
Abstract
Sensory sensitivities in children are found not only across a range of childhood disorders, but also within the general population. The current exploratory study examines the reliability and validity of a novel parent-report measure which assesses sensory-sensitivities in both typically developing and non-typically developing children. This 42-item Parent-completed Glasgow Sensory Questionnaire (GSQ-P) has been adapted by us from an existing adult tool (Glasgow Sensory Questionnaire), and measures children’s hyper-sensitivities (sensory overload leading to avoidance-behaviours) and hypo-sensitivities (sensory dampening leading to seeking-behaviours) across seven different sense domains (visual, auditory, gustatory, olfactory, tactile, vestibular, proprioception). We validated this novel measure on the parents of 601 English children 6–11 years. Both the long version (42-items GSQ-P) and an additional reduced version (24-item rGSQ-P) significantly associated with children’s anxiety, behavioural difficulties, and ability to empathise. As expected, sensory sensitivities were invariant across age and gender, but non-typically developing children had significantly elevated scores compared to typically developing peers (in both GSQ-P and rGSQ-P). We also provide insight into the structure of sensory sensitivities in children, showing for the first time that hyper sensitivities cluster by sense (e.g., tactile questions cluster together; visual questions cluster together) whilst hypo sensitivities cluster by behaviour (e.g., a cluster of seeking-behaviours irrespective of sense; a cluster of sensory dampening irrespective of sense). We offer both instruments (GSQ-P and rGSQ-P) as free reliable measures for better understanding children’s sensitivities, for use in different circumstances depending on focus.
Highlights
-
The paper explores two new parent-report sensory sensitivity questionnaires adapted from the adult Glasgow Sensory Questionnaire.
-
Sensory sensitivity scores were invariant across age groups (6–10 years) and between girls and boys.
-
Anxiety, internalising behaviours and poorer empathy were associated more closely with hyper-sensitivity, whereas externalising behaviours were associated more with hypo-sensitivity.
-
Hyper-sensitivity items clustered together within sense modalities, whereas hypo-sensitivity items tendered to cluster by behavioural manifestation.
Similar content being viewed by others


Sensory sensitivity is characterised by over- (hyper) or under- (hypo) responding to sensory stimuli, and can occur within a number of different sense domains (e.g., visual, auditory, olfactory, gustatory, tactile, vestibular, proprioceptive). Hyper-sensitivity typically incorporates sensory overload and avoidance behaviours, while hypo-sensitivity incorporates sensory under-responsivity and seeking behaviours. For example, a person with hyper-sensitivity might find strong smells overwhelming (i.e., sensory overload) and avoid them (i.e., sensory avoidance), while a person with hypo-sensitivity might fail to notice strong smells at all (i.e., sensory under-responsivity or ‘dampening’) and actively seek them out (i.e., sensory seeking). Children can find sensory information more disruptive than adults (Ahn et al., 2004), but their sensory sensitivities are poorly understood. Limited research has concentrated to a large extent on clinical groups (see below), but beyond clinical groups, our knowledge is vague. One barrier has been a lack of instruments that can measure childhood sensory sensitivities across both clinical and non-clinical populations, while also adequately capturing the complexity of sensory experiences and their multifaceted nature. Any useful measure would need to be able to test multiple sense domains (vision, audition, olfaction etc.), for both hyper and hypo sensitivity, with both sensory and behavioural components (i.e., overload/dampening vs. avoidance/seeking). The current paper presents an instrument which aims to fulfil all these requirements.
We noted above that research in sensory sensitivities has tended to focus on clinical populations, and in particular, on children with an Autism Spectrum Condition (ASC), also known as Autism Spectrum Disorder (ASD; henceforth autism) where sensitivities are particularly high (Baranek et al., 2007; Billstedt et al., 2007; McCormick et al., 2016; Robertson and Simmons, 2013; Watling et al., 2001). Indeed sensory sensitivities now form part of the diagnostic criteria for autism within the Diagnostic and Statistical Manual of Mental Disorders (DSM-V: American Psychiatric Association 2013). Other conditions, too, show sensory sensitivities, including Attention Deficit Hyperactivity Disorder (Cheung & Siu, 2009; Ghanizadeh, 2011; Panagiotidi et al., 2018; Yochman et al., 2004), childhood developmental delays (Baranek et al., 2007; McCormick et al., 2016), Tourette’s syndrome (Isaacs & Riordan, 2020), and premature births (Rahkonen et al., 2015). Moreover, sensory sensitivities are found not only within clinical populations, but are also in approximately 1 in 6 typically developing children (Ahn et al., 2004; with a notable degree of within-group variation; Brockevelt et al., 2013; Cheung & Siu, 2009) meaning as many as five children with sensitivities arise within the average English primary school classroom. The exact sensory profile of typically and non-typically developing groups requires more research (Tomchek et al., 2014), but in autistic children for example, sensory behaviours are known to cluster together, such as tactile/movement sensitivity, taste/smell sensitivity, auditory/smell sensitivity. And environmental interactions are also important; hence a child may find loud noise in a supermarket unbearable but play music loudly at home.
It is important to have a clear understanding of (and validated tests for) sensory sensitivities in children, for a number of reasons. Sensory sensitivities can have a significant impact on children’s lives, and where sensitivities arise, they present early in development (Ben-Sasson et al., 2010). Dunn, and colleagues found that children with higher levels of sensory processing issues were more likely to have difficulties in everyday routines such as eating, playing, family interactions, and other social/activity participation (Dunn et al., 2016). Hyper-sensitivities in particular (described by Dunn et al. as ‘Low threshold’) were associated with higher levels of anxiety, shyness and more challenging behaviours. Indeed, sensory sensitivities have been linked to elevated anxiety in both typically and non-typically developing children (Green et al., 2012; Lane et al., 2012; Neil et al., 2016; Reynolds & Lane, 2009). Conversely, hypo–sensitivities (described by Dunn et al. as ‘high threshold’) are associated with under-responsivity and potentially repetitive self-harming behaviours. In otherwise typically developing populations, sensory sensitivities are also linked to reduced play behaviours (Bundy et al., 2007), compulsive-like behaviour (Dar et al., 2012), modulated movement (Buitendag & Aronstam, 2010; Gal et al., 2010), and feeding problems (Davis et al., 2013; Smith et al., 2020). They can also impede social participation (Engel-Yeger and Dunn, 2011; Hochhauser & Engel-Yeger, 2010), sleep behaviours (Reynolds et al., 2011), and classroom learning (Ashburner et al., 2008; Baranek et al., 2013; Dunn, 2007; Pfeiffer et al., 2015). For example, a child with hypo-sensitivities is likely to miss information in the classroom from sensory dampening (e.g., not hearing the teacher) while a child with hyper-sensitivities (e.g., aversion to loud noise) may find the classroom a stressful environment, potentially leading to disruptive behaviour (Cheng & Boggett-Carsjens, 2005). Knowing the triggers and behavioural patterns of children with sensory sensitivities, as well as how to test for them, can enable schools to adapt (Dynia et al., 2022; Goodman-Scott & Lambert, 2015).
Measuring sensory sensitivity in children
There are a number of existing instruments to identify sensory sensitivities in children (Jorquera-Cabrera et al., 2017), each with their own strengths and limitations. The Sensory Profile 2 is one of the most commonly used questionnaires, available in a full 86-item version (Dunn, 1999, 2014) as well as a 38 item short form (Short Sensory Profile; SSP2) and is designed for parents or teachers of children from birth to 14 years (SSP2). The Sensory Profile provides scores for six sense domains (auditory, visual, touch, movement, body position, oral) and for four outcome domains (seeking, avoiding, sensitivity, registration). It has excellent psychometric properties (i.e., Cronbach’s alphas ranging 0.74 to 0.92 for the SP2, and 0.79 to 0.86 for the SSP2; Dunn et al., 2016) but also has certain limitations. As well as excluding olfactory sensitivities, the latest versions (SP2, SSP2) as with the original, do not specifically split sensitivities by hyper versus hypo domains. Another measure of childhood sensory sensitivities is the Sensory Experiences Questionnaire (Ausderau & Baranek, 2013; Baranek et al., 2006; Baranek, 2009; Little et al., 2011). Its latest edition (version 3.0) currently comprises 105 items for 2–12 year olds (Baranek, 2009) across five sense domains (auditory, visual, tactile, gustatory, and vestibular) and four outcome domains (described by the authors as Hyper, Hypo, Sensory seeking, and Enhanced perception; i.e., they use the terms hyper/hypo for over/under-sensing rather than related behaviours e.g., seeking). Whilst showing adequate psychometric properties for most scales (Cronbach’s alphas ranging 0.68 to 0.72 for subscales, 0.80 full scale: Baranek, 2009), this measure was developed specifically for sensory symptoms in children with autism or developmental disabilities so it is unclear whether it has suitability for normative populations, where internal consistency is poor (Cronbachs alpha = 0.63 for the full scale; Baranek, 2009). Finally, the Sensory Processing Measure is a questionnaire for caregivers of 5–12-year-olds (Parham et al., 2007), and comprises 62 items across five sense modalities (visual, auditory, tactile, proprioception, vestibular) and has excellent psychometric qualities (Cronbach’s alphas ranging 0.77 to 0.95 for home form subscales, 75 to 0.95 for class form subscales; Parham et al., 2007). However, the key focus of this questionnaire is tangential to sensory sensitivities per se, measuring instead sensory processing, praxis, and social participation in school. Other behavioural assessments are available, such as the Sensory Integration and Praxis Tests (Ayres, 1989), and the Sensory Processing Scale Assessments (Schoen et al., 2017). But these assessments might be considered too labour-intensive for many research situations (where sensory sensitivity can be just one aspect of assessment among many). For example, a complete Sensory Integration and Praxis Test comprises a two-hour battery, incorporating a number of different elements beyond sensory sensitivities themselves.
