
Effects of One-Stage Full-Mouth Scaling and Root Planing with Azithromycin on Diabetes and Periodontal Disease: A Randomized Controlled Trial
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
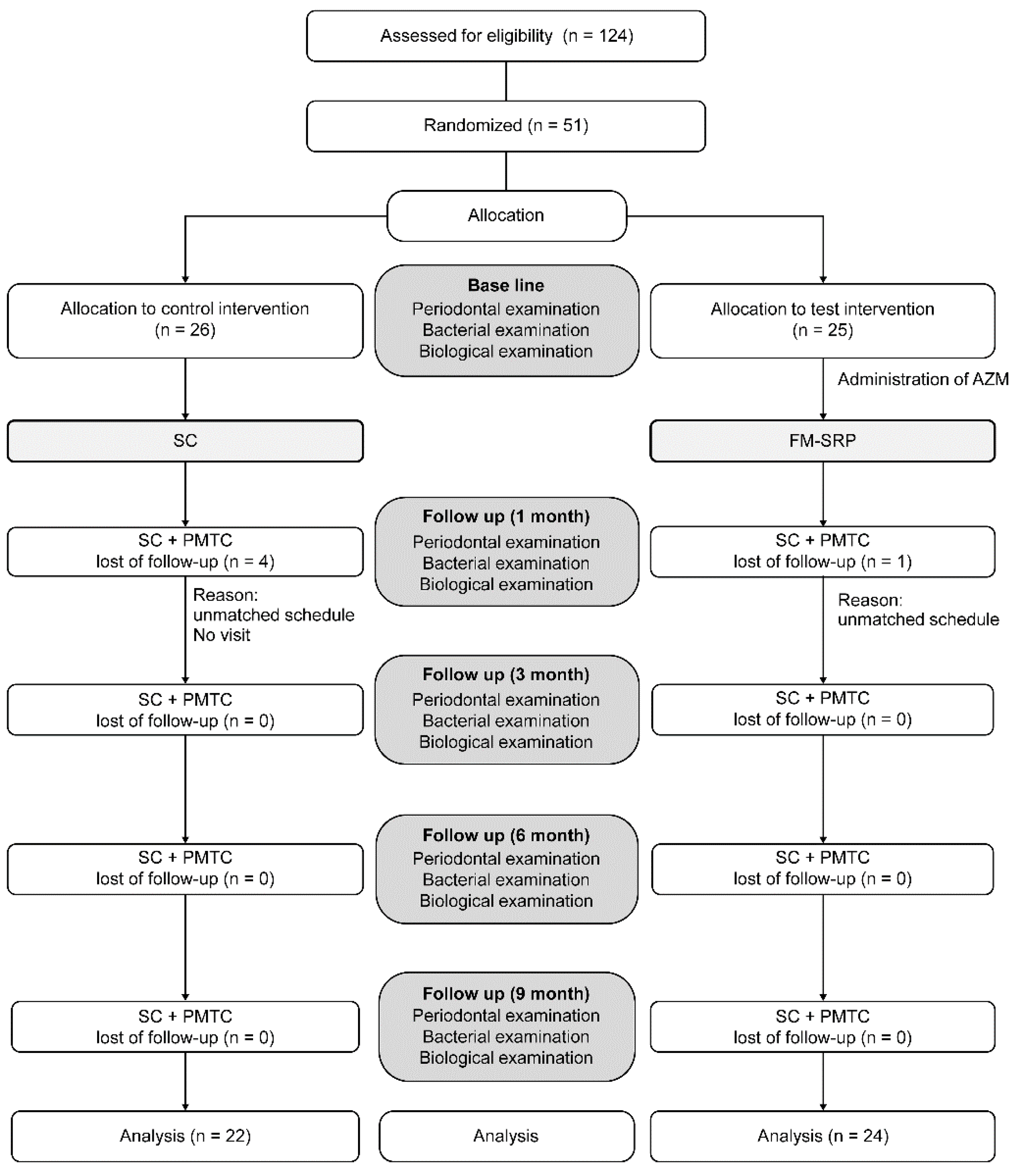
2.2. Randomization and Allocation Concealment
2.3. Clinical Protocol
2.4. Clinical Examination
2.5. Bacteriological Examination
2.6. Biochemical Examinations
2.7. Statistical Analysis
3. Results
3.1. Clinical Parameters
3.2. Bacteriological Examination
3.3. Biochemical Examinations
3.3.1. HbA1c
3.3.2. hs-CRP
3.3.3. TNF-α
3.3.4. IL-6
3.3.5. MCP-1
3.4. BMI
3.5. Correlation among HbA1c, Inflammatory Cytokines, and Clinical Parameters
3.6. Correlation with Nine-Month Changes in the FM-SRP Group and the Control Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Löe, H. Periodontal disease. The sixth complication of diabetes mellitus. Diabetes Care 1993, 16, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Chávarry, N.G.; Vettore, M.V.; Sansone, C.; Sheiham, A. The relationship between diabetes mellitus and destructive periodontal disease: A meta-analysis. Oral. Health Prev. Dent. 2009, 7, 107–127. [Google Scholar] [PubMed]
- Nelson, R.G.; Shlossman, M.; Budding, L.M.; Pettitt, D.J.; Saad, M.F.; Genco, R.J.; Knowler, W.C. Periodontal disease and NIDDM in pima Indians. Diabetes Care 1990, 13, 836–840. [Google Scholar] [CrossRef] [PubMed]
- Taylor, G.W.; Burt, B.A.; Becker, M.P.; Genco, R.J.; Shlossman, M. Glycemic control and alveolar bone loss progression in type 2 diabetes. Ann. Periodontol. 1998, 3, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Taylor, G.W.; Burt, B.A.; Becker, M.P.; Genco, R.J.; Shlossman, M.; Knowler, W.C.; Pettitt, D.J. Non-insulin dependent diabetes mellitus and alveolar bone loss progression over 2 years. J. Periodontol. 1998, 69, 76–83. [Google Scholar] [CrossRef]
- Demmer, R.T.; Desvarieux, M.; Holtfreter, B.; Jacobs Jr, D.R.; Wallaschofski, H.; Nauck, M.; Völzke, H.; Kocher, T. Periodontal status and A1c change: Longitudinal results from the study of health in Pomerania (SHIP). Diabetes Care 2010, 33, 1037–1043. [Google Scholar] [CrossRef]
