Changes in the incidence of acute bacterial meningitis caused by Streptococcus pneumoniae and the implications of serotype replacement in children in Colombia after mass vaccination with PCV10
 Juan David Farfán-Albarracín1,2,3†
Juan David Farfán-Albarracín1,2,3†  Germán Camacho-Moreno1,2,3,4*†
Germán Camacho-Moreno1,2,3,4*†  Aura Lucia Leal1,5,6
Aura Lucia Leal1,5,6  Jaime Patiño1,7 Wilfrido Coronell1,8 Iván Felipe Gutiérrez1,9,10 Sandra Beltrán1,11
Jaime Patiño1,7 Wilfrido Coronell1,8 Iván Felipe Gutiérrez1,9,10 Sandra Beltrán1,11  Martha I. Álvarez-Olmos1,6,12 Cristina Mariño1,13 Rocio Barrero1,14,15 Juan Pablo Rojas1,16,17,18 Fabio Espinosa1,4
Martha I. Álvarez-Olmos1,6,12 Cristina Mariño1,13 Rocio Barrero1,14,15 Juan Pablo Rojas1,16,17,18 Fabio Espinosa1,4  Catalina Arango-Ferreira1,19,20 Maria Alejandra Suarez1,21 Monica Trujillo1,22
Catalina Arango-Ferreira1,19,20 Maria Alejandra Suarez1,21 Monica Trujillo1,22  Eduardo López-Medina1,23 Pio López1,24 Hernando Pinzón1,8
Eduardo López-Medina1,23 Pio López1,24 Hernando Pinzón1,8  Nicolás Ramos1,25
Nicolás Ramos1,25  Vivian Marcela Moreno1 Anita Montañez1
Vivian Marcela Moreno1 Anita Montañez1- 1Red Neumocolombia, Bogotá, Colombia
- 2Departamento de Pediatría, Facultad de Medicina, Universidad Nacional de Colombia, Bogotá, Colombia
- 3HOMI-Fundación Hospital Pediátrico La Misericordia, Bogotá, Colombia
- 4Hospital Infantil Universitario de San José, Bogotá, Colombia
- 5Departamento de Microbiología, Facultad de Medicina, Universidad Nacional de Colombia, Bogotá, Colombia
- 6Grupo para el Control de la Resistencia Bacteriana en Bogotá (GREBO), Bogotá, Colombia
- 7Fundación Valle de Lili, Cali, Colombia
- 8Hospital Infantil Napoleón Franco Pareja, Cartagena, Colombia
- 9Clínica Infantil Colsubsidio, Bogotá, Colombia
- 10Clínica Infantil Santa María del Lago-Colsánitas, Bogotá, Colombia
- 11Clínica Universitaria Colombia-Clínica Pediátrica Colsanitas, Bogotá, Colombia
- 12Fundación Cardioinfantil-Instituto de Cardiología, Bogotá, Colombia
- 13Hospital Militar Central, Bogotá, Colombia
- 14Hospital Universitario Clínica San Rafael, Bogotá, Colombia
- 15Unidad de Servicios de Salud Santa Clara, Subred Centro Oriente, Bogotá, Colombia
- 16Fundación Clínica Infantil Club Noel, Cali, Colombia
- 17Facultad de Ciencias de la Salud, Universidad Libre Seccional Cali, Cali, Colombia
- 18Facultad de Salud, Universidad del Valle, Cali, Colombia
- 19Hospital Universitario San Vicente Fundación, Medellín, Colombia
- 20Departamento de Pediatría, Facultad de Medicina, Universidad de Antioquia, Medellin, Colombia
- 21Unidad de Servicio de Salud Tunal, Bogotá, Colombia
- 22Hospital Pablo Tobón Uribe, Medellín, Colombia
- 23Centro Médico Imbanaco, Cali, Colombia
- 24Hospital Universitario del Valle, Cali, Colombia
- 25Los COBOS Medical Center, Bogotá, Colombia
Introduction: Acute bacterial meningitis (ABM) is a public health problem. The disease has reemerged after the introduction of pneumococcal conjugate vaccines (PCVs) due to an increase in serotypes that are not covered. The objective was to determine the changes in the disease incidence before and after the introduction of the 10-valent vaccine (PCV10) in Colombia.
Methods: This multicenter study was conducted in 17 hospitals in Colombia. Data were collected from January 2008 to December 2019 in 10 hospitals in Bogotá and from January 2017 to December 2019 in seven hospitals in Cali, Medellín and Cartagena. The data were grouped into three periods: 2008–2011, 2012–2015, and 2016-2019.
Results: Of the 706 cases of invasive pneumococcal disease, 81 (11.4%) corresponded to meningitis. The relative incidence in Bogotá in the first period was 0.6 per 100,000 patients ≤ 5 years, decreased to 0.4 per 100,000 patients ≤ 5 years in the second period and increased in the third period to 0.7 per 100,000 patients ≤ 5 years. Serotypes covered by PCV10 decreased from 75 to 9.1%, with Spn19A (31.8%) and Spn34 (13.6%) emerging in the third period. Increased resistance to penicillin (13 to 37%) and to ceftriaxone (5.9 to 16%) was due to the emergence of multidrug-resistant Spn19A. The total mortality rate was 23.5% and increased from 12 to 33%.
Conclusions: ABM due to pneumococcus has high morbidity and mortality rates. Reemergence of the disease has been observed due to the inclusion of polymerase chain reaction (PCR) for diagnosis and replacement of circulating serotypes after the introduction of PCV10, with an increase in Spn19A, which causes death and exhibits antimicrobial resistance. Continued surveillance is needed.
Introduction
Acute bacterial meningitis (ABM) is a public health problem with high morbidity and mortality rates, especially in children under 5 years of age. One of the most common causative microorganisms is Streptococcus pneumoniae (Spn). In 2015, Wahl et al. estimated 83,900 cases of ABM caused by pneumococcus in children under 5 years of age worldwide, with an incidence of 13 in 100,000 and a mortality rate of 44%. Of the 37,900 deaths, 53.8% occurred in Africa and 26.9% in Southeast Asia. In America, 2,300 cases of ABM due to pneumococcus were reported in children under 5 years of age (incidence of 3 in 100,000), and 600 (27%) children died (1). In Colombia, in 2019, 64 cases of pneumococcal meningitis were reported in children under 18 years of age, and 35 occurred in children under 5 years of age (incidence 1.03 cases per 100,000 children under 5 years of age), with a mortality rate of 18%. In this age group, mortality rates as high as 44% were reported in 2017 (2, 3).
The World Health Organization (WHO) established a roadmap to defeat meningitis by 2030. Pillar 2 refers to optimizing diagnosis and treatment, for which molecular diagnostic techniques have been implemented that have allowed researchers to improve microorganism detection, and pillar 3 refers to the need to determine the epidemiology of this disease, strengthening surveillance systems and encouraging research on the subject (4). Vaccines against Streptococcus pneumoniae, Neisseria meningitidis and Haemophilus influenzae type b have been developed to control this disease (4, 5). Worldwide, a decrease in the incidence of pneumococcal meningitis has been observed after the application of pneumococcal conjugate vaccines (PCVs). In recent years, serotypes not included in PCVs that are applied systematically have emerged, leading to a reemergence of the disease (6).