Given the limitations of existing sensory processing measures (primarily in the breadth of sense domains covered, the populations they are limited to, or the time requirements) we sought to produce a single comprehensive instrument that would be relatively fast and easy to administer to the parents of children from a relatively young age, for both clinical and non-clinical populations. We chose a parent report in particular (as opposed to children’s self-report) for several reasons. Firstly, although children below 8 years can reliably self-report in domains such health and well-being (Riley, 2004; Smees et al., 2019), more complex domains such as problem-behaviour or personality typically require more labour-intensive approaches for younger children (Measelle et al., 1998; Norwood, 2007; Rebok et al., 2001; Rinaldi et al., 2022; Ringoot et al., 2017). Secondly, for our measure to be valuable to children who are both typically and non-typically developing, a parent-report would be required given that conditions where sensory sensitivities arise (e.g., autism) can often present with poorer reading comprehension and/or introspection skills (Frith & Happe, 1999; Kinnaird et al., 2019; Robinson et al., 2017).
We have named our novel child measure the Parent-completed Glasgow Sensory Questionnaire (GSQ-P) because it is based on an equivalent pre-existing adult measure (the GSQ), developed previously by Robertson and Simmons (Robertson & Simmons, 2013). The original GSQ had been shown to have good validation in adults, in both neuro-typical and autistic populations, and in the UK and cross-culturally (Kuiper et al., 2018; Sapey-Triomphe et al., 2018; Ujiie & Wakabayashi, 2015), displaying excellent internal reliability for the global scale (Cronbach’s Alpha ranging 0.93 - 0.95), as well as correlating strongly with both autistic and sub-autistic traits (Horder et al., 2014; Kuiper et al., 2018; Ujiie & Wakabayashi, 2015). Here we create a version applicable to children, to be completed by their parents. Exactly like the original adult measure, our own test for parents was designed to assess hyper and hypo-sensitivity (21 items each) split equally across seven sense domains (e.g., visual, auditory, olfactory, gustatory, tactile, vestibular, proprioceptive), incorporating both sensory and behavioural dimensions (i.e., sensory overload/avoidance behaviour, as well as sensory under-responsivity/seeking behaviour). Importantly, although items from the existing adult GSQ were originally chosen to reflect knowledge within the autism literature on sensory sensitivities (Baranek et al., 2006; Robertson & Simmons, 2013) it has been successfully validated and utilised in normative adult populations. Furthermore, adult instruments have been successfully adapted to a parent-report perspective (Rinaldi et al., 2020). Our tool, therefore, took the form of an appropriate re-wording of the GSQ, to create a parent-report for describing children from both typically-developing and clinical populations.
Our new child measure, the GSQ-P, has already received a degree of validation from an earlier study, which showed our tool has concurrent validity against the Sussex Misophonia Scale for Adolescents (Simner et al., 2022). Misophonia is a type of sensory hyper-sensitivity to certain of sound (e.g., eating sounds; Jastreboff & Jastreboff, 2001). High scores on the Sussex Misophonia Scale for Adolescents significantly mapped onto high scores within our GSQ-Parent, but only for its domain of sensory hyper-sensitivity. This is exactly as we might expect since misophonia is a type of hyper- (but not hypo-) sensitivity. Here we seek additional validation for our tool by investigating its psychometric properties and convergent validity, testing the parents of a large sample of children aged 6–11 years, looking at both the general population as well as children within our sample who have learning vulnerabilities. For this latter, we used the UK schooling classification of Special Educational Needs and Disabilities (SEND). The SEND system in England and Wales is designed to provide educational support to children and young people (aged 0–25) who have additional needs, as laid out in the SEND Code of Practice 2014 (Department for Education and Department of Health, 2015) and the Children and Families Act 2014 (Department_of_Education, 2014). SEND status signifies that a child has a learning difficulty and/or a disability that requires additional support in school, and includes multiple conditions including autism, sensory impairment and mental health problems. Needs cover aspects of cognition and learning; social, emotional and mental health; communication and interaction; and sensory and/or physical needs (e.g., vision impairment). Hence this population is a heterogeneous group but is known to show meaningfully group-wise characteristics (Evangelou et al., 2008; Gaspar et al., 2016; Schwab, 2019). This classification allows us to retrieve a usable sample size and, importantly, is considered to represent a unified group not only psychologically (Wigelsworth et al., 2015) but also for educational purposes (e.g., overseen by a single co-ordinator in schools).
For our study, parents completed our novel GSQ-P, as well as measures of their a well-being, anxiety, and empathy, all known to be associated with sensory sensitivities in both adults and children; i.e., lower level of empathy, poorer well-being, and higher levels of higher anxiety (Ashburner et al., 2013; Horder et al., 2014; Robertson & Simmons, 2013). In sum, we will explore the psychometric properties of the GSQ-P, examining its factor structure, and demographic predictions. We hypothesise that our GSQ-P will be psychometrically robust, and importantly, will distinguish between typically and non-typically developing children. Secondly, we aim to examine the links between sensory sensitivities and a range of behavioural and emotional measures (specifically anxiety, behavioural difficulties, and ability to empathise). We hypothesise strong associations between all the three measures and sensory sensitivities, providing additional convergent validity for our tool. Finally, we will use our measure to explore the underlying relationship within and between hyper- and hypo-sensitivities (e.g., examining how different traits cluster). Below we describe our empirical investigation, including details of how we created the GSQ-P by adapting the corresponding adult measure to make it fitting for children.
Methods
Participants
We collected data from the parents of children involved in the multisense project, a longitudinal study funded by the European Research Council intended to investigate multisensory learning in children aged 6–11 years (Rinaldi et al., 2020, 2022; Simner et al., 2021). The original study measured how individual differences in multisensory learning correlate with differences in cognition, attainment, well-being, creativity, and so on – with one component being sensory sensitivities, for which the current instrument was originally required (and hence devised). The current paper represents its separate validation. Eligibility for the multisense project was simply attending one of 22 target schools, and there was a 99% uptake of students into the cohort. These 22 schools were state-maintained infant, junior, or primary (infant + junior) schools in the southern counties of England. To describe the representativeness of our sample, we can consider the percentage of pupils entitled to the UK benefit of Free School Meals, an indicator of socio-economic disadvantage within the school district (Taylor, 2018). Across our schools, the percentage FSM averaged at 13.4% (range 0.7 to 38.1%), where the national average from the same year is 14.5%. This suggests our sample was representative of schools country-wide in terms of socio-economic status. Additionally, across our schools, the percentage for English as a second language averaged at 13.1% (range 1.2 to 57.1%), where the national average from the same year is 18.0%.
All parents of children involved in the multisense project (n = 3690) were invited to take part in the current study, and were contacted directly after we visited children in the 22 schools. Their invitation was packaged alongside the questionnaire, and sent directly from their school (see Methods), and we offered a prize draw of £100 for all respondents. No information was given about sensory sensitivities, and no parents from this MULTISENSE project cohort were excluded from participation (i.e., we accepted all respondents). Our final cohort comprised the parents of 601 children, nearly half were girls (47%) and aged 6–11 years (M = 8.74, SD = 1.22). This sample included 32 children with SEND status (5%), 510 children who are typically developing (84%), and 62 with status unknown (10%; i.e., where parent failed to give SEND status of their child). In total, 65% of children came from households where the highest qualification was degree level or above. In addition to our n601 sample, an additional 64 parents took part but were subsequently excluded: 24 began but did not complete our questionnaire, and a further 43 were removed because they referred to a child not part of the multisense project (e.g., a sibling). In 38 cases, a parent had completed the questionnaire twice, and in these cases we took the first completed questionnaire.
Materials and procedure
Our study had ethical approval from the University of Sussex Cross-Schools Science and Technology Research Committee, and was in line with the 1964 Helsinki declaration (and amendments). Parents completed our questionnaires either via paper copy or online (via a link to Qualtrics provided in email). The choice of paper versus online was dictated simply by how each school regularly communicated with its parents, and both versions were identical in all other ways. One follow-up email was sent out to parents as a reminder to take part. Participants signed to indicate consent within a written consent document (or clicked a dedicated checkbox in the online version). The task took approximately 20 min and parents completed the following measures in the order shown below.
The Parent-completed Glasgow Sensory Questionnaire (GSQ-P)
The GSQ-P is our 42-item parent-report questionnaire, assessing sensory sensitivities in the children of respondents. Our questionnaire was adapted from the adult version of the same name (Robertson & Simmons, 2013) and details of this adaptation are given below. Half of the items addressed hyper-sensitivity and half addressed hypo-sensitivity. As in the adult version, these items were equally distributed across seven sense domains (visual, auditory, gustatory, olfactory, tactile, vestibular, proprioception) giving three questions per cell (e.g., 3 questions for visual hyper-sensitivity, 3 questions for visual hypo-sensitivity, 3 questions for auditory hyper-sensitivity, etc.). Each question had five possible responses: Never, Rarely, Sometimes, Often, Always (coded 0 to 4). The questionnaire completion does not have any specific setting requirements.
GSQ-P Instrument Development
The starting point for creating our new measure was the GSQ for adults, which was originally constructed from reports of sensory symptoms commonly associated with autism, elicited from both the literature and from the parents of autistic children (Robertson & Simmons, 2008). Its wording was developed in consultation with such parents (Robertson, 2012), as well as with autism researchers, and a consultant psychiatrist, and its clarity was ensured via piloting with a consulting group of autistic adults (Robertson, 2012). For our own parent adaptation, response categories were left unchanged (Never, Rarely, Sometimes, Often, and Always) but the prefix to the original items ‘Do you…’ was replaced with ‘Does your child…’, (with other instances of ‘you’ replaced with ‘he/she’). The original wording was retained wherever possible, although, there were three substantive changes. Two related to the distinctly adult activity of wearing perfume (e.g., “Do you enjoy wearing very strong perfumes/after-shaves?” became “Does your child seek out strong smells like perfumes, plastics, paints etc.?”). The third substantive change was for an item that would have required the parent to understand a subtle internal state in their child, which we felt would be almost impossible to know (Do you like to wear something/hold something (for example, a hat or a pencil) so that you know where your body ‘ends’?). We, therefore, used a substitute item taken from a longlist used in the development of the original GSQ (Robertson & Simmons, 2013), which had the highest factor loading for hyper-sensitivity in proprioception (i.e., the relevant category which required replacement); i.e., “Does your child turn his/her whole body (rather than only the head) when looking at something or someone?”. All other changes were minimal, involving only pronouns (you -> he/she), minor editing for brevity, or the most minor additions that would allow parents to more easily comment on their child’s feelings (e.g., “Do bright lights ever hurt your eyes…?” became “Does your child ever complain that bright lights hurt his/her eyes…?”). See Supplementary Information (SI) for full details of these changes, and see the Appendix for the complete GSQ-P questionnaire.