- Demmer, R.T.; Squillaro, A.; Papapanou, P.N.; Rosenbaum, M.; Friedewald, W.T.; Jacobs Jr, D.R.; Desvarieux, M. Periodontal infection, systemic inflammation, and insulin resistance: Results from the continuous National Health and Nutrition Examination Survey (NHANES) 1999–2004. Diabetes Care 2012, 35, 2235–2242. [Google Scholar] [CrossRef]
- Saremi, A.; Nelson, R.G.; Tulloch-Reid, M.; Hanson, R.L.; Sievers, M.L.; Taylor, G.W.; Shlossman, M.; Bennett, P.H.; Genco, R.; Knowler, W.C. Periodontal disease and mortality in type 2 diabetes. Diabetes Care 2005, 28, 27–32. [Google Scholar] [CrossRef]
- Sun, W.L.; Chen, L.L.; Zhang, S.Z.; Wu, Y.M.; Ren, Y.Z.; Qin, G.M. Inflammatory cytokines, adiponectin, insulin resistance and metabolic control after periodontal intervention in patients with type 2 diabetes and chronic periodontitis. Intern. Med. 2011, 50, 1569–1574. [Google Scholar] [CrossRef]
- Munenaga, Y.; Hiroshima Study Group; Yamashina, T.; Tanaka, J.; Nishimura, F. Improvement of glycated hemoglobin in Japanese subjects with type 2 diabetes by resolution of periodontal inflammation using adjunct topical antibiotics: Results from the Hiroshima Study. Diabetes Res. Clin. Pract. 2013, 100, 53–60. [Google Scholar] [CrossRef]
- Simpson, T.C.; Needleman, I.; Wild, S.H.; Moles, D.R.; Mills, E.J. Treatment of periodontal disease for glycaemic control in people with diabetes. Cochrane Database Syst. Rev. 2010, 5, CD004714. [Google Scholar]
- Navarro-Sanchez, A.B.; Faria-Almeida, R.; Bascones-Martinez, A. Effect of non-surgical periodontal therapy on clinical and immunological response and glycaemic control in type 2 diabetic patients with moderate periodontitis. J. Clin. Periodontol. 2007, 34, 835–843. [Google Scholar] [CrossRef] [PubMed]
- Engebretson, S.P.; Hyman, L.G.; Michalowicz, B.S.; Schoenfeld, E.R.; Gelato, M.C.; Hou, W.; Seaquist, E.R.; Reddy, M.S.; Lewis, C.E.; Oates, T.W.; et al. The effect of nonsurgical periodontal therapy on hemoglobin A1c levels in persons with type 2 diabetes and chronic periodontitis: A randomized clinical trial. JAMA 2013, 310, 2523–2532. [Google Scholar] [CrossRef]
- Chen, L.; Luo, G.; Xuan, D.; Wei, B.; Liu, F.; Li, J.; Zhang, J. Effects of non-surgical periodontal treatment on clinical response, serum inflammatory parameters, and metabolic control in patients with type 2 diabetes: A randomized study. J. Periodontol. 2012, 83, 435–443. [Google Scholar] [CrossRef]
