
Determination of the Elution Capacity of Dalbavancin in Bone Cements: New Alternative for the Treatment of Biofilm-Related Peri-Prosthetic Joint Infections Based on an In Vitro Study

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Preparation of the Antibiotic-Loaded Bone Cements
4.2. Vancomycin Analysis
4.3. Dalbavancin Analysis
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lum, Z.C.; Holland, C.T.; Meehan, J.P. Systematic review of single stage revision for prosthetic joint infection. World J. Orthop. 2020, 11, 559–572. [Google Scholar] [CrossRef] [PubMed]
- Kunutsor, S.K.; Beswick, A.D.; Peters, T.J.; Gooberman-Hill, R.; Whitehouse, M.R.; Blom, A.W.; Moore, A.J. Health care needs and support for patients undergoing treatment for prosthetic joint infection following hip or knee arthroplasty: A systematic review. PLoS ONE 2017, 12, e0169068. [Google Scholar] [CrossRef] [PubMed]
- Minassian, A.M.; Osmon, U.R.; Berendt, A.R. Clinical guidelines in the management of prosthetic joint infection. J. Antimicrob. Chemother. 2014, 69 (Suppl. 1), i29–i35. [Google Scholar] [CrossRef]
- Ariza, J.; Cobo, J.; Baraia-Etxaburu, J.; de Benito, N.; Bori, G.; Cabo, J.; Corona, P.; Esteban, J.; Horcajada, J.P.; Lora-Tamayo, J.; et al. Executive summary of management of prosthetic joint infections. Clinical practice guidelines by the Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC). Enferm. Infecc. Y Microbiol. Clin. 2017, 35, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Berberich, C.; Sanz-Ruiz, P. Risk assessment of antibiotic resistance development by antibiotic-loaded bone cements: Is it a clinical concern? EFORT Open Rev. 2019, 4, 576–584. [Google Scholar] [CrossRef] [PubMed]
- López-Torres, I.I.; Sanz-Ruíz, P.; Navarro-García, F.; León-Román, V.E.; Vaquero-Martín, J. Experimental reproduction of periprosthetic joint infection: Developing a representative animal model. Knee 2020, 27, 1106–1112. [Google Scholar] [CrossRef] [PubMed]
- Nau, C.; Seebach, C.; Trumm, A.; Schaible, A.; Kontradowitz, K.; Meier, S.; Buechner, H.; Marzi, I.; Henrich, D. Alteration of Masquelet’s induced membrane characteristics by different kinds of antibiotic enriched bone cement in a critical size defect model in the rat’s femur. Injury 2016, 47, 325–334. [Google Scholar] [CrossRef]
- Paz, E.; Sanz-Ruiz, P.; Abenojar, J.; Vaquero-Martín, J.; Forriol, F.; Del Real, J.C. Evaluation of elution and mechanical properties of high-dose antibiotic-loaded bone cement: Comparative “in vitro” study of the influence of vancomycin and cefazolin. J. Arthroplast. 2015, 30, 1423–1429. [Google Scholar] [CrossRef]
- Sanz-Ruiz, P.; Calvo-Haro, J.A.; Villanueva-Martinez, M.; Matas-Diez, J.A.; Vaquero-Martín, J. Biarticular total femur spacer for massive femoral bone loss: The mobile solution for a big problem. Arthroplast. Today 2018, 4, 58–64. [Google Scholar] [CrossRef]