The main clinical manifestations are fever, headache, nuchal rigidity, confusion, an altered state of consciousness, general malaise, epileptic seizures and vomiting, depending mainly on the age of the patient (7). Other nonspecific symptoms have been described as clinical characteristics in children, including hypothermia, rejection of the oral administration route, bulging of fontanelles, irritability and alternation between irritability and drowsiness (5, 8). In addition, in children under 12 months of age, meningeal signs may be absent, further complicating the diagnostic process (5, 9, 10).
One factor that has changed the behavior of the disease worldwide is vaccination (11). For S. pneumoniae, conjugate vaccines have been designed against seven serotypes (4, 6B, 9V, 14, 18C, 19F, 23F), 10 serotypes (PCV 7 + 1, 5, 7F), 13 serotypes (PCV 10 + 3, 6A, 19A), 15 serotypes (PCV 13 + 22F, 33F) and 20 serotypes (PCV 15 + 8, 10A, 11A, 12F, 15B). As of June 2019, 37 countries in the Americas had introduced some of the PCVs into their schedule (12). In Colombia, the first vaccine introduced was the seven-valent vaccine (PCV7), initially in the city of Bogotá in 2008, and subsequently, the 10-valent vaccine (PCV10) was introduced nationwide in 2012.
The Neumocolombia network is an initiative of the Central Chapter of the Colombian Association of Infectious Diseases (Asociación Colombiana de Infectología–ACIN) and the Colombian Society of Pediatrics (Sociedad Colombiana de Pediatría-SCP) that monitors the behavior of invasive pneumococcal disease (IPD). The objective of this study was to determine the clinical, microbiological and epidemiological changes that have occurred in pneumococcal meningitis in children before and after the introduction of mass vaccination in Colombia.
Methodology
Patients aged younger than 18 years with ABM confirmed to be caused by S. pneumoniae were included and were defined as patients with a suggestive clinical presentation, cerebrospinal fluid (CSF) findings compatible with ABM and isolation of the microorganism in blood culture and/or CSF culture and/or detection by polymerase chain reaction (PCR) in CSF. Data were collected ambispectively from January 1, 2008, to December 31, 2019, in the city of Bogotá DC and from January 1, 2017, to December 31, 2019, in Cartagena, Cali and Medellín, for a total of 17 centers in Colombia. A questionnaire was designed for online data collection.
For bacterial identification and susceptibility, automatized methods were used (16 centers–Vitek 2™, and one center–BD Phoenix™ technology). The CLSI 2018 criteria for minimum inhibitory concentrations (MICs) were applied to classify susceptible, intermediate and resistant isolates for each antibiotic drug. As part of routine surveillance, isolates should be sent to local health departments (Secretarías Departamentales de Salud–SDS), where the isolates are reconfirmed and sent to the National Institute of Health (INS), where serotyping by the Quellung method and by polymerase chain reaction, as appropriate, is performed. The serotyping data were taken from the report sent by the SDS and INS to the institutions.
The data were grouped according to the start of mass vaccination with PCV in Colombia in 2012 into three different periods: prevaccination period from 2008 to 2011, transition period from 2012 to 2015 and postvaccination period from 2016 to 2019. Subsequently, the data were analyzed with the R statistics 4.1.1 tool (R Foundation for Statistical Computing, Vienna, Austria) via the software package RStudio version 1.4.1717 (RStudio, PBC, Boston, MA), initially with descriptive methods, including means, medians, standard deviations and interquartile ranges, according to the characteristics of the different variables. The values of different variables were compared, such as cell counts in blood and CSF and levels of glucose and C-reactive protein, according to specific outcomes, which included mortality and the presence of complications, using Wilcoxon rank tests or T-tests according to the characteristics of the evaluated variable. Subsequently, reference points were established for the significant variables after considering the clinical relevance of each variable. For categorical variables, the chi-square test or Fisher's exact test was used, according to the characteristics of the population, and the ORs were calculated for different outcomes, as previously mentioned.
Results
During the study period, 706 cases of IPD were identified. Of these, 81 cases (11.4%) corresponded to meningitis, 66 (81.4%) cases were from Bogotá D.C., and 15 (18.5%) cases were from outside Bogotá D.C. (seven from Cali, five from Medellín and three from Cartagena). A total of 17.3% of patients had concomitant pneumonia. The median age was 39 months (range 0–211 months), 61.7% of patients were male, 66.6% of patients were affiliated with the contributory regimen, and 29.6% were affiliated with the subsidized regimen. In 69.1% of patients, the admission diagnosis was neuroinfection, followed by pneumonia (4.9%), febrile syndrome (2.4%) and complex febrile seizures (2.4%). Table 1 shows the demographic data and characteristics of the population.
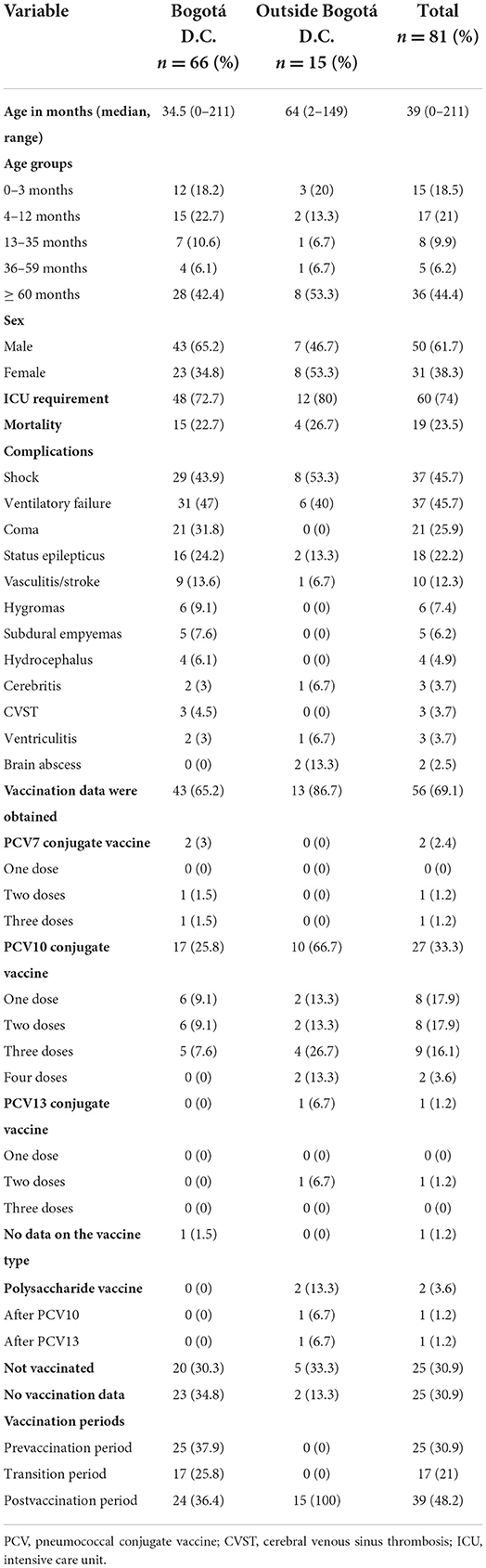
Table 1. Demographic and clinical characteristics of patients with pneumococcal meningitis.
