M., Steele, H., Knafo, J. B. H., Kinsey, M., Bonuck, K., Meisner, P., & Murphy, A. (2014). Looking from the outside in: The use of video in attachment-based interventions. Journal Attachment & Human Development, 16(4), 402–415. https://doi.org/10.1080/14616734.2014.912491
Vale, R. E. D., Altafim, R. A. P., Altafim, E. R. P., & Linhares, M. B. M. (2022). Aplicativo Para produção de vídeos em smartphone com foco em video coaching [application for video production on smartphone with focus on video coaching]. Comunicações em Informática, 6(2), 1–4. https://doi.org/10.22478/ufpb.2595-0622.2022v6n2.62180
Van Dijk, R. V., Deković, M., Bunte, T. L., Schoemaker, K., Zondervan-Zwijnenburg, M., Espy, K. A., & Matthys, W. (2017). Mother-child interactions and externalizing behavior problems in preschoolers over time: Inhibitory control as a mediator. Journal of Abnormal Child Psychology, 45(8), 1503–1517. https://doi.org/10.1007/s10802-016-0258-1
Van IJzendoorn, M. H., & Bakermans-Kranenburg, M. J. (2017). Editorial overview: Multidisciplinary and interdisciplinary perspectives on parenting. Current Opinion in Psychology, 15, 4–7. https://doi.org/10.1016/j.copsyc.2017.05.001
Weisberg, D. S., & Zosh, J. M. (2018). How guided play promotes early childhood learning. Encyclopedia on Early Childhood Development. https://www.child-encyclopedia.com/play-based-learning/according-experts/how-guided-play-promotes-early-childhood-learning. Accessed 10 Feb 2023
Woerner, W., Fleitlich-Bilyk, B., Martinussen, R., Fletcher, J., Cucchiaro, G., Dalgalorrondo, P., Lui, M., & Tannock, R. (2004). The strengths and difficulties questionnaire overseas: Evaluations and applications of the SDQ beyond Europe. European Child & Adolescent Psychiatry, 13, 47–54. https://doi.org/10.1007/s00787-004-2008-0
Acknowledgments
The authors are grateful to all the study participants. The authors are also thankful to the research assistants who participated in this study (Fernanda Leite Ongílio, Marina Dias Macedo de Melo Avezum, and Maria Julia Silveira Cassiano).
Funding
The Foundation for Support of Research in the State of São Paulo, Brazil (FAPESP, grant 2019/18674-4) for RC de Oliveira. The National Council for Scientific and Technological Development, Brazil (CNPq, Grant 310726/2021-2) for MBM Linhares. The Strengthening Bonds (RCT study) was supported by the Laboratory of Innovation for Early Childhood Development (I-Lab Primeira Infância), an initiative of the Center of Science for Early Childhood (Núcleo de Ciência pela Infância).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
de Oliveira, R.C., Altafim, E.R.P., Gaspardo, C.M. et al. Strengthening mother-child interactions among mothers and children with behavior problems at early development. Curr Psychol 43, 6062–6074 (2024). https://doi.org/10.1007/s12144-023-04786-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-023-04786-9