
Abstract
Background
Sport-related concussions (SRCs) affect millions of adolescents and young adults annually in the USA; however, current SRC consensus statements provide limited guidance on academic support for students within higher education.
Objective
To generate consensus on appropriate academic recommendations for clinicians, students, and academic stakeholders to support university students during their recovery.
Methods
Panelists participated in three stages of a modified Delphi procedure: the first stage included a series of open-ended questions after reviewing a literature review on post-SRC return-to-learn (RTL) in higher education; the second stage asked panelists to anonymously rate the recommendations developed through the first Delphi stage using a 9-point scale; and the final stage offered panelists the opportunity to change their responses and/or provide feedback based on the group’s overall ratings.
Results
Twenty-two panelists including clinicians, concussion researchers, and academic stakeholders (54.5% female) from 15 institutions and/or healthcare systems participated in a modified Delphi procedure. A total of 42 statements were developed after round one. Following the next two rounds, 27 statements achieved consensus amongst the panel resulting in the four-stage Post-Concussion Collegiate RTL Protocol.
Conclusion
There are several unique challenges when assisting university students back to the classroom after SRC. Explicit guidelines on when to seek additional medical care (e.g., if they are experiencing worsening or persistent symptoms) and how to approach their instructor(s) regarding academic support may help the student self-advocate. Findings from the present study address barriers and provide a framework for universities to facilitate a multidisciplinary approach amongst medical and academic stakeholders.
Similar content being viewed by others


Despite a growing interest in sport-related concussion (SRC) research, there is limited empirical support for return-to-learn (RTL) strategies. |
Current consensus recommendations for RTL may not be appropriate and/or feasible in higher education. |
The Post-Concussion Collegiate RTL Protocol provides specific recommendations to progress university students back to course-related activities after SRC. |
1 Introduction
Sport-related concussions (SRCs) are considered a serious public health concern due to their prevalence in young adult populations [1, 2] and potential long-term consequences [3]. As a result, SRC research has evolved over the past three decades to emphasize prevention [4,5,6], identification [7,8,9], and management strategies [10,11,12], with overwhelming interest in refining the graduated return-to-sport (RTS) protocol [13]. Although much focus is centered on the RTS protocol, several consensus statements emphasize the return-to-school strategies (also referred to as “return-to-learn” [RTL]) should precede final clearance for RTS [2, 14, 15]. Despite this recommendation, SRC literature has not rigorously addressed how to constructively assist students with their transition back to class or other learning environments (e.g., internships, clinical rotations, etc.) after SRC, especially in higher education.
Although a majority of SRCs resolve within a month of injury [16], the rapid pace of collegiate instruction highlights the need for universities to consider implementing a protocol to assist students who may need temporary academic supports. Indeed, university students reported the most difficulty during reading and computer-based tasks during their recovery [17], both of which are commonly assigned within higher education.
Therefore, it is critical to implement post-SRC procedures that will ensure students do not fall behind in their coursework, which may influence sports eligibility, access to financial assistance, academic performance, and/or time to graduation.
In 2016, the international Concussion in Sport Group (CISG) [18] outlined a four-step school-specific strategy to progress students from light cognitive activities (e.g., reading, screen time), through a full school day of academic instruction. These guidelines further suggest that a multidisciplinary approach (e.g., school counselor, physician, school nurse, teacher, etc.) may be the most beneficial in assisting students with their academic supports following SRC [2], especially in primary and secondary education. Additional school-related strategies have previously been outlined in the online Concussion Awareness Training Tool (CATT) for school professionals [19, 20] in order to facilitate RTL among pediatric populations; however, the guidelines proposed from the CISG and CATT may not readily translate to the coursework demands and/or learning environments of higher education.
To address post-SRC RTL in a university setting, a similar multidisciplinary model proposed by the CISG was adopted by the National Collegiate Athletics Association (NCAA) requiring member institutions to utilize a concussion management plan to address the physical and academic needs of student athletes recovering from SRC [21]. Yet, previous work investigating compliance regarding concussion management plans across the Power 5 Conferences concluded that the lowest area of compliance was with regard to RTL management strategies [22]. Specifically, medical teams indicated post-SRC academic adjustments/accommodations fell beyond their clinical competencies [22].