- Sumida, S.; Ishihara, K.; Kishi, M.; Okuda, K. Transmission of periodontal disease-associated bacteria from teeth to osseointegrated implant regions. Int. J. Oral Maxillofac. Implants 2002, 17, 696–702. [Google Scholar] [PubMed]
- Gladue, R.P.; Bright, G.M.; Isaacson, R.E.; Newborg, M.F. In vitro and in vivo uptake of azithromycin (CP-62, 993) by phagocytic cells: Possible mechanism of delivery and release at sites of infection. Antimicrob. Agents Chemother. 1989, 33, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Foulds, G.; Shepard, R.M.; Johnson, R.B. The pharmaco- kinetics of azithromycin in human serum and tissue. J. Antimicrob. Chemother. 1990, 25 (Suppl. A), 73–82. [Google Scholar] [CrossRef] [PubMed]
- McDonald, P.J.; Pruul, H. Phagocytic uptake and transport of azithromycin. Eur. J. Clin. Microbiol. Infect. Dis. 1991, 10, 828–833. [Google Scholar] [CrossRef]
- Schentag, J.J.; Ballow, C.H. Tissue-directed pharmacokinetics. Am. J. Med. 1991, 91, 5–11. [Google Scholar] [CrossRef]
- Gomi, K.; Yashima, A.; Nagano, T.; Kanazashi, M.; Maeda, N.; Arai, T. Effects of full-mouth scaling and root planing in conjunction with systemically administered azithromycin. J. Periodontol. 2007, 78, 422–429. [Google Scholar] [CrossRef]
- Yashima, A.; Gomi, K.; Maeda, N.; Arai, T. One-stage full-mouth versus partial-mouth scaling and root planing during the effective half-life of systemically administered azithromycin. J. Periodontol. 2009, 80, 1406–1413. [Google Scholar] [CrossRef] [PubMed]
- Nesse, W.; Abbas, F.; van der Ploeg, I.; Spijkervet, F.K.; Dijkstra, P.U.; Vissink, A. Periodontal inflamed surface area:quantifying inflammatory burden. J. Clin. Periodontol. 2008, 35, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Vissink, A.; Abbas, F.; Dijkstra, P.; Spijkervet, F.K.L.; Nesse, W. Parsprototo. Info. Available online: https://www.parsprototo.info/ (accessed on 25 February 2022).
- Vissink, A.; Abbas, F.; Dijkstra, P.; Spijkervet, F.K.L.; Nesse, W. Calculate PISA Using Probing Pocket Depth. Available online: https://parsprototo.info/docs/PISA_PPD.xls (accessed on 25 February 2022).