Of the total patients with meningitis, 45 (55.5%) were younger than 5 years of age, and 32 (39.5%) corresponded to the population 12 months old or younger (Table 1). Sixteen percent of patients used an antibiotic prior to the diagnosis of meningitis; in most cases, amoxicillin or ceftriaxone was used. The most frequent antecedent was CSF fistula in 17.3% of patients, followed by immunodeficiency and chronic neurological disease in 3.7%, chronic pneumopathy and craniofacial malformations in 2.5% and kidney failure and chronic endocrinological disease in 1.2% each. Vaccination data were obtained for 56 (69.1%) of the patients, 25 of whom (30.9%) had not received any vaccine, while 27 (33.3%) had received at least one dose of PCV10. Eleven of these patients (19.7%) had received a complete vaccination schedule, two patients had received PCV7, one received PCV13, and two received PSP23 after PCV10 and PCV13 (Table 1). Eighty percent and 100% of patients who were infected with Spn19A and Spn34, respectively, had received at least one dose of PCV10 (Supplementary material, Supplementary Figure S2).
The most common symptoms were fever, hyporexia, drowsiness and vomiting. Epileptic seizures ranked fifth, with the rate reaching 48.2%. Specific symptoms of acute meningitis, such as headache, nuchal rigidity or signs of meningeal irritation, were present in 39.5, 34.6, and 14.8% of patients, respectively. The frequency of these symptoms differed according to the age group of the patient (Supplementary material, Supplementary Figure S1). A higher prevalence of epileptic seizures was observed in patients younger than 12 months; in contrast, classic signs of acute meningitis, such as those described above, were present at a higher prevalence in children older than 36 months. Patients with Spn19A infections showed peaks between 13 and 36 months of age (44.4% of cases) after the last dose of the vaccine scheme, and their symptoms were similar to those previously described for this group, with a predominance of fever (88.9%), followed by irritability (66.7%), vomiting (44.4%), drowsiness (44.4%) and poor feeding (44.4%). The median symptom duration on admission was 3 days. The most prominent findings in the CSF studies were hypoglycorrhachia, with a median of 10 mg/dl [interquartile range (IQR) 1.6–39.5 mg/dl]; a low glycorrhachia/serum glucose ratio, with a median of 0.05 (IQR 0.01–0.29); hyperproteinorrhea, with a median of 272.1 (IQR 115.2–335.4); pleocytosis, with a median of 220 (IQR 36–1250) and a polymorphonuclear predominance; and positive Gram staining for gram-positive cocci in 70.4% of patients (Supplementary material, Supplementary Table S1).
Neuroimaging was performed in 54 (66.7%) patients with the cranial tomography (CT) scanning modality and in 24 (29.6%) patients with the brain magnetic resonance imaging (MRI) modality. The most frequent findings were parameningeal foci (mastoiditis or sinusitis), followed by normal neuroimaging (31.5 and 30.9% on CT and 37.5 and 29.2% on MRI, respectively). Cerebral edema was the third most frequent finding on tomography scans (27.8%). Likewise, meningeal enhancement was observed on brain MRI in 25% of patients, while this finding was observed on tomography scans in 5.6% of patients. These findings were more common in the Spn19A infection group, with parameningeal foci (CT: 60%, MRI: 50%), cerebral edema (CT: 20%, MRI: 50%), meningeal enhancement (CT: 20%, MRI: 50%) and normal images (CT: 20%, MRI: 50%) noted in a limited sample of patients (n = 5 for CT and n = 2 for MRI).
Relative incidence data were calculated with respect to the population aged 0 to 5 years in Bogota, including data from 10 hospitals in this city with data available from the beginning of the study. As shown in Figure 1, an increase in the number of cases was observed in the postvaccination period (2016 to 2019), with an average incidence of 0.69 cases per 100,000 inhabitants under 5 years of age, compared with the data from the transition period (2012 to 2015), which showed an average incidence of 0.35 cases per 100,000 inhabitants under 5 years of age, and the prevaccination period, where the average incidence was 0.62 cases per 100,000 inhabitants. In 75 (92.6%) patients, S. pneumoniae was isolated by CSF culture or blood culture, while in six patients (7.4%), it was performed only by molecular tests [real-time PCR (RT–PCR) multiplex-FilmArray®] for one patient in 2018 and five in 2019. This technology was not available in the first two periods of the study, and thus, the incidence in the postvaccination period (2016 to 2019) was also calculated without including these cases at 0.4 cases in 100,000 children under 5 years of age, which is lower than the incidence in the prevaccination period and higher than the incidence in the transition period (Figure 1). The data from the network represent 47% of the cases of IPD that Bogotá reports to the surveillance system (13).
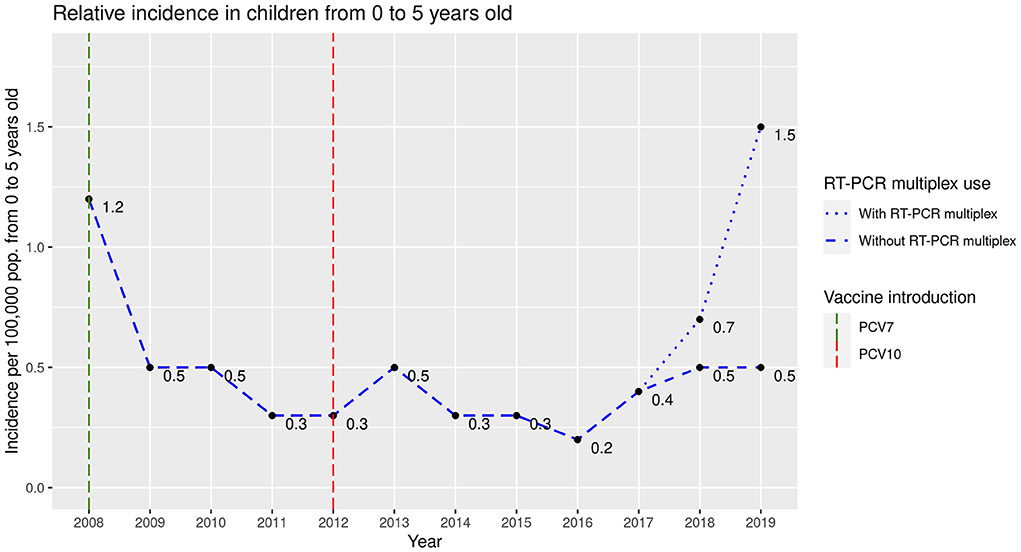
Figure 1. Relative incidence of acute bacterial meningitis in children between 0 and 5 years of age in Bogotá.
The serotype was obtained in 50 (61.7%) cases; the bacterial serotype was not obtained in any of the six cases detected using RT–PCR. When performing the analysis of the serotypes, the serotypes included in PCV10 were rare in vaccinated patients, while serotypes 19A and 34 were more frequent in vaccinated patients than in unvaccinated patients (Supplementary material, Supplementary Figure S2). When the serotypes were analyzed according to the vaccination period, the serotypes included in the PCV10 vaccine decreased in prevalence from 75 to 9.1% in the prevaccination and postvaccination periods, respectively, while the emerging serotypes were mainly represented by Spn19A and Spn34, with 31.8 and 13.6% prevalence, respectively, in the postvaccination period (Figure 2).