Notwithstanding these shortcomings, student athletes in the USA are in a unique position in terms of their access to post-SRC administrative support relative to their non-athlete student counterparts. In other words, a student athlete has access to a multidisciplinary management team to support their post-SRC needs as required by the NCAA, whereas a similar “team-based” approach is not mandated among non-athlete students. Even if multidisciplinary management is available, the knowledge of those healthcare providers relative to SRC management may be highly variable on a university campus. In contrast to students enrolled in primary and/or secondary education, university students are no longer under the direct supervision of parents/guardians, which further accentuates the need for a university-specific RTL protocol to uphold communication between academic stakeholders and medical teams to support students during their recovery.
Previous work by Hall et al. (2015) estimated that university students dedicate 36–64 h per week to academic activities [23]. Due to the rigor and rapid pace of higher education, students and faculty/staff must be educated on ways to progressively reintroduce cognitive load (i.e., gradually increasing the amount of information the working memory can retain at a given time) [23] prior to returning to a full academic schedule. Yet, without mandated SRC education, students and faculty/staff may not be aware of how SRC may negatively influence cognitive load, as well as how to adjust course-related activities to limit symptom provocation.
Overall, there is a lack of a standardized approach to assist university students with their academic supports following SRC. Therefore, the purpose of this study was to provide a universal framework regarding post-SRC RTL that may be applicable for all students in higher education using a modified Delphi technique. Ultimately, these findings may serve as a framework for future institutional policy by providing specific and inclusive pedagogical practices to support university students who require academic supports following SRC.
2 Methods
2.1 Delphi Approach
The modified Delphi technique provides working conditions to establish discussion amongst panelists in order to create policies and/or recommendations [24], and is often utilized in the development of SRC-related position statements [25, 26]. Key features of the Delphi technique include response anonymity, repeated iterations of surveys using a diverse panel, and resolution of differences to achieve the ultimate goal of consensus [27, 28].
The Delphi method is most commonly initiated using an open-ended questionnaire with supplementary materials (e.g., literature review) directly related to the subject matter [29]. Panelists’ responses are collected, analyzed, and anonymously provided to the group for each panelist to determine the importance of each item and, ultimately, achieve consensus [29].
2.2 RTL Delphi Procedure
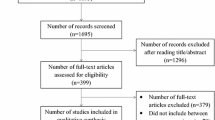
The following Delphi procedure is a part of a larger project investigating policy recommendations for students returning to academic activities after concussion in higher education [30]. Briefly, a literature review on SRC was constructed using the PubMed database between September 2020 through February 2021. The resultant document comprised 105 original research articles, consensus guidelines and/or position statements published between 1974–2020 that described the following: SRC diagnosis, recovery trends, learning disabilities in higher education, and general concussion management recommendations among adolescent and/or young adult populations. The literature review also provided information regarding post-SRC RTL strategies within primary, secondary, and post-secondary educational levels. Overall, the purpose of the literature review was to provide background information regarding RTL strategies after SRC as a preparatory step for panelists to reference while responding to the open-ended questions during the first round of the Delphi procedure (Fig. 1). Specifically, panelists were prompted by questions through an electronic survey regarding what modifications they would propose for a university-specific population based on the current return-to-school strategies from the 2016 CISG [2] as well as their own experiences assisting university-aged students recovering from concussion (Table 1).

Overview of Delphi procedure. The Delphi procedure was comprised of three total rounds (including a preparatory phase). Panelists were asked to complete an open-ended questionnaire (Round 1) resulting in 42 content statements. During Round 2, panelists rated each statement by level of importance. By Round 3, panelists had the opportunity to review their individual responses relative to the group and adjust their scores if desired. aNo change in number of statements after Round 2 (all statements rated > 3). bStatements were considered to achieve consensus if they earned a group mean score ≥ 7 after Round 3
Electronic surveys were distributed to the panelists via email and included personalized survey links (Qualtrics, Provo, UT, USA). Each survey was developed and reviewed by the research team before distribution to the panel.
Responses to open-ended questions during the first round were analyzed using directed content analysis [31] using Dedoose, a secure data management system and qualitative analysis software (www.dedoose.com; Los Angeles, CA, USA). This type of deductive approach to qualitative analysis utilizes previously established frameworks/theory as operational definitions (i.e., using four stages of the CISG guidelines) [31]. Researchers used this approach while applying the pre-determined codes to the Delphi panel’s open-ended responses in order to extend the current framework to consider university-specific modifications. During this process, two members of the research team reviewed these statements together and finalized the list of recommendations.