- Sanz-Ruiz, P.; Carbó-Laso, E.; del Real, J.C.; Arán-Ais, F.; Iglesias, Y.B.; Paz, E.; Sánchez-Navarro, M.; Pérez-Limiñana, M.; Vaquero-Martín, J. Microencapsulation of rifampicin: A technique to preserve the mechanical properties of bone cement. J. Orthop. Res. 2018, 36, 459–466. [Google Scholar]
- Sanz-Ruiz, P.; Matas-Diez, J.A.; Villanueva-Martinez, M.; Carbo-Laso, E.; Lopez-Torres, I.I.; Vaquero-Martín, J. A new biarticular cement spacer technique for infected total hip and knee arthroplasty with massive bone loss. HIP Int. 2021, 31, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Ruiz, P.; Paz, E.; Abenojar, J.; del Real, J.C.; Vaquero, J.; Forriol, F. Effects of vancomycin, cefazolin and test conditions on the wear behavior of bone cement. J. Arthroplast. 2014, 29, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Aho, O.-M.; Lehenkari, P.; Ristiniemi, J.; Lehtonen, S.; Risteli, J.; Leskelä, H.-V. The mechanism of action of induced membranes in bone repair. J. Bone Jt. Surg. 2013, 95, 597–604. [Google Scholar] [CrossRef]
- Giannoudis, P.V.; Harwood, P.J.; Tosounidis, T.; Kanakaris, N.K. Restoration of long bone defects treated with the induced membrane technique: Protocol and outcomes. Injury 2016, 47 (Suppl. 6), S53–S61. [Google Scholar] [CrossRef]
- Henrich, D.; Seebach, C.; Nau, C.; Basan, S.; Relja, B.; Wilhelm, K.; Schaible, A.; Frank, J.; Barker, J.; Marzi, I. Establishment and characterization of the Masquelet induced membrane technique in a rat femur critical-sized defect model. J. Tissue Eng. Regen. Med. 2016, 10, E382–E396. [Google Scholar] [CrossRef]
- Ikeda, S.; Uchiyama, K.; Minegishi, Y.; Ohno, K.; Nakamura, M.; Yoshida, K.; Fukushima, K.; Takahira, N.; Takaso, M. Double-layered antibiotic-loaded cement spacer as a novel alternative for managing periprosthetic joint infection: An in vitro study. J. Orthop. Surg. Res. 2018, 13, 322. [Google Scholar] [CrossRef] [PubMed]
- Saravolatz, L.D.; Billeter, M.; Zervos, M.J.; Chen, A.Y.; Dalovisio, J.R.; Kurukularatne, C. Dalbavancin: A novel once-weekly lipoglycopeptide antibiotic. Clin. Infect. Dis. 2008, 46, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Cercenado, E. Antimicrobial spectrum of dalbavancin. Mechanism of action and in vitro activity against gram-positive microorganisms. Enferm. Infecc. Microbiol. Clin. 2017, 35 (Suppl. 1), 9–14. [Google Scholar] [CrossRef]
- Di Pilato, V.; Ceccherini, F.; Sennati, S.; D’Agostino, F.; Arena, F.; D’Atanasio, N.; Di Giorgio, F.P.; Tongiani, S.; Pallecchi, L.; Rossolini, G.M. In vitro time-kill kinetics of dalbavancin against Staphylococcus spp. biofilms over prolonged exposure times. Diagn. Microbiol. Infect. Dis. 2020, 96, 114901. [Google Scholar] [CrossRef]
- Díaz-Ruíz, C.; Alonso, B.; Cercenado, E.; Cruces, R.; Bouza, E.; Muñoz, P.; Guembe, M. Can dalbavancin be used as a catheter lock solution? Antimicrob. Agents Chemother. 2018, 67, 936–944. [Google Scholar] [CrossRef]