Strengths and Difficulties Questionnaire (SDQ)
Validated for children 5–15 years (Goodman et al., 2010), the SDQ is a 25-item emotional and behavioural screening questionnaire, incorporating five subscales: Conduct problems, Emotional symptoms, Peer problems, Hyperactivity and Prosocial behaviours (Goodman, 1997). Each item is a statement about the child over the last six months, and responses are made on a 3-point Likert scale: Not true, Somewhat true, and Certainly true (coded 0-2). For example, Item 17 relates to Prosocial behaviours and states “Kind to younger children”. A systematic review of the psychometric properties of the SDQ (Kersten et al., 2016) found good internal consistency (α = 0.73, see also Muris et al., 2003). It has been recommended that re-combining into two scales only is more robust for measuring behaviour in general populations (Goodman et al., 2010), these scales being Externalising Behaviours (combining Hyperactivity and Conduct problems) and Internalising Behaviours (combining Peer problems, Emotional symptoms), so we take this approach in our analyses below. We also tested for internal consistency for the Externalising and Internalising scales in our own sample, both of which were very good (Externalising α = 0.80; Internalising α = 0.81).
The Screen for Child Anxiety-Related Disorders (SCARED)
Validated on children aged 5–18 (Birmaher et al. 1997, 1999; Sequeira et al. 2019), the SCARED is a 41-item childhood screening questionnaire for Anxiety Disorder, with anxiety symptoms related to Panic disorder, General anxiety disorder, School avoidance, Social anxiety or Separation anxiety. Questions are presented as statements, which parents rate based on their child over the past three months. For example, Item 36 relates to school avoidance and states “My child is scared to go to school”. Parents respond on a 3-point Likert scale “Not true or hardly ever true/ Somewhat true or sometimes true/ Very true or often true”. The 41-item scale has shown excellent internal consistency (α = 0.90), and parent-child correlations for the total scale are rs = 0.32 (Birmaher et al. 1999). Internal consistency for our own sample was also excellent (α = 0.94).
Empathy Quotient (EQ-C)
Originally validated on 4–11 year olds (Auyeung et al., 2009), the Empathy Quotient for Children EQ-C (Auyeung et al., 2009) is a 27-item questionnaire, measuring children’s cognitive empathy (e.g., perspective taking) and emotional empathy (e.g., emotional response). For example, Item 11 states “My child is often rude or impolite without realising it”. Each question has four possible responses: Definitely Agree, Slightly Agree, Slightly Disagree, Definitely Disagree. These are coded, respectively, 2 1 0 0 for positively worded items reflecting high empathy (e.g., Definitely Agree would be scored 2) and are coded as 0 0 1 2 for negatively items reflecting low empathy (e.g., Definitely Agree would be scored 0). The original study (Auyeung et al., 2009) showed excellent internal consistency (α = 0.93) and our own sample also showed very good internal consistency (α = 0.87).
Demographic Questionnaire
This in-house 20-item questionnaire elicited background information such as highest parental qualification, mother’s age at child’s birth, child’s age, as well as whether the child had a SEND status. A SEND status had been established previously, either by the school alone (e.g., the school SENCO, teaching staff) or in conjunction with external professionals (e.g., educational psychologist, psychiatrist), and includes the following categories (1) learning difficulties (specific, moderate, severe, profound & multiple), (2) social, emotional and mental health, (3) speech, language and communication needs, (4) physical impairments (hearing, visual, multi-sensory), (5) physical disabilities, (6) autistic spectrum disorder, and (7) ‘other difficulties/disorders’, a category for less common cases that are not easily defined by categories 1–6. Age and SEND status (a binary category) were relevant for our current interests (and results from other factors will be published elsewhere).
Analytical Approach
In the analyses below we look first at the reliability and domain structure of the GSQ-P in isolation. The internal consistency was evaluated using Cronbach’s Alpha. Pearson’s or Spearman’s correlations were used to examine the relationship between the hyper and hypo-sensitivity domains in both the typically developing and Special Needs groups. The domain structure was investigated using Exploratory Factor Analysis (EFA), rotating the solution and allowing the factors to correlate (Oblimin rotation). The Kaiser–Meyers–Olkin measure of sampling adequacy was used to identify the amount of variance within the data that is shared by underlying factors. In light of these analyses, we next created a shortened version of our measure (i.e., a reduced form), repeating the previous EFA and assessing again the internal reliability of the reduced scale. Next, we look at the convergent validity of our scales against other measures (e.g., Goodman’s SDQ), and finally, we consider demographic differences (e.g., whether there are any differences in the sensory sensitivities of boys and girls). Throughout our analyses, we consider children as a whole but also, where relevant, as sub-groups (Typically Developing vs. SEND, and here we exclude the 62 children with status unknown). Next, we examined group differences for age and gender in sensory sensitivity scores using one-way independent sample t-tests and ANOVAs. We then investigated convergent validity with other measures (e.g., Goodman’s SDQ) using Pearson’s correlations. Finally, we carried out a hierarchical cluster analysis of sensory domain scores using Ward’s minimum variance method, using squared Euclidean distance (Yim & Ramdeen, 2015). This technique allows us to explore not only whether particular domains cluster together, but how closely they cluster. Missing responses from respondents who answered over 90% of questions were imputed with the item mean (respondents with fewer responses than this were removed). All statistical analyses were carried out using SPSS 24.0 statistical software and statistical significance was set at p < 0.05. Finally, we point out that all data was elicited from parents; hence where our results describe children, this should be taken in the context of parental-reported characteristics.
Results
GSQ-P Scale Validation, Reliability, and Factor structure
In this section, we analysed the structure of the GSQ-P overall, and its three sensitivity domains (total Sensitivity, hyper-sensitivity, hypo-sensitivity) and seven sense domains (visual, auditory, gustatory, olfactory, tactile, vestibular, proprioception; i.e., combining hyper and hypo-sensitivities for each sense). Note that we are using the terminology of ‘sense domains’ to refer to sensory channels (e.g., visual, auditory, gustatory…) and ‘sensitivity domains’ to refer to the type of sensitivity (total sensitivity, hypo- hyper-). We point out that although fourteen individual sub-domains were possible at the finest level (hyper/hypo x seven senses), these were not investigated directly unless relevant for further data reduction analyses. We also considered the internal consistency of the scale, and its factor structure.
For the sample as a whole, the relationship between total GSQ-P hyper- and hypo-sensitivity was large (i.e., they strongly correlated; r(599) = 0.78, p < 0.001). Within individual sense domains, this same relationship was less pronounced, but was generally moderate in size (see Table 1) with the weaker correlations found for vestibular, tactile, and olfactory senses. Considering now our participant sub-groups, we found that associations between the hyper and hypo domains were larger for the SEND group than children who are typically developing, particularly within individual sense domains. See also SI, which provides comparable findings from adults in two recent studies using the related adult (GSQ) scale. In other words, the evidence suggests that the pattern of associations between hyper- and hypo-scales is found for both typical and non-typical populations.
We next considered the reliability of the scale in terms of its internal consistency (i.e., the extent to which the separate questions within our scale express a single concept of sensory sensitivity). Internal consistency, measured by Cronbach’s alpha was excellent for the overall GSQ-P scale (All children α = 0.93, Typically developing α = 0.93; SEND α = 0.95), as well as for separate hyper and hypo domains (hyper-sensitivity: All children α = 0.90, Typically developing α = 0.88; SEND α = 0.93; hypo-sensitivity: All children α = 0.85, Typically developing α = 0.83; SEND α = 0.87). In terms of the sense domains, internal reliability was somewhat lower, although was “moderate” or “good” (Hair et al., 2010) in most instances (see Table 1 below; all but Tactile fell in the range of “moderate” or “good”). Similarly, the reliability remained “good” for all sense domains except tactile for the SEND group. The reliability statistics from three other adult samples can be found in the SI for comparison. The adult studies found similarly high reliability for the broader scales (overall GSQ-P, hyper-sensitivity, hypo-sensitivity) and, in line with our own findings, somewhat poorer reliability for individual sense domains. Taken together, the results suggest that the broader scales (Overall GSQ-P, hyper-sensitivity, hypo-sensitivity) form more reliable scales, but the lower reliability for sense domain scales (e.g., within the visual domain, or within the auditory domain) suggests scales scores for individual sense domains should be treated with some caution.
Factor structure of the GSQ-P
We next considered the factor structure of the GSQ-P. The factor structure of the adult GSQ has been investigated previously, and shown to load successfully as both a unitary factor based on an un-rotated Principle Components Analysis (Robertson & Simmons, 2013) and a rotated two-factor structure largely falling into hyper and hypo-sensitivities (Sapey-Triomphe et al., 2018). In other words, adults show an overall trait of sensory sensitivity as well as separate traits of hyper- and hypo-sensitivity. We, therefore, repeated a similar analysis in our child data since the factor structure may differ in younger samples. Whilst we expected to find distinct hyper and hypo sensitivity domains (i.e., two factors), we did not know a priori whether individual questionnaire items would replicate in a developmental population, especially as they now were no longer first-person report. We therefore took an exploratory approach with the expectation of one and two-factor solutions, with flexibility to also explore individual questions within the instrument for robustness.