Results from the qualitative analysis yielded 42 original statements, which were presented to the panel during the second round. Panelists rated each of the 42 statements for level of importance on a 9-point scale [32], with “1” indicating very low importance, and “9” suggesting high importance [33, 34]. Statements with a mean score ≤ 3 were discarded [33]. After panelists completed the second round, measures of central tendency for each recommendation were calculated and anonymously presented to each panelist with their individual scores adjacent to the group’s scores for the third/final round of the Delphi procedure.
During the final round, panelists had the opportunity to compare their ratings with the group’s scores and decide whether to modify or retain their original score(s). Panelists also provided reasoning for their decision and/or additional edits/suggestions [35,36,37]. Following the final round, statements maintaining a mean score ≥ 7 [33, 38] were considered to achieve consensus. The total number of rounds and the mean score required for consensus were established a priori.
2.3 Delphi Panel
Thirty-nine individuals were invited to participate on the Delphi panel based on the following criteria: (1) experience advocating for academic needs for undergraduate students (e.g., academic counselors, instructors, deans, etc.); (2) nationally and/or internationally recognized concussion researchers; and/or (3) licensed healthcare providers with experience in the collegiate setting (e.g., neurology, psychiatry, sports medicine, primary care, neuropsychology, etc.). Prospective panelists who were unable to participate were asked to provide the study’s information to colleagues with similar expertise [39]. In all, 22 panelists completed the entire Delphi process.
This study was deemed exempt from further oversight by the University of Michigan Institutional Review Board Committee. Panelists were compensated $50 upon completion of the entire Delphi process and were provided with the opportunity to serve as co-author for prospective research abstracts and/or manuscripts from this study.
3 Results
3.1 Delphi Panel Demographics
Twenty-three panelists were originally enrolled in this study; however, one panelist dropped out before data collection began. As a result, 22 panelists (mean age 45.64 ± 11.77 years; 54.45% female) across 15 institutions and/or healthcare systems completed the full three rounds of the Delphi procedure (Table 2). The panel comprised clinicians (n = 9) with specialties in neurology, physical therapy, psychiatry, neuropsychology, primary care, and/or sports medicine/athletic training; researchers (n = 8) with expertise in education, prevention, diagnosis, and management; finally, academic stakeholders (n = 5) including advisors and tenure-track professors.
Clinicians and researchers reported a total authorship of 797 peer-reviewed, concussion-related publications, with 329 publications as first or senior author. Moreover, 31.8% of panelists are co-authors on concussion position and/or consensus statements currently used in clinical practice. Additional panelist demographics are highlighted in Table 2.
3.2 RTL Protocol Based on Delphi Consensus
Of the 42 statements, 27 (64.3%) achieved consensus amongst the Delphi panelists (Table 3). The final protocol includes six statements in Stage 1 to assist with gradual reintroduction of activities of daily living, and eight statements, respectively, in Stage 2 (increase cognitive tolerance) and Stage 3 (increase cognitive and symptom tolerance during in-class activities). In addition, there were four statements that achieved consensus in Stage 4 to facilitate a gradual decrease in academic supports to fully return to coursework, and only one out of five statements reached agreement under Additional Recommendations. The statements developed and agreed upon by the Delphi panelists (Table 3) were used to create the Post-Concussion Collegiate RTL Protocol (Table 4). Statements included in the novel RTL protocol were briefly modified by the research team for clarity and/or re-worded as a task for future use.
The goal of Stage 1 of the Post-Concussion Collegiate RTL Protocol is to support a gradual reintroduction to activities of daily living. Therefore, students are encouraged to notify their instructor(s) of potential absences, as well as follow the list of suggestions for a gradual reintroduction of activities of daily living that are specific to the university setting (e.g., socializing with friends, cooking, going to the cafeteria on campus, etc.). The objective for Stage 2 is to progressively increase cognitive tolerance. Indeed, students may reintegrate technology when completing out of class assignments or watching lectures. Students are also encouraged to discuss the possibility of additional time to complete assignments, quizzes, or tests or consider alternative options with similar outcomes. The goal for Stage 3 is to continue to increase cognitive and symptom tolerance while engaging in in-class activities. Therefore, students may opt to attend in-class activities through the use of academic support such as notetakers, lecture audio recordings, printouts of lectures, and/or use of sunglasses, blue light blocking glasses or by turning off their computer screens during hybrid learning. By Stage 4, students should be gradually weaning away from academic supports to attend a full week of class within their learning environment(s). Similar to the 2016 CISG school-specific strategies, there are no definitive timeframes for progressing through each phase due to the individuality of SRC recovery. If a student’s symptoms are worsening at any point in the protocol, they are encouraged to either return to the previous stage or communicate with their instructor(s) on how to further modify course-related activities. Most notably, the Post-Concussion Collegiate RTL Protocol encourages students to uphold communication with their academic support group, whether that is their academic advisor, instructor(s), disability services representative, and/or any other individual who facilitates their academic progress.