- Tadokoro, K.; Yamaguchi, T.; Kawamura, K.; Shimizu, H.; Egashira, T.; Minabe, M.; Yoshino, T.; Oguchi, H. Rapid quantification of periodontitis-related bacteria using a novel modification of Invader PLUS technologies. Microbiol. Res. 2010, 165, 43–49. [Google Scholar] [CrossRef]
- Tada, A.; Takeuchi, H.; Shimizu, H.; Tadokoro, K.; Tanaka, K.; Kawamura, K.; Yamaguchi, T.; Egashira, T.; Nomura, Y.; Hanada, N. Quantification of periodontopathic bacteria in saliva using the invader assay. Jpn. J. Infect. Dis. 2012, 65, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Mealey, B.L.; Oates, T.W.; American Academy of Periodontology. Diabetes mellitus and periodontal diseases. J. Periodontol. 2006, 77, 1289–1303. [Google Scholar] [CrossRef]
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontol 2000 2013, 62, 59–94. [Google Scholar] [CrossRef]
- Emrich, L.J.; Shlossman, M.; Genco, R.J. Periodontal disease in non-insulin-dependent diabetes mellitus. J. Periodontol. 1991, 62, 123–131. [Google Scholar] [CrossRef]
- Borgnakke, W.S.; Glick, M.; Genco, R.J. Periodontitis: The canary in the coal mine. J. Am. Dent. Assoc. 2013, 144, 764–766. [Google Scholar] [CrossRef]
- Grossi, S.G.; Skrepcinski, F.B.; DeCaro, T.; Robertson, D.C.; Ho, A.W.; Dunford, R.G.; Genco, R.J. Treatment of periodontal disease in diabetics reduces glycated hemoglobin. J. Periodontol. 1997, 68, 713–719. [Google Scholar] [CrossRef]
- O’Connell, P.A.; Taba, M.; Nomizo, A.; Foss-Freitas, M.C.; Suaid, F.A.; Uyemura, S.A.; Trevisan, G.L.; Novaes, A.B.; Souza, S.L.; Palioto, D.B.; et al. Effects of periodontal therapy on glycemic control and inflammatory markers. J. Periodontol. 2008, 79, 774–783. [Google Scholar] [CrossRef]
- Rodrigues, D.C.; Taba, M.J.; Novaes, A.B.; Souza, S.L.; Grisi, M.F. Effect of non-surgical periodontal therapy on glycemic control in patients with type 2 diabetes mellitus. J. Periodontol. 2003, 74, 1361–1367. [Google Scholar] [CrossRef] [PubMed]
- Miranda, T.S.; Feres, M.; Perez-Chaparro, P.J.; Faveri, M.; Figueiredo, L.C.; Tamashiro, N.S.; Bastos, M.F.; Duarte, P.M. Metronidazole and amoxicillin as adjuncts to scaling and root planing for the treatment of type 2 diabetic subjects with periodontitis: 1-year outcomes of a randomized placebo-controlled clinical trial. J. Clin. Periodontol. 2014, 41, 890–899. [Google Scholar] [CrossRef] [PubMed]
- Campus, G.; Salem, A.; Uzzau, S.; Baldoni, E.; Tonolo, G. Diabetes and periodontal disease: A case-control study. J. Periodontol. 2005, 76, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Mashimo, P.A.; Yamamoto, Y.; Slots, J.; Park, B.H.; Genco, R.J. The periodontal microflora of juvenile diabetics. Culture, immunofluorescence, and serum antibody studies. J. Periodontol. 1983, 54, 420–430. [Google Scholar] [CrossRef] [PubMed]
- Thorstensson, H.; Dahlén, G.; Hugoson, A. Some suspected periodontopathogens and serum antibody response in adult long-duration insulin-dependent diabetics. J. Clin. Periodontol. 1995, 22, 449–458. [Google Scholar] [CrossRef]