In the current study, the Kaiser–Meyers–Olkin measure of sampling adequacy was found to be “excellent” (KMO = 0.93), indicating a high degree of potential shared variance between the 42 questionnaire items. Our Bartlett’s test of Sphericity was also excellent, χ2 (1, DF = 861) = 8767.64, p < 0.001. These results indicate that the data is suitable for factor analysis (which requires a minimum degree of shared variance between items within an instrument).
Based on our own Scree plot inspection and previous literature we performed an EFA with oblique rotation on the full 42 items, constraining extraction to two factors. The two-factor model explained 29% (26 and 3% respectively) of the variance, and the majority of items loaded on the correct hyper or hypo domain to which they were originally assigned by (Robertson & Simmons, 2013). Five items loaded on the incorrect hyper/hypo domain (Items 7, 11, 32, 37, 40) and five items did not load on either factor (<0.30; Items 3, 5, 10, 29, 38). Six of these non-complying items were proprioception questions (the entire scale): all either loading on the incorrect factor or on neither factor (<0.30, see SI for factor loadings).
In light of these issues, we created a shortened version of the GSQ-P, retaining the largest factor loadings on the correct hyper/hypo domain within each sense. The exception was proprioception, which was removed from the scale entirely. We named this new “reduced” scale the rGSQ-P and it contained 24 items (i.e., two questions for each sensitivity domain [hyper, hypo] within each sense domain [visual, auditory, olfactory, gustatory, tactile, vestibular]). We repeated the previous EFA on this reduced scale, explaining 29% (25 and 4% respectively) of the variance. All items loaded on the correct domain (see SI for full details of the factor loadings). The rGSQ-P overall hyper- and hypo- domains become more distinct, (r(599) = 0.58), and was greater for the sense domains (e.g., gustatory hyper-sensitivities now show only low correlation with gustatory hypo-sensitivities, see SI). This is to be expected given we have removed cross-loading items, and we return to this issue in the Discussion. Similar to the long GSQ-P scale, the internal reliability of the rGSQ-P scale was very good/excellent for the full scale (All children α = 0.87; Typically developing α = 0.85; SEND α = 0.91), and favourable for separate hyper and hypo domains (hyper-sensitivity All children α = 0.77; Typically developing α = 0.83; SEND α = 0.90; hypo-sensitivity All children α = 0.77; Typically developing α = 075; SEND α = 0.79). Reliability for individual sense domains was lower (ranging from 0.51–0.70, see SI), suggesting the rGSQ-P should not be used for sense domain information.
Group differences in sensory sensitivity
Above we found the long and short-form scales possessed their own strengths and issues. Although the broader scales were robust, the long from GSQ-P possessed better reliability on sense domains scales, whilst the rGSQ-P displayed a stronger factor structure. Here we now explore differences in sensory sensitivity scores across age groups, gender, and SEND classification. Our demographic comparisons utilised one-way independent sample t-tests and ANOVAs, bootstrapped where appropriate. We explored both GSQ-P and rGSQ-P (for total sensitivity, hypo-Sensitivity, hyper-sensitivity) and full statistics are found in the SI but are summarised here. No significant gender or age differences were found for either the GSQ-P or rGSQ-P. In contrast, children with a SEND status scored significantly higher on all sensitivity domains than children who are typically developing, GSQ-P: total sensitivity, t(31.759) = −6.112, p < 0.001, Bootstrapped p < 0.001, as well as hyper-sensitivity t(31.802) = −6.174, p < 0.001, Bootstrapped p < 0.001, and hypo-sensitivity t(31.915) = −5.450, p < 0.001, Bootstrapped p < 0.001; total hypo-Sensitivity, rGSQ-P: t(31.759) = −5.598, p < 0.001, Bootstrapped p < 0.001, hypo-sensitivity GSQ-P: t(538) = −5.480, p < 0.001, Bootstrapped p < 0.001, and hyper-sensitivity GSQ-P t(31.788) = −5.578, p < 0.001, Bootstrapped p < 0.001.
Convergent validity
Convergent validity was assessed by comparing the GSQ-P and rGSQ-P scores with the Empathy Quotient (EQ-C), the Strengths and Difficulties Questionnaire (SDQ), and the SCARED anxiety questionnaire using correlation statistics for children with available data on these measures. As noted earlier, anxiety is known to be associated with sensory sensitivities, in both adults and children (Ashburner et al., 2013; Ben-Sasson et al., 2009; Horder et al., 2014). We, therefore, investigated these co-morbidities using anxiety measures from both SCARED and from the appropriate scale of the SDQ (i.e., the Internalising scale, which combines Emotional symptoms and Peer problems). Both the SCARED and the Internalising scale were significantly correlated with total GSQ-P and rGSQ-P scores; higher levels of anxiety and internalising behaviours were associated with greater sensory sensitivities. The results are summarised in Table 2 (for full details see SI). Sensory sensitivity is also known to be been linked with lower levels of empathy in children (Tavassoli et al., 2018) as well as with poorer Externalising scores (i.e., poorer outward behaviour) on the Goodman’s SDQ measure (Fox et al., 2014). Here again, this was mirrored in our data: both the EQ-C questionnaire and the SDQ Externalising sub-scale were significantly associated with overall GSQ-P and rGSQ-P scores in the expected direction. These findings suggest that sensory sensitivities, as measured by the GSQ-P or rGSQ-P, show the expected associations with anxiety, empathy, and internalised/externalised wellbeing.
Next, we looked within each of the two sensitivity (hyper/hypo) domains, and found associations with EQ-C, SDQ and SCARED scales, albeit weaker than for combined scores (see Table 2 below). For both scales, poorer emotional wellbeing i.e.,.SDQ-Internalising scores and anxiety (SCARED) was more closely related to hyper-sensitivity, while poorer behaviour (i.e., SDQ-Externalising scores) more closely related to hypo-sensitivity (this latter is likely to be because the child is constantly engaging in sensory-seeking behaviour).
Investigating sensitivity clusters within hyper-sensitivity and hypo-sensitivity domains
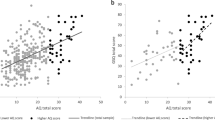
To explore how lower domains scores (e.g., visual hyper, visual hypo, etc.) clustered together within this developmental sample we replicated an earlier cluster analysis by Horder and colleagues which had been performed in adults (Horder et al., 2014). Employing hierarchical clustering of domain scores (Ward’s minimum variance method, using squared Euclidean distance, Yim & Ramdeen, 2015) on each instrument in turn (GSQ-P, rGSQ-P) we found the two factor solution was largely supported by the data. In line with our exploratory factor analysis above—the proprioception domain again was problematic in the long form, because hyper-items clustered within hypo- domains (specifically gustatory behaviours, see Fig. 1 left panel). Cluster analysis of the short form scale (rGSQ-P) revealed two distinct clusters: hyper and hypo sensitivity (see Fig. 1; right panel).

Cluster analysis of the 14 sub-domains within the GSQ-P (left panel), and 12 sub-domains within the rGSQ-P (right panel). Note: Each sub-domain is labelled by its sense (e.g., “Auditory”) and its sensitivity (“+” represents hyper-sensitivity; “−” represents hypo-sensitivity). For example, the sub-domain “Auditory+” is the domain of auditory hyper-sensitivity. Groupings represent how closely the sub-domains are linked hierarchically in our analyses. Left-hand panel shows that questions already loosely cluster into hyper- and hypo-domains in the long form of the scale, but with some exceptions (i.e., “+” elements are largely grouped together, except proprioception). The right hand panel shows a yet cleaner separation in the reduced form rGSQ-P
Within Fig. 1, our analysis a priori forces together items within the smallest cell units (e.g., we pair a priori the individual auditory hyper-sensitivity).
We also carried out a novel cluster analysis. Using the rGSQ-P to avoid the issues of cross-loading items described earlier, we entered all items from the questionnaire individually. We see in Fig. 2 the expected clustering for hyper-sensitivity (i.e., the two auditory questions cluster together; the two visual questions cluster together etc.). In contrast, we do not find this for hypo-sensitivity (which initially seem to show more arbitrary clusterings, see Fig. 1). This suggests that questions within each sense are more closely mirroring each other for hyper-sensitivity, but this is less true for hypo-sensitivity. We return to the interesting possible reasons for this in our Discussion.

Cluster analysis of the rGSQ-P. Figure shows the clear division into hyper questions (top) and hypo questions (bottom). Note: Within each sensitivity domain, questions for the same sense are labelled 1 and 2 (e.g., Gustatory 1 and Gustatory 2). Figure shows that hyper-sensitivity questions cluster by sense domain (e.g., Auditory 1 clusters with Auditory 2) but this is not true for hypo-sensitivity
Discussion
This paper evaluated the psychometric properties of our novel adaptation of the adult version of the GSQ (Robertson & Simmons, 2013) into both full and reduced short–form scales (GSQ-P, rGSQ-P). Re-designed to measure sensory sensitivities in children via parent report, the long form GSQ-P had 42 items (mirroring the adult version; Robertson & Simmons, 2013), crossing hyper- and hypo-sensitivity within each of seven sense domains (visual, auditory, gustatory, olfactory, tactile, vestibular, proprioception) giving three questions per cell. The short form (rGSQ-P) had 24 items, again crossing hyper- and hypo-sensitivity but this time with two questions only in each of six sense domains (proprioception was excluded given cross-loading in the long-form; see below). Both versions are freely available to use (presented in entirety in the Appendix), as comprehensive yet brief measures of sensory sensitivity suitable for parents reporting on younger children, and validated here on 6–11-year-olds.