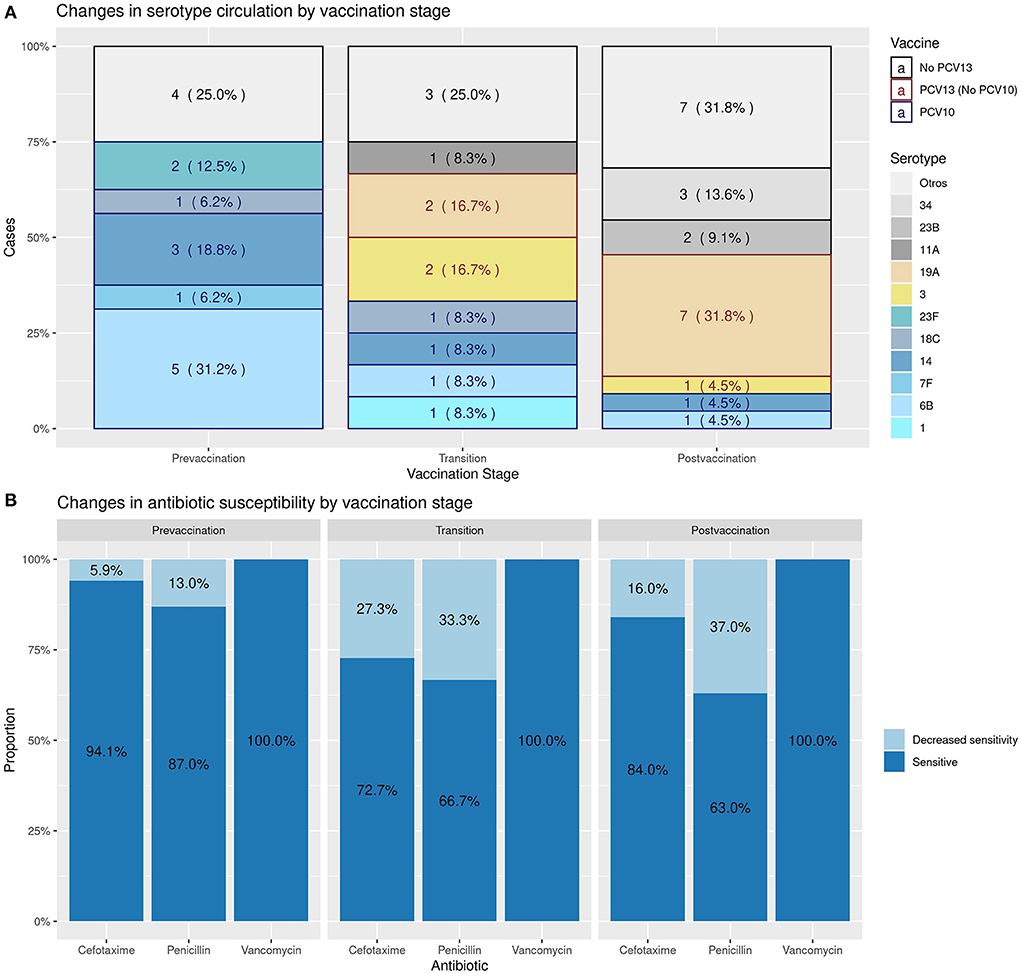
Figure 2. Changes in the circulation of serotypes and in bacterial resistance according to the vaccination period.
Likewise, Figure 2 shows the antimicrobial sensitivity to the most frequently used antibiotics to treat IPD, such as penicillin, cefotaxime and vancomycin, throughout the vaccination period. The sensitivity to the first two drugs decreased progressively, with a decreased sensitivity (intermediate or resistant) of 40% for penicillin and 16% for third-generation cephalosporins in the postvaccination period. Specifically, Spn19A's resistance increased from none in the transition period to 66.7% in the postvaccination period for both penicillin and cefotaxime. All isolates were sensitive to vancomycin.
The most empirically used antibiotics were third-generation cephalosporins (90.1%), followed by vancomycin (69.1%) and ampicillin (9.9%). The empirical use of glycopeptides increased from 60% in the prevaccination period to 71.8% in the postvaccination period. Likewise, vancomycin was maintained as part of the treatment after the results of the susceptibility testing in 0% of the patients in the prevaccination period, in 11.8% in the transition period and in 12.8% in the postvaccination period.
The rate of dexamethasone use in combination with antibiotics was 22.2%; dexamethasone was started simultaneously with antibiotics in 50% of patients and started before antibiotics in 22.2%. The median hospital stay duration was 16 days, and 60 (74%) patients required admission to the intensive care unit, with a median stay of 4 days.
The most frequent complications were severe shock, ventilatory failure, coma, status epilepticus and central nervous system vasculitis or stroke (Table 1). Some important differences were observed between the no Spn19A and Spn19A groups in severe shock (46.3 vs. 55.6%), cerebritis (2.4 vs. 11.1%) and status epilepticus (26.8 vs. 11.1%), none of which were statistically significant. The mortality rate of the disease reached 23% and varied, with an important increase since the prevaccination period from 12% compared with those in the transition (17.6%) and postvaccination (33.3%) periods. This difference between the prevaccination period and postvaccination period was not statistically significant (p = 0.104).
In the bivariate analysis, associations were observed between lower blood counts of leukocytes, neutrophils and monocytes, higher C-reactive protein levels, lower glucose levels in CSF and a younger age with a greater probability of presenting some complication. Finally, lower leukocyte and neutrophil counts, lower hemoglobin levels, a higher C-reactive protein level in blood and a lower glucose level in CSF were associated with higher mortality (Table 2).
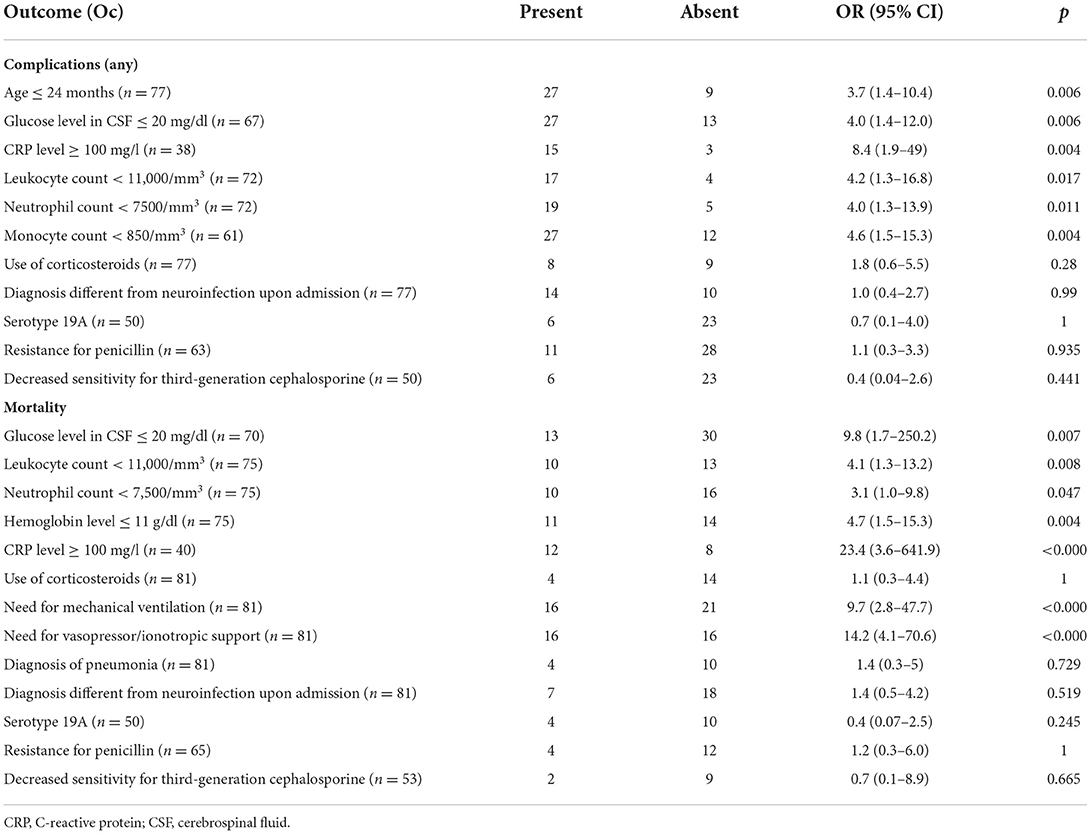
Table 2. Variables associated with greater complications and greater lethality.