4 Discussion
Although SRC research has significantly evolved over the previous decade, emphasis has been placed on injury assessment, management, and RTS. However, there continues to be a lack of evidence-based guidance around returning student athletes and non-athlete students to the classroom across all educational levels. Specifically, management strategies to address academic needs after SRC within higher education remain relatively scarce in medical literature. Therefore, the statements that achieved consensus among the Delphi panelists built upon the guidelines proposed in the current RTL protocol [2] to specifically support a collaborative approach to managing university students recovering from SRC.
The Post-Concussion Collegiate RTL Protocol serves as a resource for academic stakeholders to reference in order to support students who require a gradual progression when returning to their typical academic workload [23]. University students have previously identified numerous academic challenges following SRC including computer-based tasks and reading [17], whereas others reported difficulty with math-based coursework [40]. In order to address the heterogeneity of SRC and its management, the Post-Concussion Collegiate RTL Protocol may be used as a gateway to uphold communication between clinicians, students, and academic stakeholders to support the individualized needs of university students during their recovery. The proposed protocol builds upon the 4-step return-to-school strategy outlined by the 2016 CISG [2], beginning with light cognitive activities and progressing to a full week of in-person classes with university-specific considerations for academic stakeholders or students to modify based on their coursework and/or learning environments.
Further, the legal obligation of universities to support students recovering from SRC is unclear. The Americans with Disability Act (ADA) of 1990 defines disability as a mental or physical impairment that limits major life activities (e.g., school, employment, etc.) [41] and under this definition, SRC may be considered as a temporary disability. Yet, university students with disabilities have previously reported stigma [42] and lack of cooperation from faculty/staff who may question the authenticity of the student’s disability status [43]. The attitudes and behaviors of university faculty/staff may be due to societal biases, time constraints, and/or insufficient training on accommodating students with disabilities [44]. Indeed, many universities in the USA utilize Offices for Disability Services as a method to facilitate this procedure; however, processing this documentation may extend beyond the typical SRC recovery timeline [16]. Therefore, the proposed Post-Concussion Collegiate Protocol provides guided suggestions for faculty/staff to consider implementing during the first few weeks of recovery to facilitate collaboration between the students and their academic teams. Additional research is necessary to further investigate the processes by which students recovering from SRC obtain academic supports in the university setting.
To date, the body of RTL research has focused on primary and secondary education students [45, 46]. At these educational levels, students are often supervised by parents, pediatricians, school nurses, principals, teachers, and/or school psychologists [47] with direct oversight of their medical care as educational safeguards [48]. In higher education, the use of a multidisciplinary approach is required by the NCAA for all student athletes recovering from SRC [21]; however, there is no such management model among non-athlete students. Therefore, the proposed Post-Concussion Collegiate RTL Protocol goes well above the current NCAA post-SRC guidelines, as well as provides direction on how to achieve a multidisciplinary approach to support RTL among all university students. Further, the processes outlined in the Post-Concussion Collegiate RTL Protocol may serve to facilitate a discussion between the student and instructor(s) on appropriate adjustments to their coursework and learning environments. These findings may also promote collaboration among students, their medical providers and/or coaches to determine appropriate post-SRC progressions in non-academic learning environments, such as watching film or engaging in team meetings.
Moreover, university instructors maintain a pivotal role in student academic success, especially among students recovering from SRC. Recent research conducted by Bevilacqua et al. (2021) sought to unveil common perspectives regarding collegiate RTL and classroom management following concussion [49]. Ninety-five percent of instructors indicated they wished to be a part of a “RTL Team,” a task easily accomplished with academic support requiring no additional demand on the instructor (e.g., wearing sunglasses in class, additional time for assignments/exams, etc.) [49]. The Post-Concussion Collegiate RTL Protocol supports this demand for academic stakeholders to take a lead role in initiating and facilitating an appropriate progression for students returning to their respective learning environments, as these may differ among courses. In addition, several academic supports outlined in the Post-Concussion Collegiate RTL Protocol complement the work by Bevilacqua et al. including limiting computer use, utilizing paper handouts, taking rest breaks, and reducing screen brightness [50]. Researchers hypothesized implementation of academic supports may be inversely related to its time commitment [51], which may be particularly relevant for university instructors who teach hundreds of students per semester. Importantly, these recommendations may also support academic stakeholders at the university level who do not receive SRC education and/or training, by providing specific examples of how to adjust their learning environments and/or coursework. Overall, there is a strong need for a standardized approach for students to obtain academic support across disciplines and departments in order to decrease the burden on instructors and students.