The adult version has been used extensively elsewhere for research (Horder et al., 2014; Ward et al., 2018) and we here present a comparable version for children. The original adult version of the GSQ has been found elsewhere to have excellent psychometric properties and this was replicated here for the overall scale in both long and reduced forms. The suitability of both the GSQ-P and rGSQ-P for general sensory sensitivity is also evidenced by their relatively similar overall Cronbach’s alphas as well as from their similarity in convergent validity with other measures. Both showed expected empathy and well-being associations known to be co-morbid with sensory sensitivities in children (Boterberg & Warreyn, 2016; Dean et al., 2017; Green et al., 2012). Both the long and short form (GSQ-P and rGSQ-P) were unrelated to age and gender, making it a useful measure for all children across the 6–11 age group. In addition, both successfully distinguished between SEND and typically-developing populations. It may be useful in future studies where numbers of SEND children were available to investigate profiles of sensory sensitivity within specific SEND categories. The sensitivity sub-domains of both GSQ-P and rGSQ-P (total Sensitivity, hypo-sensitivity, hyper-sensitivity) also showed very good (rGSQ-P) or excellent (GSQ-P) internal consistency (i.e., collapsing across senses). Exploratory and cluster analyses of the full scale (GSQ-P) supported two main factors, which largely reflected hyper and hypo-sensitivity. As found previously in adults (Sapey-Triomphe et al., 2018), we found in children that hyper and hypo-sensitivities co-exist in the same person, but more so for some senses (vision, audition, gustation, and proprioception) than others (i.e., tactile). However, there were notable issues with individual questionnaire items due to cross-loading (and hence increasing the correlation between hyper and hypo domains) or poor factor loadings, and these ultimately led to our generating the reduced scale (rGSQ-P). Items in the proprioception modality were found to be particularly problematic and it is possible that proprioceptive items are more difficult to assess accurately from a parental perspective than sensitivities in other modalities. It should be noted that the correlation between total proprioception score (combining hyper and hypo proprioceptive sensitivities) and GSQ-P total sensitivity score (excluding proprioception) was strong (rs = 0.66) suggesting, parents are likely to notice proprioceptive sensitivities but may be misidentifying hyper and hypo responses. The removal of poorer items made hyper and hypo domains in our reduced scale more distinct (r = 0.58 compared to r = 0.78 for the full scale). By removing problematic items all hyper and hypo-sensitivity items to now load correctly. Correlation with the full 42-item scale was still extremely high (r = 0.94–0.97 for hyper-, hypo-, and total sensitivity scales). It is hoped the rGSQ-P may therefore be a useful addition to the psychometrically evaluated instruments available, especially when time is at a premium, and for future research wishing to specifically tease apart hyper- and hypo- experiences. In contrast, the long form offers the opportunity to investigate sensitivity if comparison with adult populations is required (i.e., the adult GSQ).
Cronbach’s Alphas within individual senses were somewhat poorer than for the broader domains. Specifically, when looking at gross sensitivities within any sense (e.g., collapsing across hyper- and hypo-sensitivities within vision) the long form had “acceptable” or “good” Cronbach’s alphas for all but the Tactile sense, while the short form was generally “acceptable” at best. This suggests that if scores for individual sense domains are required (e.g., visual; i.e., when collapsed over hyper- and hypo- items) the long form GSQ-P would provide the most reliable diagnostic scores. A similar pattern of lower reliability for sense domains has been found in an adult-GSQ sample (Sapey-Triomphe et al., 2018) and could be explained by a relatively small number of items per scale (Heo et al., 2015) or, alternatively, reflect the reduced utility in measuring sensitivities in this way. A possibility that needs to be explored is that hyper and hypo-sensitivities may not necessarily be constrained to the same sense modality. A child who exhibits visual hyper-sensitivity (e.g., aversion to bright lights) may have hypo-sensitivities in other domains (e.g., gustatory dampening). Hence collapsing items within any given sense may be somewhat fallacious, and could explain our low correlations between hyper/hypo questions within senses.
We also found further evidence that hyper-sensitivity may stand apart conceptually and psychologically from hypo-sensitivity. Our cluster analysis showed a more cohesive structure within hyper-sensitivities versus hypo-sensitivities (in reduced form rGSQ-P). Specifically, hyper-sensitivity questions clustered by sense modality (e.g., tactile questions grouped together; visual questions grouped together), whereas hypo-sensitivity questions did not. Instead, hypo- responses grouped by behavioural outcomes, with clusters of seeking-behaviours (e.g., seeking olfactory, tactile or auditory stimuli), clusters of sensory dampening (e.g., not feeling pain; not feeling cold), and an apparent cluster of repetitive behaviours (e.g., repetitively playing the same piece of music [auditory], spinning round and round [vestibular]). Hypo versus hyper-sensitivity may therefore spring from different mechanisms. Other differences are that hypo- outcomes are often enjoyable (Kapp et al., 2019) in contrast to hyper-sensitivities, and may help regulate sensory input and reduce stress (Liss et al., 2005; Steward, 2015). Furthermore, we found that poorer emotional well-being relates more to hyper-sensitivity [SDQ-Internalising/ Anxiety], while externalising behaviours relates more to hypo-sensitivity [SDQ-Externalising: hyperactivity, Conduct problems]. In summary, we have found a number of ways in which hyper-sensitivity stands apart from hypo-sensitivity, despite falling within the single dimension of ‘sensory sensitivities’.
In conducting our study we were aware of certain limitations. First, we acknowledge that this analysis is exploratory. Future validations using confirmatory techniques would therefore be useful. Second, as with any parent report measure, the child is not describing his/her own experiences directly. Although parent and child reports of behaviour and traits are known to converge in many ways (Powers et al., 2003; Zhou et al., 2008), their perspectives sometimes differ, for example in measures of wellbeing, behaviour, and personality – where somewhat lower associations between parent and child perspectives have been reported (Barbaranelli et al., 2003; Brown et al., 2008; Phares et al., 1989). Future work is in progress to investigate an alternative, self-report, child version of the GSQ (see Brown et al., 2021) which could allow triangulation of the data and a greater understanding of underlying sensitivities as they emerge through modes of reporting. It would also provide important insights on how the two perspectives of parent and child might differ. It would also be useful in future studies to seek test-retest reliability, and discriminant validity, for both the GSQ-P and rGSQ-P. Although sample limitations make it not possible to analyse using generalizability theory (G-theory: Brennan, 1992) we hope future studies may use these techniques to explore potential forms of variance across different type of responder (e.g., mother or father), and we might also seek to investigate measurement invariance in respect to age, ethnicity, and gender.
A strength of our paper is that we investigated sensory sensitivity in a population sample recruited from mainstream schools. It is the first study to date, as far as we are aware, to measure sensory sensitivities in children who are both typically-/non-typically developing (SEND) using six or more sense modalities and two domains of sensitivity (hyper-/ hypo-), rather than a single global measure (Ben-Sasson et al., 2008; Schoen et al., 2014). This affords potentially important novel insights. The size of our SEND sample meant we could not explore sensitivity profiles within specific sub-groups of SEND children. Future work would be highly desirable to investigate symptom presentation in a larger sample of children with specific psychological diagnoses, including for example targeted samples with autism, ADHD, anxiety disorders, intellectual disabilities, and specific learning disabilities. This type of finer focus would contribute to knowledge about the role of sensory issues in different diagnoses, and allow further validation of our questionnaire across multiple additional groups.
Finally, future studies might also compare our measure alongside existing sensory sensitivity questionnaires such as the widely used Sensory Profile 2. Given our interests in Open Science, we presented a study that could be replicated by others without cost. However, other sensory sensitivity measures are available, such as the Sensory Experiences Questionnaire or indeed the Sensory Integration and Praxis Tests which we were unable to run on our large sample of >600 children given its labour-intensity (e.g., 2 h complete test). This type of concurrent validity in future studies would be particularly important, although we remind the reader to our recent work showing concurrent validity between the rGSQ-P and the Sussex Misophonia Scale for Adolescents (Simner et al., 2022). High scores on the Sussex Misophonia Scale for Adolescents mapped onto high scores within the rGSQ-P domain of sensory hyper-sensitivity, but not hypo-sensitivities—exactly as we might expect since misophonia is a type of hyper- (but not hypo-) sensitivity. Hence our measures also shows concurrent validity against another scale of hyper-sensitivity. For convergent validity, beyond that already shown here, our rGSQ-P has now also been compared against measures of creativity (Smees et al., 2022), where our hypo-sensitivity subscale predicted higher scores on the creativity-linked trait of Openness to Experiences (Kaufman et al., 2016) and greater orientation towards creative activities involving movement and dance (exactly as we might expect from the sensory seeking aspect of the hypo-sensitivity trait). In summary, we have presented a range of ways in which our measure of childhood sensory sensitivities shows convergent validity, as well as showing convergent and concurrent validity elsewhere.
Our current study has provided a robust instrument to detect sensory sensitivities in research contexts, but it also has other potential applications. The questionnaire is quick and easy to administer so could be a useful additional tool in educational and therapeutic settings. We noted in our Introduction the many ways in which children with sensory sensitivities face challenges, for example, finding school and classroom environments particularly overwhelming (Dunn, 2007). Many typically developing children experience higher levels of sensory sensitivities (Little et al., 2017) but present with behavioural and emotional responses rather than articulating their sensory issues (Cheng & Boggett-Carsjens, 2005). Children demonstrating such difficulties may therefore benefit from a sensory sensitivity assessment so that their exact sensory profile might be understood. A similar routine assessment might be particularly beneficial for groups known to have higher sensory challenges (e.g., SEND groups, as shown here). Their sensory profile could then be written into their support plan (e.g., into their Educational, Health and Care Plan [EHCP] for schools in England where we tested). This type of application could be particularly beneficial because significant improvements are known to be found when environments are adapted for children’s sensory needs (Dynia et al., 2022). Our novel tool, completed quickly and simply by their parents, would therefore be highly valuable.
To conclude, the measures we have presented here provide robust indicators of sensory sensitivity as an overall scale, and (in the short form especially) for the separate dimension of hyper-sensitivity as distinct from hypo-sensitivity. The rGSQ-P short form would be especially useful where time is limited and shows a particularly high correspondence to the full scale, although it no longer has functionality within the proprioceptive domain. The GSQ-P long form would be more useful where comparison with adult populations is required (i.e., the adult GSQ), and allow researchers to track sensory sensitivities longitudinally. We hope this validation might enable future researcher a better understanding of the sensory sensitivities of children, especially as viewed through the eyes of their caregivers.