Discussion
ABM due to S. pneumoniae in pediatric patients is a pathology with diverse clinical manifestations, making its diagnosis and timely treatment difficult. This study is one of the largest case series analyses of the disease, which exclusively includes the pediatric population. Likewise, all age pediatric groups are represented, with cases predominantly occurring in the first 36 months of life, including a slightly higher proportion of males, which has also been described in other cohorts (14–16).
In the present study, significant variation was observed in the most frequent symptoms according to the age group, with nonspecific manifestations observed in patients under 12 months of age. This diversity of symptoms, as well as their lack of specificity at early ages, has been reported in other local studies, where fever (93%), vomiting (78%), an altered state of consciousness (42%) and headache (40%) are described as the main symptoms (7). Symptoms did not significantly vary with Spn19A infection in this study. Likewise, symptoms similar to those mentioned in the present study were reported in a systematic review of the clinical characteristics of meningitis in children, and the best predictors of meningitis were bulging fontanelle, epileptic seizures and hyporexia, but the ideal combination of symptoms for diagnosis was unclear (17). Thus, a high diagnostic suspicion is necessary from admission to the emergency unit.
On the other hand, in terms of laboratory tests, hypoglycemia and hyperproteinorrhachia were observed, which are expected in the context of bacterial meningitis, with values similar to those reported in other studies (16). In previous studies, very high levels of C-reactive protein were associated with a higher rate of complications and sequelae of bacterial meningitis in children (18). However, in our study, C-reactive protein was also associated with mortality. In this study, blood leukocyte and neutrophil counts below the expected values, as well as the presence of anemia, were associated with mortality and complications. Other factors associated with mortality described in other studies, such as severe hypoglycemia (15), were also identified in our study.
Regarding the two neuroimaging techniques used, tomography and MRI, signs with high specificity for the diagnosis of meningitis are rare, their diagnostic value is scarce, and they do not replace biochemical and microbiological studies. The greatest utility of these studies is in detecting disease complications and not in the diagnostic process itself, as can be concluded from specific research on the subject (19, 20).
The trends in the incidence of the cases described (Figure 1), specifically in the city of Bogotá, correlated with the annual incidence among children under 5 years of age reported by the National Institute of Health in Colombia, with a rate of 1.19 per 100,000 children under 5 years of age in 2009 (21), which decreased to 0.51 per 100,000 children under 5 years of age in 2012 (22), remained stable between 0.54 and 0.63 per 100,000 children under 5 years of age between 2013 and 2018 (2, 23–27) and increased to 1.03 cases per 100,000 children under 5 years of age in 2019 (3). The implementation of molecular diagnostic techniques has increased the number of confirmed cases, allows the incidence and burden of the disease to be established more accurately and facilitates more timely treatment (28).
The behavior after mass vaccination reveals that in the first years after the introduction of vaccines, the incidence decreased, but a progressive increase in the relative incidence of ABM due to pneumococcus was observed in the postvaccination period, which may be mainly due to two factors: serotype replacement and the introduction of diagnostic strategies other than culture and/or antigen detection, such as detection using RT–PCR. Although the change in incidence without molecular testing was small, there was an increase respect to the minimum value (Figure 1). The phenomenon of serotype replacement has also been described in other regions of the world where PCVs have been introduced (14, 16, 29). The increase in the prevalence of serotypes not covered by PCV10 in IPD, especially Spn19A, has already been observed previously in Colombian cohorts of children and adults (30, 31), in Latin American cohorts (32) and in other regions of the world (6, 33). Notably, Spn34 has been reported only occasionally in patients with this disease.
On the other hand, we observed that resistance to third-generation cephalosporins increased from the prevaccination period to the postvaccination period, a phenomenon that has also been reported in other regions where PCV7 or PCV10 has been introduced (34), which is associated with an increase in the proportion of multidrug-resistant Spn19A (35). In this study, Spn19A decreased sensitivity changed from 0 to 66.7%. In Colombia, similar to other countries, this serotype has been associated with the ST320 clonal complex (36–38). PCVs decrease antimicrobial resistance to the extent that resistant and prevalent serotypes are included in them. Other factors, such as the nasopharyngeal carrying capacity and the inappropriate use of antibiotics, may be determining factors in the generation of resistance (39, 40). The introduction of vaccines with greater coverage in serotypes, especially against Spn19A, might help reduce resistance, along with the introduction of policies and strategies that promote an adequate and rational use of antibiotics (39, 40).
The increase in resistance affects the use of antibiotics, as observed for vancomycin in the transition and postvaccination periods, as its empiric use and its use in targeted treatment showed an important increase in the study population.
The use of dexamethasone as part of treatment has shown usefulness mainly in reducing sequelae and mortality associated with the disease (41, 42). However, the use of this drug by the study population was low.
Severe complications were observed in approximately half of the patients, and the high mortality rate, which has increased in recent periods, might be considered a consequence of the circulation of more virulent serotypes and greater resistance to antibiotics, although this finding was not statistically significant in this study (Table 2). These values are greater than those reported in other studies examining the burden of pneumococcal meningitis in children, where up to 67.3% of children were admitted to the intensive care unit, and only 23.1% required invasive mechanical ventilation (43). The severity seems to be greater with Spn19A infection in terms of complications and mortality, but the differences were not statistically significant.
Mass vaccination in Colombia had the expected effect, with an initial decrease in the number of cases related to the serotypes included in the vaccine and a subsequent increase that was probably secondary to the circulation of serotypes that are not included, especially Spn19A, with a significant effect on severity of the disease and resistance to antibiotics. These data have been confirmed by the laboratory reports of the National Institute of Health, which show variation in resistance patterns from an intermediate or resistant sensitivity of 28.3% for meningeal isolates to third-generation cephalosporins between 2006 and 2007 in children under 5 years of age to 35.3% for the period from 2017 to 2018 (13). Therefore, new strategies, including the use of vaccines with greater serotype coverage, strengthening of diagnostic strategies and awareness regarding the disease and improvements in therapeutic strategies using tools that reduce sequelae, complications and lethality, must be established in accordance with the objectives proposed by the WHO in the program “Defeating meningitis by 2030” (4, 44).