- Sivori, F.; Cavallo, I.; Kovacs, D.; Guembe, M.; Sperduti, I.; Truglio, M.; Pasqua, M.; Prignano, G.; Mastrofrancesco, A.; Toma, L.; et al. Role of extracellular DNA in dalbavancin activity against methicillin-resistant staphylococcus aureus (MRSA) biofilms in patients with skin and soft tissue infections. Microbiol. Spect. 2022, 10, e0035122. [Google Scholar] [CrossRef] [PubMed]
- Jacob, B.; Makarewicz, O.; Hartung, A.; Brodt, S.; Roehner, E.; Matziolis, G. In vitro additive effects of dalbavancin and rifampicin against biofilm of Staphylococcus aureus. Sci. Rep. 2021, 11, 23425. [Google Scholar] [CrossRef]
- Boucher, H.W.; Wilcox, M.; Talbot, G.H.; Puttagunta, S.; Das, A.F.; Dunne, M.W. Once-weekly dalbavancin versus daily conventional therapy for skin infection. N. Engl. J. Med. 2014, 370, 2169–2179. [Google Scholar] [CrossRef]
- Poliseno, M.; Bavaro, D.F.; Brindicci, G.; Luzzi, G.; Carretta, D.M.; Spinarelli, A.; Messina, R.; Miolla, M.P.; Achille, T.I.; Dibartolomeo, M.R.; et al. Dalbavancin efficacy and impact on hospital length-of-stay and treatment costs in different gram-positive bacterial infections. Clin. Drug Investig. 2021, 41, 437–448. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Flamm, R.K.; Castanheira, M.; Sader, H.S.; Mendes, R.E. Dalbavancin in-vitro activity obtained against Gram-positive clinical isolates causing bone and joint infections in US and European hospitals (2011–2016). Antimicrob. Agents Chemother. 2018, 51, 608–611. [Google Scholar] [CrossRef]
- Morata, L.; Cobo, J.; Fernández-Sampedro, M.; Vasco, P.G.; Ruano, E.; Lora-Tamayo, J.; Somolinos, M.S.; Ruano, P.G.; Nieto, A.R.; Arnaiz, A.; et al. Safety and efficacy of prolonged use of dalbavancin in bone and joint infections. Antimicrob. Agents Chemother. 2019, 63, e02280-18. [Google Scholar] [CrossRef] [PubMed]
- Tobudic, S.; Forstner, C.; Burgmann, H.; Lagler, H.; Steininger, C.; Traby, L.; Vossen, M.G.; Winkler, S.; Thalhammer, F. Real-world experience with dalbavancin therapy in gram-positive skin and soft tissue infection, bone and joint infection. Infection 2019, 47, 1013–1020. [Google Scholar] [CrossRef]
- Silva, V.; Antão, H.S.; Guimarães, J.; Prada, J.; Pires, I.; Martins, Â.; Maltez, L.; Pereira, J.E.; Capelo, J.L.; Igrejas, G.; et al. Efficacy of dalbavancin against MRSA biofilms in a rat model of orthopaedic implant-associated infection. J. Antimicrob. Chemother. 2020, 75, 2182–2187. [Google Scholar] [CrossRef]
- Dunne, M.W.; Puttagunta, S.; Sprenger, C.R.; Rubino, C.; Van Wart, S.; Baldassarre, J. Extended-duration dosing and distribution of dalbavancin into bone and articular tissue. Antimicrob. Agents Chemother. 2015, 59, 1849–1855. [Google Scholar] [CrossRef]
- Martín, L.B.; Fernández, M.M.; Ruiz, J.M.P.; Lafont, M.O.; Paredes, L.Á.; Rodríguez, M.Á.M.; Regueras, M.F.; Morón, M.Á.M.; Lobón, G.M. Dalbavancin for treating prosthetic joint infections caused by gram-positive bacteria: A proposal for a low dose strategy. A retrospective cohort study. Rev. Esp. Quimioter. 2019, 32, 532–538. [Google Scholar]