Despite the novelty of these findings, the Post-Concussion Collegiate RTL Protocol is only a preliminary step in addressing larger-scale issues related to academic support within institutions of higher education. Future clinical implications and/or use of this protocol must consider the complex intersection of student identity (race, ethnicity, socioeconomic status, sexual orientation, etc.) at the university level, that may inherently influence a student’s likelihood of seeking academic supports, irrespective of injury. In general, current RTL literature has not sufficiently addressed the specific processes by which students obtain academic supports within post-secondary educational settings. Despite several initiatives to provide pedagogical training in diversity, equity, and inclusion, university instructors may subconsciously demonstrate explicit biases [51], which may influence a student’s initiative to seek academic supports. Specifically, universities strive to provide equitable opportunities for historically minoritized groups (e.g., first-generation, students with [dis]abilities, Black/Indigenous/Students of Color, Hispanic and/or Latinx, gender diversities and/or LGBTQAI + , etc.); however, future investigations should seek to address how social identity may influence the processes by which students obtain academic supports following SRC, as well as its impact on future protocol implementation.
This study is not without limitations. It was difficult to recruit academic stakeholders in contrast to clinicians and researchers, and as a result, the final sample was unevenly distributed (skewed toward clinician and researcher perspectives), which may bias the results. These findings may also be more representative of the perspectives of athletic trainers than clinicians and researchers from other disciplines. In addition, the Post-Concussion Collegiate RTL Protocol may not be appropriate for all disciplines/curricula; however, it may serve as a universal framework for instructors to utilize when assisting students with their RTL progressions. For example, guidelines for students in courses or laboratories requiring physical exertion with audio, visual, and/or vestibular stimuli (e.g., Performing Arts, Chemistry, Movement Science, etc.) will require additional considerations. Further, 82% of the Delphi panel self-identified as White and non-Hispanic and/or Latinx. Although the panel’s demographics are representative of predominantly White institutions [51], the present findings may not be generalizable to minority serving institutions. Lastly, although the Delphi technique is a validated procedure [52] used to obtain expert opinion across disciplines, it is only one method of developing consensus. Despite these limitations, the results from the present study provide medical and academic stakeholders with a general framework to build upon when assisting students with their specific academic needs during their RTL progression in post-secondary education. Future research should assess the infrastructure, resources, and local implementation strategies of the Post-Concussion Collegiate RTL Protocol among academic stakeholders and university students returning to class after SRC.
5 Conclusions
This is the first study to employ a modified Delphi approach with a multidisciplinary panel to develop consensus recommendations on appropriate academic support for university-aged students recovering from SRC. The resultant Post-Concussion Collegiate RTL Protocol emphasizes the processes of creating and maintaining a multidisciplinary approach to facilitate recovery within higher education. It should be emphasized that SRC management must be individualized in order to appropriately address each student’s unique clinical presentations. Although this is the first step towards promoting collaboration among students and academic stakeholders regarding course-specific RTL strategies, future research must consider how student identity influences the likelihood of seeking academic supports after concussion.
References
Zemek RL, Farion KJ, Sampson M, McGahern C. Prognosticators of persistent symptoms following pediatric concussion: a systematic review. JAMA Pediatr. 2013;167(3):259–65.
McCrory P, Meeuwisse W, Dvorak J, Aubry M, Bailes J, Broglio S, et al. Consensus statement on concussion in sport—the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med. 2017;51(11):838–47.
Control CfD, Prevention. Report to Congress on mild traumatic brain injury in the United States: steps to prevent a serious public health problem. Atlanta, GA: Centers for Disease Control and Prevention. 2003;45.
Collins MW, Kontos AP, Reynolds E, Murawski CD, Fu FH. A comprehensive, targeted approach to the clinical care of athletes following sport-related concussion. Knee Surg Sports Traumatol Arthrosc. 2014;22(2):235–46.