This study has the strength of being a multicenter study including a large number of patients with meningitis. To our knowledge, this study is the first to analyze the clinical behavior of acute bacterial meningitis after the introduction of PCV10 in Colombia. The limitations of this research include the type of data collected, which were retrospective in some cases, implying the lack of availability of some information. Another limitation is that the serotypes and vaccination status were not available for all patients, especially patients treated in the first period. During the third study period, molecular diagnostic techniques were introduced in seven hospitals of the network. This change complicates comparisons of the incidence of the disease with the rates in the first two periods. The incidence of the third period was also calculated excluding the six cases detected only with molecular tests to control for this limitation. The results of the study are related to the national data reported by the National Institute of Health of Colombia, which includes a representative sample and reduces the effects of these limitations.
ABM due to pneumococcus has high morbidity and mortality rates, and its care requires significant use of health resources. In the present study, reemergence of pneumococcal meningitis was observed partially due to the turnover in circulating serotypes after the implementation of PCV10, with an increase in the prevalence of serotypes that are not covered by PCV 10, especially Spn19A, and associated with greater antimicrobial resistance. These results are similar to findings from patients with other clinical presentations of IPD, such as bacteremic pneumonia and primary bacteriemia (22–24, 36, 45, 46), and to those reported by the national epidemiological surveillance system (3, 27–32). The data from this and other studies were analyzed by the National Council of Immunization Practices (Concejo Nacional de Prácticas de Inmunización-CNPI); in April 2022, the Ministry of Health and Social Protection of Colombia announced the change from PCV10 to PCV13, which has been administered since July 1, 2022, to children born since May 1, 2022. Continued surveillance is required to detect epidemiological changes after the inclusion of this vaccine.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving human participants were reviewed and approved by HOMI-Fundación Hospital Pediátrico La Misericordia, Bogotá, Colombia. Clínica Universitaria Colombia-Clínica Pediátrica Colsanitas, Bogotá, Colombia. Fundación Cardioinfantil-Instituto de Cardiología, Bogotá, Colombia. Hospital Militar Central, Bogotá, Colombia. Unidad de Servicio de Salud Tunal, Bogotá, Colombia. Hospital Universitario Clínica San Rafael, Bogotá, Colombia. Unidad de Servicios de Salud Santa Clara, Subred Centro Oriente, Bogotá, Colombia. Los COBOS Medical Center, Bogotá, Colombia. Hospital Infantil Universitario de San José, Bogotá, Colombia. Fundación Valle de Lili, Cali, Colombia. Fundación Clínica Infantil Club Noel, Cali, Colombia. Centro Médico Imbanaco, Cali, Colombia. Hospital Universitario San Vicente Fundación, Medellín,Colombia. Hospital Pablo Tobón Uribe, Medellín, Colombia. Hospital Infantil Napoleón Franco Pareja, Cartagena, Colombia. Hospital Universitario del Valle, Cali, Colombia. Clínica Infantil Colsubsidio, Bogotá, Colombia. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
Conception and study design, data collection, and writing of the final manuscript, editing, review, and approval: JF-A, GC-M, AL, JP, VM, WC, IG, SB, MÁ-O, CM, RB, JR, FE, CA-F, MS, MT, EL-M, PL, HP, NR, and AM. Statistical analysis: JF-A, GC-M, VM, and WC. Writing of the original manuscript: JF-A, GC-M, AL, JP, and WC. All authors contributed to the article and approved the submitted version.
Funding
This work was funded through independent Grant Number WI235048 from the Colombian Association of Infectious Diseases (Asociación Colombiana de Infectología-ACIN)-central chapter to Pfizer SAS Laboratories. The authors are responsible for the information and its analysis. Pfizer Laboratories did not participate in the preparation or analysis of the data presented in this article. The institutional researchers did not receive any remuneration for their participation in the study.
Acknowledgments
We thank the microbiology group of the National Institute of Health (Instituto Nacional de Salud-INS) of Colombia for providing information on serotyped isolates and the District Secretary of Health of Bogotá (Secretaria Distrital de Salud SDS) Bacterial Resistance Group of Bogotá (Grupo de Resistencia Bacteriana de Bogotá–GREBO), Colombian Association of Infectious Diseases (Asociacion Colombiana de Infectologia Capitulo Central) and the Colombian Society of Pediatrics (Sociedad Colombiana de Pediatria) for their collaboration and research support. Red Neumocolombia members: Daniela Jerez, HOMI, Fundación Hospital Pediátrico la Misericordia; Magda Sánchez, Fundación Cardioinfantil; Juan Pablo Londoño; Clínica Infantil Colsubsidio. Claudia Clavijo, Hospital Universitario Clínica San Rafael; Nella Sánchez; Oscar Pancha, Unidad de Servicios de Salud Santa Clara; Katherine Duran, Daniela Arevalo, Hospital Infantil Universitario de San José; Cindy Carolina Suarez, John Alexander García, Fundación Valle de Lili; Adriana Correa, Centro Médico Imbanaco; María del Palmar Aros, Clínica Infantil Club Noel; Andrea Restrepo, Hospital Pablo Tobón Uribe; Oscar Villada, Mayiver Hernando Roldan, María Gabriela Becerra, Hospital San Vicente Fundación; Alejandro Restrepo; Red Neumocolombia.
Conflict of interest
GC-M has received support from Pfizer, MSD (Merck Sharp and Dohme) and Sanofi Pasteur for participation in congresses and paid conferences, has participated in advisory boards and has received support from MSD for research. AL has received support from Pfizer and MSD (Merck Sharp and Dohme) for participation in congresses and paid conferences, has participated in advisory boards and has received support from MSD for research. JP has received support from Pfizer for participation in congresses. WC has received support from Pfizer, GSK and AstraZeneca for participation in congresses and paid conferences. IG has received support from Pfizer for participation in congresses and paid conferences. SB has received support from Pfizer for participation in congresses. MÁ-O has received support from Pfizer for participation in congresses. CM has received support from Pfizer for participation in congresses. RB has received support from Pfizer and MSD for participation in congresses. FE has received support from MSD for research. JR has received support from Pfizer for participation in congresses and paid conferences. EL-M has received research support from MSD, GSK, Sanofi Pasteur, Pfizer, Takeda and Janssen. PL has received research support from GSK, Sanofi Pasteur and Takeda.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2022.1006887/full#supplementary-material
References
1. Wahl B, O'Brien KL, Greenbaum A, Majumder A, Liu L, Chu Y, et al. Burden of Streptococcus pneumoniae and haemophilus influenzae type B disease in children in the era of conjugate vaccines: global, regional, and national estimates for 2000-15. Lancet Glob Health. (2018) 6:e744–57. doi: 10.1016/S2214-109X(18)30247-X
2. Salas HP. Informe de evento meningitis bacteriana, Colombia, año 2017. Colombia: Instituto Nacional de Salud (2018). Available online at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/MENINGITIS%20BACTERIANA%202017.pdf (accessed October 20, 2021).
3. Aparicio Fuentes SM. Informe de evento meningitis bacteriana y enfermedad meningocócica, Colombisa, 2019. Colombia: Insituto Nacional de Salud (2020). Available online at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/MENINGITIS%20BACTERIANA_2019.pdf (accessed October 20, 2021).
4. Organización Mundial de la Salud. Derrotar a la meningitis para 2030: una hoja de ruta mundial. (2021). Available online at: https://www.who.int/es/publications/i/item/9789240026407 (accessed July 12, 2022).