References
Ahn, R. R., Miller, L. J., Milberger, S., & McIntosh, D. N. (2004). Prevalence of parents’ perceptions of sensory processing disorders among kindergarten children. American Journal of Occupational Therapy, 58(3), 287–293. https://doi.org/10.5014/ajot.58.3.287.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Association.
Ashburner, J., Ziviani, J., & Rodger, S. (2008). Sensory processing and classroom emotional, behavioral, and educational outcomes in children with autism spectrum disorder. The American Journal of Occupational Therapy, 62(5), 564–573. https://doi.org/10.5014/AJOT.62.5.564.
Ashburner, J., Bennett, L., Rodger, S., & Ziviani, J. (2013). Understanding the sensory experiences of young people with autism spectrum disorder: A preliminary investigation. Australian Occupational Therapy Journal, 60(3), 171–180. https://doi.org/10.1111/1440-1630.12025.
Ausderau, K. K., & Baranek, G. T. (2013). Sensory Experiences Questionnaire. In Encyclopedia of Autism Spectrum Disorders (pp. 2770–2774). Springer New York. https://doi.org/10.1007/978-1-4419-1698-3_1192.
Auyeung, B., Wheelwright, S., Allison, C., Atkinson, M., Samarawickrema, N., & Baron-Cohen, S. (2009). The children’s Empathy Quotient and Systemizing Quotient: Sex differences in typical development and in autism spectrum conditions. Journal of Autism and Developmental Disorders, 39(11), 1509–1521. https://doi.org/10.1007/s10803-009-0772-x.
Ayres, A. J. (1989). Sensory Integration and Praxis Tests (SIPT). Western Psychological Services.
Baranek, G. T., David, F. J., Poe, M. D., Stone, W. L., & Watson, L. R. (2006). Sensory Experiences Questionnaire: discriminating sensory features in young children with autism, developmental delays, and typical development. Journal of Child Psychology and Psychiatry, 47(6), 591–601. https://doi.org/10.1111/j.1469-7610.2005.01546.x.
Baranek, G. T., Boyd, B. A., Poe, M. D., David, F. J., & Watson, L. R. (2007). Hyperresponsive sensory patterns in young children with autism, developmental delay, and typical development. American Journal of Mental Retardation, 112(4), 233–245. https://doi.org/10.1352/0895-8017(2007)112[233:HSPIYC]2.0.CO;2.
Baranek, G. T., Watson, L. R., Boyd, B. A., Poe, M. D., David, F. J., & McGuire, L. (2013). Hyporesponsiveness to social and nonsocial sensory stimuli in children with autism, children with developmental delays, and typically developing children. Development and Psychopathology, 25(2), 307–320. https://doi.org/10.1017/S0954579412001071.
Baranek, G. T. (2009). Sensory Experiences Questionnaire (Version 3.0, Unpublished manuscript)
Barbaranelli, C., Caprara, G. V., Rabasca, A., & Pastorelli, C. (2003). A questionnaire for measuring the Big Five in late childhood. Personality and Individual Differences, 34(4), 645–664. https://doi.org/10.1016/S0191-8869(02)00051-X.
Ben-Sasson, A., Carter, A. S., & Briggs-Gowan, M. J. (2010). The development of sensory over-responsivity from infancy to elementary school. Journal of Abnormal Child Psychology, 38(8), 1193–1202. https://doi.org/10.1007/s10802-010-9435-9.
Ben-Sasson, A., Hen, L., Fluss, R., Cermak, S. A., Engel-Yeger, B., & Gal, E. (2009). A meta-analysis of sensory modulation symptoms in individuals with autism spectrum disorders. Journal of Autism and Developmental Disorders, 39(1), 1–11. https://doi.org/10.1007/s10803-008-0593-3.
Ben-Sasson, Cermak, S., Orsmond, G., Tager-Flusberg, H., Kadlec, M., & Carter, A. (2008). Sensory clusters of toddlers with autism spectrum disorders: differences in affective symptoms. Journal of Child Psychology and Psychiatry, 49(8), 817–825. https://doi.org/10.1111/j.1469-7610.2008.01899.x.
Billstedt, E., Gillberg, C. I., & Gillberg, C. (2007). Autism in adults: symptom patterns and early childhood predictors. Use of the DISCO in a community sample followed from childhood. Journal of Child Psychology and Psychiatry, 48(11), 1102–1110. https://doi.org/10.1111/j.1469-7610.2007.01774.x.
Birmaher, B., Brent, D. A., Chiappetta, L., Bridge, J., Monga, S., & Baugher, M. (1999). Psychometric properties of the screen for child anxiety related emotional disorders (SCARED): A replication study. Journal of the American Academy of Child and Adolescent Psychiatry, 38(10), 1230–1236. https://doi.org/10.1097/00004583-199910000-00011.
Birmaher, B., Khetarpal, S., Cully, M., Balach, L., Kaufman, J., & Neer, S. M. (1997). The Screen for Child Anxiety Related Emotional Disorders (SCARED): Scale Construction and Psychometric Characteristics. Journal of the American Academy of Child & Adolescent Psychiatry, 36(4), 545–553. https://doi.org/10.1097/00004583-199704000-00018.
Boterberg, S., & Warreyn, P. (2016). Making sense of it all: The impact of sensory processing sensitivity on daily functioning of children. Personality and Individual Differences, 92, 80–86. https://doi.org/10.1016/J.PAID.2015.12.022.
Brennan, R. L. (1992). Generalizability theory. Educational Measurement: Issues and Practice, 11(4), 27–34. https://doi.org/10.1111/J.1745-3992.1992.TB00260.X.
Brockevelt, B. L., Nissen, R., Schweinle, W. E., Kurtz, E., & Larson, K. J. (2013). A comparison of the Sensory Profile scores of children with autism and an age- and gender-matched sample. South Dakota Medicine: The Journal of the South Dakota State Medical Association, 66, 11.
Brown, G. L., Mangelsdorf, S. C., Agathen, J. M., & Ho, M.-H. (2008). Young children’s psychological selves: Convergence with maternal reports of child personality. Social Development, 17(1), 161–182. https://doi.org/10.1111/j.1467-9507.2007.00421.x.
Brown, L., Millington, E., Robertson, A. E., & Simmons, D. (2021). Children’s Glasgow Sensory Questionnaire (C-GSQ): Validation of a Simplified and VisuallyAided Questionnaire. In Prep.
Buitendag, K., & Aronstam, M. C. (2010). The relationship between developmental dyspraxia and sensory responsivity in children aged four to eight years - Part II. In South African Journal of Occupational Therapy (Vol. 40, Issue 3). Springer US. https://doi.org/10.1007/978-1-4899-3142-9_5
Bundy, A. C., Shia, S., Qi, L., & Miller, L. J. (2007). How does sensory processing dysfunction affect play. American Journal of Occupational Therapy, 61(2), 201–208. https://doi.org/10.5014/ajot.61.2.201.
Cheng, M., & Boggett-Carsjens, J. (2005). Consider sensory processing disorders in the explosive child: case report and review. The Canadian Child and Adolescent Psychiatry Review, 14(2), 44. /pmc/articles/PMC2542921/
Cheung, P. P. P., & Siu, A. M. H. (2009). A comparison of patterns of sensory processing in children with and without developmental disabilities. Research in Developmental Disabilities, 30(6), 1468–1480. https://doi.org/10.1016/J.RIDD.2009.07.009.
Dar, R., Kahn, D. T., & Carmeli, R. (2012). The relationship between sensory processing, childhood rituals and obsessive-compulsive symptoms. Journal of Behavior Therapy and Experimental Psychiatry, 43, 679–684. https://doi.org/10.1016/j.jbtep.2011.09.008.
Davis, A. M., Bruce, A. S., Khasawneh, R., Schulz, T., Fox, C., & Dunn, W. (2013). Sensory processing issues in young children presenting to an outpatient feeding clinic. Journal of Pediatric Gastroenterology and Nutrition, 56(2), 156–160. https://doi.org/10.1097/MPG.0b013e3182736e19.
Dean, E. E., Little, L., Tomchek, S., & Dunn, W. (2017). Sensory processing in the general population: Adaptability, resiliency, and challenging behavior. American Journal of Occupational Therapy, 72(1). https://doi.org/10.5014/ajot.2018.019919
Department_of_Education. (2014). Children and Families Act.
Dunn, W. (2007). Supporting children to participate successfully in everyday life by using sensory processing knowledge. Infants and Young Children, 20(2), 84–101. https://doi.org/10.1097/01.IYC.0000264477.05076.5D.
Dunn, W., Little, L., Dean, E., Robertson, S., & Evans, B. (2016). The state of the science on sensory factors and their impact on daily life for children. OTJR: Occupation, Participation, and Health, 36(2_suppl), 3S–26S. https://doi.org/10.1177/1539449215617923.
Dunn, W. (1999). The sensory profile: Examiner’s manual.
Dunn, W. (2014). Sensory Profile 2 manual. Pearson.
Dynia, J. M., Walton, K. M., Sagester, G. M., Schmidt, E. K., & Tanner, K. J. (2022). Addressing Sensory Needs for Children With Autism Spectrum Disorder in the Classroom, 1(7), 105345122210937. https://doi.org/10.1177/10534512221093786
Engel-Yeger, B., & Dunn, W. (2011). The relationship between sensory processing difficulties and anxiety level of healthy adults. British Journal of Occupational Therapy, 74(5), 210–216. https://doi.org/10.4276/030802211X13046730116407.
Evangelou, M., Taggart, B., Sylva, K., Melhuish, E., Sammons, P., & Siraj-Blatchford, I. (2008). Effective Pre-school, Primary and Secondary Education 3–14 Project (EPPSE3–14): What Makes a Successful Transition from Primary to secondary School?
Fox, C., Snow, P. C., & Holland, K. (2014). The relationship between sensory processing difficulties and behaviour in children aged 5–9 who are at risk of developing conduct disorder. Emotional and behavioural difficulties, 19(1), 71–88. https://doi.org/10.1080/13632752.2013.854962.