- Barnea, Y.; Lerner, A.; Aizic, A.; Navon-Venezia, S.; Rachi, E.; Dunne, M.W.; Puttagunta, S.; Carmeli, Y. Efficacy of dalbavancin in the treatment of MRSA rat sternal osteomyelitis with mediastinitis. J. Antimicrob. Chemother. 2015, 71, 460–463. [Google Scholar] [CrossRef] [PubMed]
- Almangour, T.A.; Perry, G.K.; Terriff, C.M.; Alhifany, A.A.; Kaye, K.S. Dalbavancin for the management of gram-positive osteomyelitis: Effectiveness and potential utility. Diagn. Microbiol. Infect. Dis. 2019, 93, 213–218. [Google Scholar] [CrossRef]
- Sanz-Ruiz, P.; Matas-Diez, J.A.; Villanueva-Martínez, M.; Blanco, A.D.S.V.; Vaquero, J. Is dual antibiotic-loaded bone cement more effective and cost-efficient than a single antibiotic-loaded bone cement to reduce the risk of prosthetic joint infection in aseptic revision knee arthroplasty? J. Arthroplast. 2020, 35, 3724–3729. [Google Scholar] [CrossRef] [PubMed]
- Bouza, E.; Valerio, M.; Soriano, A.; Morata, L.; Carus, E.G.; Rodríguez-González, M.C.; Hidalgo-Tenorio, C.; Plata, A.; Muñoz, P.; Vena, A.; et al. Dalbavancin in the treatment of different gram-positive infections: A real-life experience. Int. J. Antimicrob. Agents 2018, 51, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Durante-Mangoni, E.; Gambardella, M.; Iula, V.D.; De Stefano, G.F.; Corrado, M.F.; Esposito, V.; Gentile, I.; Coppola, N. Current trends in the real-life use of dalbavancin: Report of a study panel. Int. J. Antimicrob. Agents 2020, 56, 106107. [Google Scholar] [CrossRef]
- Malchau, K.S.; Tillander, J.; Zaborowska, M.; Hoffman, M.; Lasa, I.; Thomsen, P.; Malchau, H.; Rolfson, O.; Trobos, M. Biofilm properties in relation to treatment outcome in patients with first-time periprosthetic hip or knee joint infection. J. Orthop. Transl. 2021, 30, 31–40. [Google Scholar]
- Davidson, D.J.; Spratt, D.; Liddle, A.D. Implant materials and prosthetic joint infection: The battle with the biofilm. EFORT Open Rev. 2019, 4, 633–639. [Google Scholar] [CrossRef]
- López-Torres, I.I.; Vaquero-Martín, J.; Torres-Suárez, A.I.; Navarro-García, F.; Fraguas-Sánchez, A.I.; León-Román, V.E.; Sanz-Ruíz, P. The tale of microencapsulated rifampicin: Is it useful for the treatment of periprosthetic joint infection? Int. Orthop. 2022, 46, 677–685. [Google Scholar] [CrossRef]
- Silva, T.; Silva, J.C.; Colaco, B.; Gama, A.; Duarte-Araújo, M.; Fernandes, M.H.; Bettencourt, A.; Gomes, P. In vivo tissue response and antibacterial efficacy of minocycline delivery system based on polymethylmethacrylate bone cement. J. Biomater. Appl. 2018, 33, 380–391. [Google Scholar] [CrossRef]
- Lawrie, C.M.; Jo, S.; Barrack, T.; Roper, S.; Wright, R.W.; Nunley, R.M.; Barrack, R.L. Local delivery of tobramycin and vancomycin in primary total knee arthroplasty achieves minimum inhibitory concentrations for common bacteria causing acute prosthetic joint infection. Bone Jt. J. 2020, 102 (Suppl. A), 163–169. [Google Scholar] [CrossRef]
- Martínez-Moreno, J.; Merino, V.; Nácher, A.; Rodrigo, J.L.; Yuste, B.B.B.; Merino-Sanjuán, M. Bioactivity of ceftazidime and fluconazole included in polymethyl methacrylate bone cement for use in arthroplasty. J. Arthroplast. 2017, 32, 3126.e1–3133.e1. [Google Scholar] [CrossRef] [PubMed]