5. Kim KS. Acute bacterial meningitis in infants and children. Lancet Infect Dis. (2010) 10:32–42. doi: 10.1016/S1473-3099(09)70306-8
6. Koelman DLH, Brouwer MC, van de Beek D. Resurgence of pneumococcal meningitis in Europe and Northern America. Clin Microbiol Infect Off Publ Eur Soc Clin Microbiol Infect Dis. (2020) 26:199–204. doi: 10.1016/j.cmi.2019.04.032
7. Silvestre AJJ, Izquierdo BÁ, Uscátegui A, Álvarez A, Turriago RP, Baquero OL, et al. Características clínicas y paraclínicas de la meningitis bacteriana en niños. Estudio en cinco centros hospitalarios de referencia en la ciudad de Bogotá. Acta Neurol Colomb. (2007) 23:6–14. doi: 10.22379/issn.2422-4022
8. Mace SE. Acute bacterial meningitis. Emerg Med Clin North Am. (2008) 26:281–317. doi: 10.1016/j.emc.2008.02.002
9. Wu HM, Cordeiro SM, Harcourt BH, Carvalho M, Azevedo J, Oliveira TQ, et al. Accuracy of real-time PCR, gram stain and culture for streptococcus pneumoniae, neisseria meningitidis and haemophilus influenzae meningitis diagnosis. BMC Infect Dis. (2013) 13:26. doi: 10.1186/1471-2334-13-26
10. Davis LE. Acute bacterial meningitis. Contin Minneap Minn. (2018) 24:1264–83. doi: 10.1212/CON.0000000000000660
11. Agrawal S, Nadel S. Acute bacterial meningitis in infants and children: epidemiology and management. Paediatr Drugs. (2011) 13:385–400. doi: 10.2165/11593340-000000000-00000
12. PAHO/WHO. PCV Introduction. Available online at: https://www.paho.org/hq/index.php?option=com_content&view=article&id=1938:2009-pcv-intro-map&Itemid=1678&lang=en. (accessed October 12, 2021).
13. Dirección Redes en Salud Pública. Vigilancia por laboratorio de aislamientos invasores de Streptococcus pneumoniae Colombia 2006-2018 - SIREVA II. Colombia: Instituto Nacional de Salud (2019). Available online at: https://www.ins.gov.co/buscador-eventos/Informacin%20de%20laboratorio/Vigilancia%20por%20laboratorio%20S.%20pneumoniae%202006-2018.pdf (accessed October 20, 2021).
14. Stockmann C, Ampofo K, Byington CL, Filloux F, Hersh AL, Blaschke AJ, et al. Pneumococcal meningitis in children: epidemiology, serotypes, and outcomes from 1997–2010 in Utah. Pediatrics. (2013) 132:421–8. doi: 10.1542/peds.2013-0621
15. Kuti BP, Bello EO, Jegede TO, Olubosede O. Epidemiological, clinical and prognostic profile of childhood acute bacterial meningitis in a resource poor setting. J Neurosci Rural Pract. (2015) 6:549–57. doi: 10.4103/0976-3147.165424
16. González-Escartín E, Angulo López I, Ots Ruiz E, Martínez-Martínez L, Cabero Pérez MJ. Pneumococcal meningitis in Cantabria (Spain) in the pneumococcal conjugate vaccine era (2001–2015). Arch Argent Pediatr. (2017) 115:160–4. doi: 10.5546/aap.2017.eng.160
17. Curtis S, Stobart K, Vandermeer B, Simel DL, Klassen T. Clinical features suggestive of meningitis in children: a systematic review of prospective data. Pediatrics. (2010) 126:952–60. doi: 10.1542/peds.2010-0277
18. Peltola H, Pelkonen T, Roine I, Cruzeiro ML, Bernardino L. Predicting outcome of childhood bacterial meningitis with a single measurement of C-reactive protein. Pediatr Infect Dis J. (2016) 35:617–21. doi: 10.1097/INF.0000000000001133
19. Lummel N, Koch M, Klein M, Pfister HW, Brückmann H, Linn J. Spectrum and prevalence of pathological intracranial magnetic resonance imaging findings in acute bacterial meningitis. Clin Neuroradiol. (2016) 26:159–67. doi: 10.1007/s00062-014-0339-x
20. Oliveira CR, Morriss MC, Mistrot JG, Cantey JB, Doern CD, Sánchez PJ. Brain magnetic resonance imaging of infants with bacterial meningitis. J Pediatr. (2014) 165:134–9. doi: 10.1016/j.jpeds.2014.02.061
21. Calume ML. Informe de vigilancia epidemiológica de meningitis bacterianas en Colombia 2009 Final. Colombia: Insituto Nacional de Salud (2010). Available online at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/Meningitis%202009.pdf (accessed October 20, 2021).
22. Pinzón Gutiérrez C. Informe del evento meningitis bacteriana, hasta el periodo epidemiológico XIII del año 2012. Colombia: Insituto Nacional de Salud (2013). Available online at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/Meningitis%202012.pdf (accessed October 20, 2021).
23. Acosta Amador NM. Informe final meningitis bacteriana (MBA), Colombia, 2013. Colombia: Insituto Nacional de Salud (2014). Available online at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/Meningitis%202013.pdf (accessed October 20, 2021).
24. Reyes Hernández KJ. Informe final meningitis aguda bacteriana (MBA), Colombia, 2014. Colombia: Instituto Nacional de Salud (2015). Available online at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/Meningitis%202014.pdf (accessed October 20, 2021).
25. Alvarez Galindo JN. Informe de evento meningitis aguda bacteriana (MBA) hasta periodo epidemiológico XIII, Colombia, 2015. Colombia: Insituto Nacional de Salud (2016). Available online at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/Meningitis%202015.pdf (accessed October 20, 2021).
26. Salas HP. Informe del evento meningitis aguda bacteriana (MBA), hasta el periodo epidemiológico XIII, Colombia, 2016. Colombia: Insituto Nacional de Salud (2017). Available online at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/Meningitis%202016.pdf (accessed October 20, 2017).
27. Aparicio Fuentes SM. Informe de evento meningitis bacteriana y enfermedad meningocócica, Colombia, 2018. Colombia: Insituto Nacional de Salud (2019). Available online at: https://www.ins.gov.co/buscador-eventos/Informesdeevento/MENINGITIS%20BACTERIANA_2018.pdf (accessed October 20, 2021).
28. Guerrero MP, Romero AF, Luengas M, Dávalos DM, Mesa-Monsalve JG, Vivas-Trochez R, et al. Etiology and risk factors for admission to the pediatric intensive care unit in children with encephalitis in a developing country. Pediatr Infect Dis J. (2022). doi: 10.1097/INF.0000000000003637. [Epub ahead of print].