Maas AIR, Menon DK, Adelson PD, Andelic N, Bell MJ, Belli A, et al. Traumatic brain injury: integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017;16(12):987–1048.
Eckner JT, Oh YK, Joshi MS, Richardson JK, Ashton-Miller JA. Effect of neck muscle strength and anticipatory cervical muscle activation on the kinematic response of the head to impulsive loads. Am J Sports Med. 2014;42(3):566–76.
Broglio SP, Katz BP, Zhao S, McCrea M, McAllister T, Investigators CC. Test-retest reliability and interpretation of common concussion assessment tools: findings from the NCAA-DoD CARE Consortium. Sports Med. 2018;48(5):1255–68.
McCrea M, Kelly JP, Randolph C, Kluge J, Bartolic E, Finn G, et al. Standardized assessment of concussion (SAC): on-site mental status evaluation of the athlete. J Head Trauma Rehabil. 1998;13(2):27–35.
McCrea M, Randolph C, Kelly J. Standardized Assessment of Concussion (SAC): manual for administration, scoring and interpretation. Waukesha: CNS. Inc.; 2000. (Google Scholar).
Alsalaheen BA, Mucha A, Morris LO, Whitney SL, Furman JM, Camiolo-Reddy CE, et al. Vestibular rehabilitation for dizziness and balance disorders after concussion. J Neurol Phys Ther. 2010;34(2):87–93.
Leddy JJ, Haider MN, Ellis MJ, Mannix R, Darling SR, Freitas MS, et al. Early subthreshold aerobic exercise for sport-related concussion: a randomized clinical trial. JAMA Pediatr. 2019;173(4):319–25.
Leddy JJ, Haider MN, Ellis M, Willer BS. Exercise is medicine for concussion. Curr Sports Med Rep. 2018;17(8):262–70.
Aubry M, Cantu R, Dvorak J, Graf-Baumann T, Johnston K, Kelly J, et al. Summary and agreement statement of the first International Conference on Concussion in Sport, Vienna 2001. Br J Sports Med. 2002;36(1):6–7.
Herring S, Kibler WB, Putukian M, Solomon GS, Boyajian-O'Neill L, Dec KL, Franks RR, Indelicato PA, LaBella CR, Leddy JJ, Matuszak J, McDonough EB, O'Connor F, Sutton KM. Selected issues in sport-related concussion (SRC|mild traumatic brain injury) for the team physician: a consensus statement. Br J Sports Med. 2021;55(22):1251–61. https://doi.org/10.1136/bjsports-2021-104235.
Harmon KG, Clugston JR, Dec K, Hainline B, Herring S, Kane SF, et al. American Medical Society for Sports Medicine position statement on concussion in sport. Br J Sports Med. 2019;53(4):213.
Broglio SP, McAllister T, Katz BP, LaPradd M, Zhou W, McCrea MA; CARE Consortium Investigators. The Natural History of Sport-Related Concussion in Collegiate Athletes: Findings from the NCAA-DoD CARE Consortium. Sports Med. 2022;52(2):403–15. https://doi.org/10.1007/s40279-021-01541-7.
Holmes A, Chen Z, Yahng L, Fletcher D, Kawata K. Return to Learn: Academic Effects of Concussion in High School and College Student-Athletes. Front Pediatr. 2020;4(8):57. https://doi.org/10.3389/fped.2020.00057.
McCrory P, Meeuwisse W, Johnston K, Dvorak J, Aubry M, Molloy M, et al. Consensus statement on Concussion in Sport–the 3rd International Conference on Concussion in Sport held in Zurich, November 2008. S Afr J Sports Med. 2009;21(2):185–200.
Babul S, Pike I. The online concussion awareness training tool (catt). Br J Sports Med. 2017;51(11):A72-A.
Damji F, Babul S. Improving and standardizing concussion education and care: a Canadian experience. Concussion. 2018;3(4):CNC58.
National Collegiate Athletic Association 2014–15 Sports Medicine Handbook 2015. http://www.ncaa.org/sport-science-institute/2014-15-ncaa-sports-medicine-handbook. Accessed Oct 2021.
Buckley TA, Baugh CM, Meehan WP, Difabio MS. Concussion management plan compliance: a study of NCAA Power 5 Conference Schools. Orthop J Sports Med. 2017;5(4):232596711770260.
Hall EE, Ketcham CJ, Crenshaw CR, Baker MH, McConnell JM, Patel K. Concussion management in collegiate student-athletes: return-to-academics recommendations. Clin J Sport Med. 2015;25(3):291–6.