- Amerstorfer, F.; Fischerauer, S.; Sadoghi, P.; Schwantzer, G.; Kuehn, K.D.; Leithner, A.; Glehr, M. Superficial vancomycin coating of bone cement in orthopedic revision surgery: A safe technique to enhance local antibiotic concentrations. J. Arthroplast. 2017, 32, 1618–1624. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.; Cai, X.-Z.; Shi, M.-M.; Ying, Z.-M.; Hu, B.; Zhou, C.-H.; Wang, W.; Shi, Z.-L.; Yan, S.-G. In Vitro and In Vivo Evaluation of Vancomycin-Loaded PMMA Cement in Combination with Ultrasound and Microbubbles-Mediated Ultrasound. BioMed Res. Int. 2015, 2015, 309739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minelli, E.B.; Benini, A.; Samaila, E.; Bondi, M.; Magnan, B. Antimicrobial activity of gentamicin and vancomycin combination in joint fluids after antibiotic-loaded cement spacer implantation in two-stage revision surgery. J. Chemother. 2015, 27, 17–24. [Google Scholar] [CrossRef]
- Hsu, Y.-H.; Hu, C.-C.; Hsieh, P.-H.; Shih, H.-N.; Ueng, S.W.; Chang, Y. Vancomycin and ceftazidime in bone cement as a potentially effective treatment for knee periprosthetic joint infection. J. Bone Jt. Surg. 2017, 99, 223–231. [Google Scholar] [CrossRef]
- Meeker, D.G.; Beenken, K.E.; Mills, W.B.; Loughran, A.J.; Spencer, H.J.; Lynn, W.B.; Smeltzer, M.S. Evaluation of Antibiotics Active against Methicillin-Resistant Staphylococcus aureus Based on Activity in an Established Biofilm. Antimicrob. Agents Chemother. 2016, 60, 5688–5694. [Google Scholar] [CrossRef]
- Darouiche, R.; Mansouri, M. Dalbavancin compared with vancomycin for prevention of Staphylococcus aureus colonization of devices in vivo. J. Infect. 2005, 50, 206–209. [Google Scholar] [CrossRef]
- Díaz-Navarro, M.; Hafian, R.; Manzano, I.; Pérez-Granda, M.J.; Cercenado, E.; Pascual, C.; Rodríguez, C.; Muñoz, P.; Guembe, M. A dalbavancin lock solution can reduce enterococcal biofilms after freezing. Infect. Dis. Ther. 2022, 11, 743–755. [Google Scholar] [CrossRef]
- Oliva, A.; Stefani, S.; Venditti, M.; Di Domenico, E.G. Biofilm-related infections in gram-positive bacteria and the potential role of the long-acting agent dalbavancin. Front. Microbiol. 2021, 12, 749685. [Google Scholar] [CrossRef]
- Morris, J.L.; Letson, H.L.; Grant, A.; Wilkinson, M.; Hazratwala, K.; McEwen, P. Experimental model of peri-prosthetic infection of the knee caused by Staphylococcus aureus using biomaterials representative of modern TKA. Biol. Open 2019, 8, bio045203. [Google Scholar] [CrossRef]
- Silva, V.; Miranda, C.; Antão, H.S.; Guimarães, J.; Prada, J.; Pires, I.; Maltez, L.; Pereira, J.E.; Capelo, J.L.; Igrejas, G.; et al. Therapeutic potential of dalbavancin in a rat model of methicillin-resistant Staphylococcus aureus (MRSA)-osteomyelitis. Int. J. Antimicrob. Agents 2020, 56, 106021. [Google Scholar] [CrossRef] [PubMed]