29. Nakamura T, Cohen AL, Schwartz S, Mwenda JM, Weldegebriel G, Biey JNM, et al. The global landscape of pediatric bacterial meningitis data reported to the world health organization-coordinated invasive bacterial vaccine-preventable disease surveillance network, 2014–2019. J Infect Dis. (2021) 224:S161–73. doi: 10.1093/infdis/jiab217
30. Camacho Moreno G, Imbachi LF, Leal AL, Moreno VM, Patiño JA, Gutiérrez IF, et al. Emergence of Streptococcus pneumoniae serotype 19A (Spn19A) in the pediatric population in Bogotá, Colombia as the main cause of invasive pneumococcal disease after the introduction of PCV10. Hum Vaccines Immunother. (2020) 16:2300–6. doi: 10.1080/21645515.2019.1710411
31. Severiche-Bueno DF, Severiche-Bueno DF, Bastidas A, Caceres EL, Silva E, Lozada J, et al. Burden of invasive pneumococcal disease (IPD) over a 10-year period in Bogotá, Colombia. Int J Infect Dis IJID Off Publ Int Soc Infect Dis. (2021) 105:32–9. doi: 10.1016/j.ijid.2021.02.031
32. Agudelo CI, Castañeda-Orjuela C, Brandileone MC de C, Echániz-Aviles G, Almeida SCG, Carnalla-Barajas MN, et al. The direct effect of pneumococcal conjugate vaccines on invasive pneumococcal disease in children in the Latin American and Caribbean region (SIREVA 2006-17): a multicentre, retrospective observational study. Lancet Infect Dis. (2021) 21:405–17. doi: 10.1016/S1473-3099(20)30489-8
33. Garcia Quesada M, Yang Y, Bennett JC, Hayford K, Zeger SL, Feikin DR, et al. Serotype distribution of remaining pneumococcal meningitis in the mature PCV10/13 period: findings from the PSERENADE project. Microorganisms. (2021) 9:738. doi: 10.3390/microorganisms9040738
34. Toda H, Satoh K, Komatsu M, Fukuda S, Nakamura T, Jikimoto T, et al. Laboratory surveillance of antimicrobial resistance and multidrug resistance among Streptococcus pneumoniae isolated in the Kinki region of Japan, 2001–2015. J Infect Chemother Off J Jpn Soc Chemother. (2018) 24:171–6. doi: 10.1016/j.jiac.2017.12.010
35. Ricketson LJ, Vanderkooi OG, Wood ML, Leal J, Kellner JD. Clinical features and outcomes of serotype 19A invasive pneumococcal disease in Calgary, Alberta. Can J Infect Dis Med Microbiol J Can Mal Infect Microbiol Medicale. (2014) 25:e71–75. doi: 10.1155/2014/196748
36. Camacho-Moreno G, Duarte C, García D, Calderón V, Maldonado LY, Castellar L, et al. Sentinel surveillance for bacterial pneumonia and meningitis in children under the age of 5 in a tertiary pediatric hospital in Colombia-2016. Biomed Rev Inst Nac Salud. (2021) 41:62–75. doi: 10.7705/biomedica.5658
37. Parra EL, Ramos V, Sanabria O, Moreno J. Serotype and genotype distribution among invasive Streptococcus pneumoniae isolates in Colombia, 2005–2010. PLoS ONE. (2014) 9:e84993. doi: 10.1371/journal.pone.0084993
38. Cassiolato AP, Almeida SCG, Andrade AL, Minamisava R, Brandileone MC de C. Expansion of the multidrug-resistant clonal complex 320 among invasive Streptococcus pneumoniae serotype 19A after the introduction of a ten-valent pneumococcal conjugate vaccine in Brazil. PLoS ONE. (2018) 13:e0208211. doi: 10.1371/journal.pone.0208211
39. Kaur R, Pham M, Yu KOA, Pichichero ME. Rising pneumococcal antibiotic resistance in the post-13-valent pneumococcal conjugate vaccine era in pediatric isolates from a primary care setting. Clin Infect Dis Off Publ Infect Dis Soc Am. (2021) 72:797–805. doi: 10.1093/cid/ciaa157
40. Andrejko K, Ratnasiri B, Lewnard JA. Association of pneumococcal serotype with susceptibility to antimicrobial drugs: A systematic review and meta-analysis. Clin Infect Dis. (2021) 75:131–40. doi: 10.1093/cid/ciab852
41. Wang Y, Liu X, Wang Y, Liu Q, Kong C, Xu G. Meta-analysis of adjunctive dexamethasone to improve clinical outcome of bacterial meningitis in children. Childs Nerv Syst ChNS Off J Int Soc Pediatr Neurosurg. (2018) 34:217–23. doi: 10.1007/s00381-017-3667-8
42. Shao M, Xu P, Liu J, Liu W, Wu X. The role of adjunctive dexamethasone in the treatment of bacterial meningitis: an updated systematic meta-analysis. Patient Prefer Adherence. (2016) 10:1243–9. doi: 10.2147/PPA.S109720
43. Klobassa DS, Zoehrer B, Paulke-Korinek M, Gruber-Sedlmayr U, Pfurtscheller K, Strenger V, et al. The burden of pneumococcal meningitis in Austrian children between 2001 and 2008. Eur J Pediatr. (2014) 173:871–8. doi: 10.1007/s00431-013-2260-8
44. Stuart JM. Editorial for the special issue: bacterial meningitis-epidemiology and vaccination. Microorganisms. (2021) 9:917. doi: 10.3390/microorganisms9050917
45. Gutiérrez-Tobar IF, Londoño-Ruiz JP, Mariño-Drews C, Beltrán-Higuera S, Camacho-Moreno G, Leal-Castro AL, et al. Epidemiological characteristics and serotype distribution of culture-confirmed pediatric pneumococcal pneumonia before and after PCV 10 introduction, a multicenter study in Bogota, Colombia, 2008-2019. Vaccine. (2022) 40:2875–83. doi: 10.1016/j.vaccine.2022.03.022
46. Sanchez-Marmolejo S, Rojas JP, Pacheco R, Camacho-Moreno G, Leal Castro AL, Patiño-Niño JA, et al. Clinical and microbiological profile of primary bacteremia caused by streptococcus pneumoniae infection in pediatric patients hospitalized at tertiary care centers of red neumocolombia. 2017-2019. Infectio. (2022) 26:222–7. doi: 10.22354/issn.2422-3794
Keywords: pneumococcal meningitis, pediatrics, infections, vaccines, microbiology, serotype
Citation: Farfán-Albarracín JD, Camacho-Moreno G, Leal AL, Patiño J, Coronell W, Gutiérrez IF, Beltrán S, Álvarez-Olmos MI, Mariño C, Barrero R, Rojas JP, Espinosa F, Arango-Ferreira C, Suarez MA, Trujillo M, López-Medina E, López P, Pinzón H, Ramos N, Moreno VM and Montañez A (2022) Changes in the incidence of acute bacterial meningitis caused by Streptococcus pneumoniae and the implications of serotype replacement in children in Colombia after mass vaccination with PCV10. Front. Pediatr. 10:1006887. doi: 10.3389/fped.2022.1006887
Received: 29 July 2022; Accepted: 30 August 2022;
Published: 23 September 2022.
Edited by:
Cecilia Perret, Pontificia Universidad Católica de Chile, ChileReviewed by:
Cecilia Gonzalez, Universidad del Desarrollo, ChileJose Maria Marimon, Osakidetza Hospital Universitario Donostia, Spain
Kaihu Yao, Beijing Children's Hospital, Capital Medical University, China
Copyright © 2022 Farfán-Albarracín, Camacho-Moreno, Leal, Patiño, Coronell, Gutiérrez, Beltrán, Álvarez-Olmos, Mariño, Barrero, Rojas, Espinosa, Arango-Ferreira, Suarez, Trujillo, López-Medina, López, Pinzón, Ramos, Moreno and Montañez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Germán Camacho-Moreno, gcamachom@unal.edu.co
†These authors have contributed equally to this work and share first authorship