Gupta A, Summerville G, Senter C. Treatment of acute sports-related concussion. Curr Rev Musculoskelet Med. 2019;12(2):117–23.
Giza CC, Kutcher JS, Ashwal S, Barth J, Getchius TS, Gioia GA, et al. Summary of evidence-based guideline update: evaluation and management of concussion in sports: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80(24):2250–7.
Rivara FP, Tennyson R, Mills B, Browd SR, Emery CA, Gioia G, et al. Consensus statement on sports-related concussions in youth sports using a modified Delphi approach. JAMA Pediatr. 2020;174(1):79.
Gupta UG, Clarke RE. Theory and applications of the Delphi technique: a bibliography (1975–1994). Technol Forecast Soc Chang. 1996;53(2):185–211.
Guzys D, Dickson-Swift V, Kenny A, Threlkeld G. Gadamerian philosophical hermeneutics as a useful methodological framework for the Delphi technique. Int J Qual Stud Health Well Being. 2015;10(1):26291.
Linstone HA, Turoff M. Introduction to the Delphi method: techniques and applications. Reading: Addison-Wesley Publishing Company; 1975. p. 9.
Memmini AK, Popovich MJ, Schuyten KH, Herring SA, Scott KL, Clugston JR, et al. Recommendations for medical discharge documentation and academic supports for university students recovering from concussion. J Head Trauma Rehabil (in press).
Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–88.
Stitt-Gohdes WL, Crews TB. The Delphi technique: a research strategy for career and technical education. J Career Tech Educ. 2004;20:55–67.
Kroshus E, Chrisman SPD, Harmon KG, Herring SA, Broglio SP, Master CL, et al. What do parents need to know about concussion? Developing consensus using the Delphi method. Clin J Sport Med. 2018;1.
Boulkedid R, Abdoul H, Loustau M, Sibony O, Alberti C. Using and reporting the Delphi method for selecting healthcare quality indicators: a systematic review. PLoS ONE. 2011;6(6): e20476.
Ludwig B. Predicting the future: Have you considered using the Delphi methodology. J Ext. 1997;35(5):1–4.
Hsu C-C, Sandford B. The Delphi Technique: making sense of consensus. In: Practical assessment, research and evaluation. 2007;12.
Hyslop-Margison EJ, Armstrong J. The Delphi technique: a research strategy for career and technical education. J Career Tech Educ. 2004;21(1).
Zumsteg JM, Ennis SK, Jaffe KM, Mangione-Smith R, MacKenzie EJ, Rivara FP. Quality of care indicators for the structure and organization of inpatient rehabilitation care of children with traumatic brain injury. Arch Phys Med Rehabil. 2012;93(3):386-93.e1.
Streeton R, Cooke M, Campbell J. Researching the researchers: using a snowballing technique. Nurse Res. 2004;12(1):35–47.
Bevilacqua ZW, Kerby ME, Fletcher D, Chen Z, Merritt B, Huibregtse ME, et al. Preliminary evidence-based recommendations for return to learn: a novel pilot study tracking concussed college students. Concussion. 2019;4(2):CNC3.
Americans with Disabilities Act of 1990. Pub. L. No. 101–336, 42 U.S.C. 12111, 12112. (1990).
Magnus E, Tøssebro J. Negotiating individual accommodation in higher education. Scand J Disabil Res. 2014;16(4):316–32.
Hong BS, Himmel J. Faculty attitudes and perceptions toward college students with disabilities. Coll Q. 2009;12(3):678–84.
Smith SA, Woodhead E, Chin-Newman C. Disclosing accommodation needs: exploring experiences of higher education students with disabilities. Int J Incl Educ. 2021;25(12):1358–74.
O’Neill JA, Cox MK, Clay OJ, Johnston JM Jr, Novack TA, Schwebel DC, et al. A review of the literature on pediatric concussions and return-to-learn (RTL): implications for RTL policy, research, and practice. Rehabil Psychol. 2017;62(3):300–23.
Master CL, Gioia GA, Leddy JJ, Grady MF. Importance of “return-to-learn” in pediatric and adolescent concussion. Pediatr Ann. 2012;41(9):1–6.
McAvoy K, Eagan-Johnson B, Halstead M. Return to learn: Transitioning to school and through ascending levels of academic support for students following a concussion. NeuroRehabilitation. 2018;42(3):325–30.