Frith, U., & Happe, F. (1999). Theory of mind and self-consciousness: what is it like to be autistic? Mind and Language, 14(1), 82–89. https://doi.org/10.1111/1468-0017.00100.
Gal, E., Dyck, M. J., & Passmore, A. (2010). Relationships between stereotyped movements and sensory processing disorders in children with and without developmental or sensory disorders. American Journal of Occupational Therapy, 64(3), 453–461. https://doi.org/10.5014/ajot.2010.09075.
Gaspar, T., Bilimória, H., Albergaria, F., & Matos, M. G. (2016). Children with special education needs and subjective well-being: Social and personal influence. International Journal of Disability, Development and Education, 63(5), 500–513.
Ghanizadeh, A. (2011). Sensory processing problems in children with ADHD, a systematic review. Psychiatry Investigation, 8(2), 89 https://doi.org/10.4306/pi.2011.8.2.89.
Goodman, A., Lamping, D. L., & Ploubidis, G. B. (2010). When to use broader internalising and externalising subscales instead of the hypothesised five subscales on the Strengths and Difficulties Questionnaire (SDQ): Data from British parents, teachers, and children. Journal of Abnormal Child Psychology, 38(8), 1179–1191. https://doi.org/10.1007/s10802-010-9434-x.
Goodman, R. (1997). The Strengths and Difficulties Questionnaire: A research note. Journal of Child Psychology and Psychiatry, 38(5), 581–586. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x.
Goodman-Scott, E., & Lambert, S. F. (2015). Professional counseling for children with sensory processing disorder. Counseling & Human Services Faculty Publications, 12(2), 273–292. https://doi.org/10.15241/egs.5.2.273.
Green, S. A., Ben-Sasson, A., Soto, T. W., & Carter, A. S. (2012). Anxiety and sensory over-responsivity in toddlers with autism spectrum disorders: Bidirectional effects across time. Journal of Autism and Developmental Disorders, 42(6), 1112–1119. https://doi.org/10.1007/s10803-011-1361-3.
Hair, J. F., Black, W. C., Babin, B. J., & Anderson, R. E. (2010). Multivariate data analysis. Prentice Hall.
Heo, M., Kim, N., & Faith, M. S. (2015). Statistical power as a function of Cronbach alpha of instrument questionnaire items. BMC Medical Research Methodology, 15(1), 86 https://doi.org/10.1186/s12874-015-0070-6.
Hochhauser, M. & Engel-Yeger, B. (2010). Sensory processing abilities and their relation to participation in leisure activities among children with high-functioning autism spectrum disorder (HFASD). Research in Autism Spectrum Disorders, 4(4), 746–754. https://doi.org/10.1016/J.RASD.2010.01.015.
Horder, J., Wilson, C. E., Mendez, M. A., & Murphy, D. G. (2014). Autistic traits and abnormal sensory experiences in adults. Journal of Autism and Developmental Disorders, 44(6), 1461–1469. https://doi.org/10.1007/s10803-013-2012-7.
Isaacs, D., & Riordan, H. (2020). Sensory hypersensitivity in Tourette syndrome: A review. Brain and Development, 42(9), 627–638. https://doi.org/10.1016/J.BRAINDEV.2020.06.003.
Jastreboff, M. M., & Jastreboff, P. J. (2001). Components of decreased sound tolerance: hyperacusis, misophonia, phonophobia. ITHS News Letter, 2, 5–7.
Jorquera-Cabrera, S., Romero-Ayuso, D., Rodriguez-Gil, G., & Triviño-Juárez, J.-M. (2017). Assessment of sensory processing characteristics in children between 3 and 11 years old: A systematic review. Frontiers in Pediatrics, 5, 57 https://doi.org/10.3389/fped.2017.00057.
Kapp, S. K., Steward, R., Crane, L., Elliott, D., Elphick, C., Pellicano, E., & Russell, G. (2019). ‘People should be allowed to do what they like’: Autistic adults’ views and experiences of stimming. Autism, 23(7), 1782–1792. https://doi.org/10.1177/1362361319829628.
Kaufman, S. B., Quilty, L. C., Grazioplene, R. G., Hirsh, J. B., Gray, J. R., Peterson, J. B., & DeYoung, C. G. (2016). Openness to experience and intellect differentially predict creative achievement in the arts and aciences. Journal of Personality, 84(2), 248–258. https://doi.org/10.1111/jopy.12156.
Kersten, P., Czuba, K., McPherson, K., Dudley, M., Elder, H., Tauroa, R., & Vandal, A. (2016). A systematic review of evidence for the psychometric properties of the Strengths and Difficulties Questionnaire. International Journal of Behavioral Development, 40(1), 64–75. https://doi.org/10.1177/0165025415570647.
Kinnaird, E., Stewart, C., & Tchanturia, K. (2019). Investigating alexithymia in autism: A systematic review and meta-analysis. In European Psychiatry (Vol. 55, pp. 80–89). Elsevier Masson SAS. https://doi.org/10.1016/j.eurpsy.2018.09.004
Kuiper, M., Verhoeven, E., & Geurts, H. (2018). The Dutch Glasgow Sensory Questionnaire: Psychometric properties of an autism-specific sensory sensitivity measure. Autism, 23(4), 922–932. https://doi.org/10.1177/1362361318788065.
Lane, S. J., Reynolds, S., & Dumenci, L. (2012). Sensory over-responsivity and anxiety in typically developing children and children with autism and attention deficit hyperactivity disorder: cause or coexistence. American Journal of Occupational Therapy, 66(5), 595–603. https://doi.org/10.5014/ajot.2012.004523.
Liss, M., Timmel, L., Baxley, K., & Killingsworth, P. (2005). Sensory processing sensitivity and its relation to parental bonding, anxiety, and depression. Personality and Individual Differences, 39(8), 1429–1439. https://doi.org/10.1016/J.PAID.2005.05.007.
Little, L., Freuler, A. C., Houser, M. B., Guckian, L., Carbine, K., David, F. J., & Baranek, G. T. (2011). Psychometric validation of the sensory experiences questionnaire. American Journal of Occupational Therapy, 65(2), 207–210. https://doi.org/10.5014/ajot.2011.000844.
Little, L. M., Dean, E., Tomchek, S. D., & Dunn, W. (2017). Classifying sensory profiles of children in the general population. Child: Care, Health and Development, 43(1), 81–88. https://doi.org/10.1111/cch.12391.
McCormick, C., Hepburn, S., Young, G. S., & Rogers, S. J. (2016). Sensory symptoms in children with autism spectrum disorder, other developmental disorders and typical development: A longitudinal study. Autism, 20(5), 572–579. https://doi.org/10.1177/1362361315599755.
Measelle, J. R., Ablow, J. C., Cowan, P. A., & Cowan, C. P. (1998). Assessing young children’s views of their academic, social, and emotional lives: An evaluation of the self-perception scales of the Berkeley Puppet Interview. Child Development, 69(6), 1556–1576. https://doi.org/10.1111/j.1467-8624.1998.tb06177.x.
Muris, P., Meesters, C. & van den Berg, F. (2003). The Strengths and Difficulties Questionnaire (SDQ). European Child & Adolescent Psychiatry, 12(1), 1–8. https://doi.org/10.1007/s00787-003-0298-2.
Neil, L., Olsson, N. C., & Pellicano, E. (2016). The relationship between intolerance of uncertainty, sensory sensitivities, and anxiety in autistic and typically developing children. Journal of Autism and Developmental Disorders, 46(6), 1962–1973. https://doi.org/10.1007/S10803-016-2721-9/FIGURES/3.
Norwood, S. (2007). Validity of self-reports of psychopathology from children of 4–11 years of age. Vulnerable Children and Youth Studies, 2(2), 89–99. https://doi.org/10.1080/17450120701403136.
Panagiotidi, M., Overton, P. G., & Stafford, T. (2018). The relationship between ADHD traits and sensory sensitivity in the general population. Comprehensive Psychiatry, 80, 179–185. https://doi.org/10.1016/j.comppsych.2017.10.008.
Parham, D. L., Ecker, C., Miller-Kuhaneck, H., Henry, D. A., & Glennon, T. J. (2007). Sensory Processing Measure (SPM) manual. Western Psychological Services.
Department for Education and Department of Health. (2015). Special educational needs and disability code of practice: 0 to 25 years. Available at: https://www.gov.uk/government/publications/send-code-of-practice-0-to-25.
Pfeiffer, B., Daly, B. P., Nicholls, E. G., & Gullo, D. F. (2015). Assessing sensory processing problems in children with and without attention deficit hyperactivity disorder. Physical and Occupational Therapy in Pediatrics, 35(1), 1–12. https://doi.org/10.3109/01942638.2014.904471.
Phares, V., Compas, B. E., & Howell, D. C. (1989). Perspectives on child behavior problems: Comparisons of children’s self-reports with parent and teacher reports. Psychological Assessment: A Journal of Consulting and Clinical Psychology, 1(1), 68–71. https://doi.org/10.1037/1040-3590.1.1.68.
Powers, S. W., Patton, S. R., Hommel, K. A., & Hershey, A. D. (2003). Quality of life in childhood migraines: clinical impact and comparison to other chronic illnesses. Pediatrics, 112(1), e1–e5. https://doi.org/10.1542/peds.112.1.e1.
Rahkonen, P., Lano, A., Pesonen, A. K., Heinonen, K., Räikkönen, K., Vanhatalo, S., Autti, T., Valanne, L., Andersson, S., & Metsäranta, M. (2015). Atypical sensory processing is common in extremely low gestational age children. Acta Paediatrica, 104(5), 522–528. https://doi.org/10.1111/APA.12911.
Rebok, G., Riley, A., Forrest, C., Starfield, B., Green, B., Robertson, J., & Tambor, E. (2001). Elementary school-aged children’s reports of their health: A cognitive interviewing study. Quality of Life Research, 10(1), 59–70. https://doi.org/10.1023/A:1016693417166.