- Almangour, T.A.; Alhifany, A.A. Dalbavancin for the management of osteomyelitis: A major step forward? J. Antimicrob. Chemother. 2020, 75, 2717–2722. [Google Scholar] [CrossRef] [PubMed]
- Levack, A.E.; Turajane, K. Thermal stability and in vitro elution kinetics of alternative antibiotics in polymethylmethacrylate (PMMA). Bone Cem. 2021, 103, 1694–1704. [Google Scholar] [CrossRef] [PubMed]
- Slane, J.; Gietman, B.; Squire, M. Antibiotic elution from acrylic bone cement loaded with high doses of tobramycin and vancomycin. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2018, 36, 1078–1085. [Google Scholar] [CrossRef]
- Klekamp, J.; Dawson, J.M.; Haas, D.W.; DeBoer, D.; Christie, M. The use of vancomycin and tobramycin in acrylic bone cement: Biomechanical effects and elution kinetics for use in joint arthroplasty. J. Arthroplast. 1999, 14, 339–346. [Google Scholar] [CrossRef]
- Azanza, J.R.; Sádaba, B.; Reis, J. Dalbavancin: Pharmacokinetic and pharmacodynamic parameters. Enferm. Infecc. Microbiol. Clin. 2017, 35 (Suppl. 1), 22–27. [Google Scholar] [CrossRef]


{kind=link}
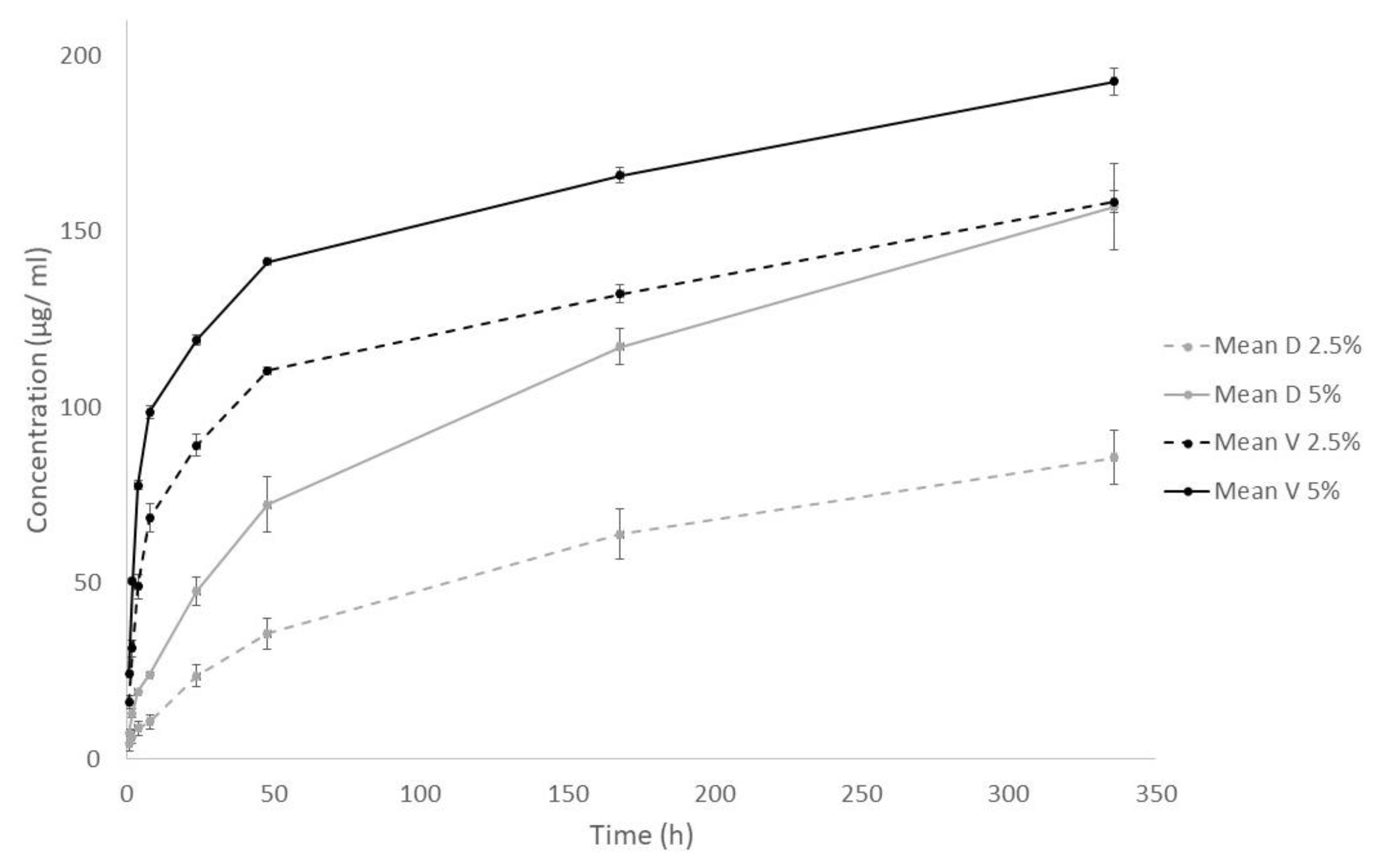
| Time (Hours) | Cumulative Concentration (µg/mL) Mean ± SD | |||
|---|---|---|---|---|
| 2.5% V | 5% V | 2.5% D | 5% D | |
| 1 | 16.13 (1.88) | 24.44 (0.42) | 4.35 (1.92) | 7.43 (1.18) |
| 2 | 31.49 (2.44) | 50.54 (0.77) | 6.32 (2.00) | 13.05 (1.30) |
| 4 | 49.08 (3.56) | 77.95 (1.37) | 8.75 (1.97) | 19.25 (0.39) |
| 8 | 68.60 (4.15) | 98.68 (0.86) | 10.58 (1.91) | 23.98 (0.56) |
| 24 | 89.31 (3.25) | 119.27 (1.39) | 23.70 (3.13) | 47.82 (3.96) |
| 48 | 110.55 (1.07) | 141.48 (0.57) | 35.68 (4.35) | 72.45 (7.71) |
| 168 | 132.29 (2.65) | 166.07 (2.28) | 63.98 (7.08) | 117.32 (5.23) |
| 336 | 158.49 (3.09) | 192.67 (3.92) | 85.73 (7.64) | 157.12 (12.43) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Somolinos, M.; Díaz-Navarro, M.; Benjumea, A.; Tormo, M.; Matas, J.; Vaquero, J.; Muñoz, P.; Sanz-Ruíz, P.; Guembe, M. Determination of the Elution Capacity of Dalbavancin in Bone Cements: New Alternative for the Treatment of Biofilm-Related Peri-Prosthetic Joint Infections Based on an In Vitro Study. Antibiotics 2022, 11, 1300. https://doi.org/10.3390/antibiotics11101300
Sánchez-Somolinos M, Díaz-Navarro M, Benjumea A, Tormo M, Matas J, Vaquero J, Muñoz P, Sanz-Ruíz P, Guembe M. Determination of the Elution Capacity of Dalbavancin in Bone Cements: New Alternative for the Treatment of Biofilm-Related Peri-Prosthetic Joint Infections Based on an In Vitro Study. Antibiotics. 2022; 11(10):1300. https://doi.org/10.3390/antibiotics11101300
Chicago/Turabian StyleSánchez-Somolinos, Mar, Marta Díaz-Navarro, Antonio Benjumea, Marta Tormo, José Matas, Javier Vaquero, Patricia Muñoz, Pablo Sanz-Ruíz, and María Guembe. 2022. "Determination of the Elution Capacity of Dalbavancin in Bone Cements: New Alternative for the Treatment of Biofilm-Related Peri-Prosthetic Joint Infections Based on an In Vitro Study" Antibiotics 11, no. 10: 1300. https://doi.org/10.3390/antibiotics11101300