McAvoy K, Eagan-Johnson B, Dymacek R, Hooper S, McCart M, Tyler J. Establishing Consensus for Essential Elements in Returning to Learn Following a Concussion. J Sch Health. 2020;90(11):849–58.
Bevilacqua Z, Cothran DJ, Rettke DJ, Koceja DM, Nelson-Laird TF, Kawata K. Educator perspectives on concussion management in the college classroom: a grounded theory introduction to collegiate return-to-learn. BMJ Open. 2021;11(4): e044487.
Dee T, Gershenson S. Unconscious Bias in the Classroom: Evidence and Opportunities, 2017. Stanford Center for Education Policy Analysis. 2017. https://cepa.stanford.edu/content/unconscious-biasclassroom-evidence-and-opportunities. Accessed Oct 2021 .
Race/Ethnicity of College Faculty (2018): National Center for Education Statistics. https://nces.ed.gov/fastfacts/display.asp?id=61. Accessed Oct 2021.
Landeta J. Current validity of the Delphi method in social sciences. Technol Forecast Soc Change. 2006;73:467–82.
Acknowledgements
The authors would like to extend a note of gratitude to Drs. Annemarie Palincsar and Donald Freeman from the University of Michigan School of Education for their contributions to the study design and qualitative analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing Interests
Dr. Steven Broglio has current or previous research funding from the National Institutes of Health, Centers for Disease Control and Prevention, and Department of Defense (U.S.A. Medical Research Acquisition Activity), National Collegiate Athletic Association, National Athletic Trainers’ Association Foundation, National Football League/Under Armour/GE, Simbex, and ElmindA; is a co-author of Biomechanics of Injury (3rd edition, Human Kinetics); serves as a consultant for U.S. Soccer (paid), U.S. Cycling (unpaid), medico-legal litigation; received speaker honorarium and travel reimbursements for his research presentations; and has a patent pending on “Brain Metabolism Monitoring Through CCO Measurements Using All-Fiber-Integrated Super-Continuum Source” (U.S. Application No. 17/164,490). Under Dr. Steven Broglio’s direction, Dr. Allyssa Memmini has secured funding from the University of Michigan Rackham Graduate Research Grant. Dr. Meeryo Choe serves as a speaker for pediatric grand rounds and consultant for medico-legal litigation. Dr. Anthony Kontos receives royalties from APA Books and support for research to the University of Pittsburgh from the National Football League. Dr. Johna Register Mihalik received research funding to The University of North Carolina-Chapel Hill in the past three years from the National Football League, Department of Defense, Centers for Disease Control and Prevention, National Athletic Trainers’ Association Foundation, and the NCAA-DoD Mind Matters Research Challenge, as well as previously served on USA Football’s Football Development Council. All Delphi panelists received $50 as an incentive for their participation in this study.
Funding
This study was funded by the University of Michigan Rackham Graduate Student Research Grant.
Author Contributions
Allyssa Memmini, Steven Broglio, Rebecca Hasson, and Sami Rifat contributed to the study conception and design. Material preparation, data collection, and analysis were conducted by Allyssa Memmini and Steven Broglio. Delphi panelists (Michael Popovich, Kristen Schuyten, Stanley Herring, Katie Scott, James Clugston, Meeryo Choe, Christopher Bailey, Alison Brooks, Scott Anderson, Michael McCrea, Anthony Kontos, Jessica Wallace, Johna Register-Mihalik, Tricia Kasamatsu, Tamara Valovich McLeod, Michelle Weber Rawlins, Traci Snedden, Michael Kaplan, Briana Akani, La’Joya Orr) wrote the original statements included in this study. The first draft of the manuscript was written by Allyssa Memmini and all authors commented on subsequent versions of the manuscript. All authors read and approved the final manuscript.
Availability of Data and Material
Data collection and analysis for the present study may be made available from the corresponding author on reasonable request until the end of 2023.
Ethics Approval
All study procedures were reviewed by the University of Michigan Institutional Review Board and deemed exempt. This study was conducted in accordance with the 1964 Declaration of Helsinki including its later amendments and comparable ethical standards.
Consent to Participate
Participants provided written informed consent prior to participation.
Rights and permissions
About this article

Cite this article
Memmini, A.K., Popovich, M.J., Schuyten, K.H. et al. Achieving Consensus Through a Modified Delphi Technique to Create the Post-concussion Collegiate Return-to-Learn Protocol. Sports Med 53, 903–916 (2023). https://doi.org/10.1007/s40279-022-01788-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-022-01788-8