Reynolds, S., & Lane, S. J. (2009). Sensory over-responsivity and anxiety in children with ADHD. The American Journal of Occupational Therapy, 63(4), 433–440. https://doi.org/10.5014/AJOT.63.4.433.
Reynolds, S., Lane, S. J., & Thacker, L. (2011). Sensory processing, physiological stress, and sleep behaviors in children with and without autism spectrum disorders, 32(1), 246–257. https://doi.org/10.3928/15394492-20110513-02
Riley, A. W. (2004). Evidence that school-age children can self-report on their health. Ambulatory Pediatrics, 4(4), 371–376. https://doi.org/10.1367/A03-178R.1.
Rinaldi, L. J., Smees, R., Carmichael, D. A., & Simner, J. (2020). Numeracy skills in child synaesthetes: Evidence from grapheme-colour synaesthesia. Cortex, 126. https://doi.org/10.1016/j.cortex.2020.01.007
Rinaldi, L. J., Smees, R., Carmichael, D. A., & Simner, J. (2022). Big Five personality instruments for parents and children 6+ years: The pictorial BFI-10-C; the definitional BFI-44-c, and the BFI-44-parent. manuscript submitted for publication.
Ringoot, A. P., Jansen, P. W., Rijlaarsdam, J., So, P., Jaddoe, V. W. V., Verhulst, F. C., & Tiemeier, H. (2017). Self-reported problem behavior in young children with and without a DSM-disorder in the general population. European Psychiatry: The Journal of the Association of European Psychiatrists, 40, 110–115. https://doi.org/10.1016/j.eurpsy.2016.08.009.
Robertson, A. E., & Simmons, D. R. (2013). The relationship between sensory sensitivity and autistic traits in the general population. Journal of Autism and Developmental Disorders, 43(4), 775–784. https://doi.org/10.1007/s10803-012-1608-7.
Robertson, A. E. (2012). Sensory experiences of individuals with Autism Spectrum Disorder and autistic traits: a mixed methods approach. University of Glasgow.
Robertson, A. E., & Simmons, D. R. (2008). A detailed examination of the sensory sensitivities of children with autism spectrum and other developmental disorders. In Poster presented at the 2015 International Meeting for Autism Research. 14th-16th May 2008.
Robinson, S., Howlin, P., & Russell, A. (2017). Personality traits, autobiographical memory and knowledge of self and others: A comparative study in young people with autism spectrum disorder. Autism: The International Journal of Research and Practice, 21(3), 357–367. https://doi.org/10.1177/1362361316645429.
Sapey-Triomphe, L.-A., Moulin, A., Sonié, S., & Schmitz, C. (2018). The Glasgow Sensory Questionnaire: Validation of a french language version and refinement of sensory profiles of people with high Autism-Spectrum Quotient. Journal of Autism and Developmental Disorders, 48(5), 1549–1565. https://doi.org/10.1007/s10803-017-3422-8.
Schoen, S. A., Miller, L. J., & Sullivan, J. C. (2014). Measurement in sensory modulation: the Sensory Processing Scale Assessment. The American Journal of Occupational Therapy, 68(5), 522–530. https://doi.org/10.5014/ajot.2014.012377.
Schoen, S. A., Miller, L. J., & Sullivan, J. (2017). The development and psychometric properties of the Sensory Processing Scale Inventory: A report measure of sensory modulation. Journal of Intellectual & Developmental Disability, 42(1), 12–21. https://doi.org/10.3109/13668250.2016.1195490.
Schwab, S. (2019). Friendship stability among students with and without special educational needs. Educational Studies, 45(3), 390–401.
Sequeira, S. L., Silk, J. S., Woods, W. C., Kolko, D. J., & Lindhiem, O. (2019). Psychometric Properties of the SCARED in a Nationally Representative U.S. Sample of 5–12-Year-Olds. 49(6), 761–772. https://doi.org/10.1080/15374416.2019.1614001
Simner, J., Rinaldi, L. J., Koursarou, S., & Ward, J. (2022). Autistic Traits, Emotion Regulation, and Sensory Sensitivities in Children and Adults with Misophonia. Journal of Autism and Developmental Disorders, In press.
Simner, J., Smees, R., Rinaldi, L. J., & Carmichael, D. A. (2021). Wellbeing differences in children with synaesthesia: anxiety and mood regulation. Frontiers in Bioscience (Elite Edition), 13.
Smees, R., Rinaldi, L. J., & Simner, J. (2019). Well-being measures for younger children. Psychological Assessment, 32(2), 154–169. https://doi.org/10.1037/pas0000768.
Smees, R., Rinaldi, L. J., & Simner, J. (2022). What is the link between autistic traits within the general population and creativity in children? [Manuscript submitted for publication]. Department of Psychology, University of Sussex.
Smith, B., Rogers, S. L., Blissett, J., & Ludlow, A. K. (2020). The relationship between sensory sensitivity, food fussiness and food preferences in children with neurodevelopmental disorders. Appetite, 150, 104643. https://doi.org/10.1016/j.appet.2020.104643.
Steward, R. L. (2015). Repetitive stereotyped behaviour or ‘stimming’: An online survey of 100 people on the autism spectrum. In Paper presented at the 2015 International Meeting for Autism Research. 14th–16th May 2015.
Tavassoli, T., Miller, L., Schoen, S., Brout, J., Sullivan, J., & Baron-Cohen, S. (2018). Sensory reactivity, empathizing and systemizing in autism spectrum conditions and sensory processing disorder. Developmental Cognitive Neuroscience, 29, 72–77. https://doi.org/10.1016/j.dcn.2017.05.005.
Taylor, C. (2018). The reliability of Free School Meal eligibility as a measure of socio-economic disadvantage: Evidence from the millennium cohort study in Wales. British Journal of Educational Studies, 66(1), 29–51. https://doi.org/10.1080/00071005.2017.1330464.
Tomchek, S. D., Huebner, R. A., & Dunn, W. (2014). Patterns of sensory processing in children with an autism spectrum disorder. Research in Autism Spectrum Disorders, 8(9), 1214–1224. https://doi.org/10.1016/J.RASD.2014.06.006.
Ujiie, Y., & Wakabayashi, A. (2015). Psychometric properties and overlap of the GSQ and AQ among Japanese university students. International Journal of Psychological Studies, 7(2), p195 https://doi.org/10.5539/ijps.v7n2p195.
Ward, J., Brown, P., Sherwood, J., & Simner, J. (2018). An autistic-like profile of attention and perception in synaesthesia. Cortex, 107, 121–130. https://doi.org/10.1016/J.CORTEX.2017.10.008.
Watling, R. L., Deitz, J., & White, O. (2001). Comparison of Sensory Profile scores of young children with and without autism spectrum disorders. The American Journal of Occupational Therapy, 55(4), 416–423. https://doi.org/10.5014/ajot.55.4.416.
Wigelsworth, M., Oldfield, J., & Humphrey, N. (2015). Validation of the Wider Outcomes Survey for Teachers (WOST): a measure for assessing the behaviour, relationships and exposure to bullying of children and young people with special educational needs and disabilities (SEND). Journal of Research in Special Educational Needs, 15(1), 3–11. https://doi.org/10.1111/1471-3802.12030.
Yim, O., & Ramdeen, K. T. (2015). Hierarchical cluster analysis: Comparison of three linkage measures and application to psychological data. The Quantitative Methods for Psychology, 11(1), 8–21. https://doi.org/10.20982/tqmp.11.1.p008.
Yochman, A., Parush, S., & Ornoy, A. (2004). Responses of preschool children with and without ADHD to sensory events in daily life. The American Journal of Occupational Therapy, 58(3), 294–302. https://doi.org/10.5014/ajot.58.3.294.
Zhou, H., Roberts, P., & Horgan, L. (2008). Association between self‐report pain ratings of child and parent, child and nurse and parent and nurse dyads: Meta‐analysis. Journal of advanced nursing, 63(4), 334–342. https://doi.org/10.1111/j.1365-2648.2008.04694.x.
Acknowledgements
We are grateful to Mira Kaut and Gabriel McAlpine for their help in data entry. This work was supported by the European Research Council under European Union’s Seventh Framework Programme (FP/2007-2013)/ERC Grant Agreement no. [617678].
Author information
Authors and Affiliations
Contributions
R.S., J.S., and L.R. designed the study. R.S. interpreted the results, ran the data analysis, and wrote the paper. R.S. and L.R. carried out the data collection.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Ethical Approval
The study was approved by the University of Sussex Science and Technology Cross-Schools Research Ethics Committee (C-REC), and aligns with principles of the Declaration of Helsinki.
Consent to Participate
Informed consent was obtained from all participants included in this study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Appendix
Appendix
The Parent-completed Glasgow Sensory Questionnaires (short and long forms). The short form items are presented first and displayed shaded. The additional items to complete the long form are displayed afterwards and are unshaded (i.e., the full GSQ-P is the entire set of questions). Also shown are the item numbers used during our validation.
Coding sheet for the Parent-completed Glasgow Sensory Questionnaire. Shading denotes the appropriate sense domain (visual, auditory, gustatory, olfactory, tactile, vestibular, proprioceptive) and sensitivity domain (+ hyper-sensitivity; - hypo-sensitivity). Scoring: Never = 0, Rarely = 1, Sometimes = 2, Often = 3, Always = 4.
Total Sensitivity score is the sum of items across the questionnaire (range in long-form = 0–168; range in short-form = 0–96). Hyper-sensitivity score is the sum of items across the hyper-items (n21 items in the long-form; range = 0–84; n12 items in the short-form; range = 0–48). Hypo-sensitivity score is the sum of items across the hypo-items (n21 items in the long-form; range = 0–84; n12 items in the short-form; range = 0–48).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Smees, R., Rinaldi, L.J., Simmons, D.R. et al. The Parent-completed Glasgow Sensory Questionnaire: Exploring Children’s Sensory Sensitivities and Their Relationship to Well-being. J Child Fam Stud 32, 1805–1822 (2023). https://doi.org/10.1007/s10826-022-02489-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-022-02489-6