- Zambon, J.J.; Reynolds, H.; Fisher, J.G.; Shlossman, M.; Dunford, R.; Genco, R.J. Microbiological and immunological studies of adult periodontitis in patients with noninsulin-dependent diabetes mellitus. J. Periodontol. 1988, 59, 23–31. [Google Scholar] [CrossRef]
- Sbordone, L.; Ramaglia, L.; Barone, A.; Ciaglia, R.N.; Tenore, A.; Iacono, V.J. Periodontal status and selected cultivable anaerobic microflora of insulin-dependent juvenile diabetics. J. Periodontol. 1995, 66, 452–461. [Google Scholar] [CrossRef]
- Papageorgiou, S.N.; Reichert, C.; Jäger, A.; Deschner, J. Effect of overweight/obesity on response to periodontal treatment: Systematic review and a meta-analysis. J. Clin. Periodontol. 2015, 42, 247–261. [Google Scholar] [CrossRef]
- Geisinger, M.L.; Michalowicz, B.S.; Hou, W.; Schoenfeld, E.; Gelato, M.; Engebretson, S.P.; Reddy, M.S.; Hyman, L. Systemic inflammatory biomarkers and their association with periodontal and diabetes-related factors in the diabetes and periodontal therapy trial, A randomized controlled trial. J. Periodontol. 2016, 87, 900–913. [Google Scholar] [CrossRef]
- D’Aiuto, F.; Gkranias, N.; Bhowruth, D.; Khan, T.; Orlandi, M.; Suvan, J.; Masi, S.; Tsakos, G.; Hurel, S.; Hingorani, A.D.; et al. Systemic effects of periodontitis treatment in patients with type 2 diabetes: A 12 month, single-centre, investigator-masked, randomised trial. Lancet Diabetes Endocrinol. 2018, 6, 954–965. [Google Scholar] [CrossRef]
- Engebretson, S.; Kocher, T. Evidence that periodontal treatment improves diabetes outcomes: A systematic review and meta-analysis. J. Clin. Periodontol. 2013, 40, S153–S163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwamoto, Y.; Nishimura, F.; Nakagawa, M.; Sugimoto, H.; Shikata, K.; Makino, H.; Fukuda, T.; Tsuji, T.; Iwamoto, M.; Murayama, Y. The effect of antimicrobial periodontal treatment on circulating tumor necrosis factor-alpha and glycated hemoglobin level in patients with type 2 diabetes. J. Periodontol. 2001, 72, 774–778. [Google Scholar] [CrossRef] [PubMed]
- Lechleitner, M.; Herold, M.; Dzien-Bischinger, C.; Hoppichler, F.; Dzien, A. Tumour necrosis factor-alpha plasma levels in elderly patients with type 2 diabetes mellitus-observations over 2 years. Diabet. Med. 2002, 19, 949–953. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Mizuarai, S.; Araki, H.; Mashiko, S.; Ishihara, A.; Kanatani, A.; Itadani, H.; Kotani, H. Adiposity elevates plasma MCP- 1 levels leading to the increased CD11b-positive monocytes in mice. J. Biol. Chem. 2003, 278, 46654–46660. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| FM-SRP (n = 24) | Control (n = 22) | p Value | |
|---|---|---|---|
| Age | 66.7 ± 13.9 (36–88) | 63.5 ± 12.2 (36–82) | 0.4121 |
| Sex (male/female) | 24 (9/15) | 22 (8/14) | 0.9364 |
| HbA1c (%) | 7.4 ± 0.4 (6.5–8.2) | 7.3 ± 0.6 (6.7–9.2) | 0.067 |
| BMI (kg/m2) | 26.3 ± 4.8 (20.7–40.6) | 24.8 ± 5.3 (16.3–40.9) | 0.3673 |
| PPD (mm) | 3.6 ± 0.5 | 3.5 ± 0.3 | 0.6189 |
| BOP (%) | 48.2 ± 15.4 | 44.6 ± 10.8 | 0.448 |
| PISA (mm2) | 884.9 ± 395.9 | 884.4 ± 235.1 | 0.6207 |
| hs-CRP (mg/dL) | 0.19 ± 0.32 | 0.08 ± 0.07 | 0.2222 |
| TNF-α (pg/mL) | 1.1 ± 0.5 | 0.9 ± 0.3 | 0.1183 |
| IL-6 (pg/mL) | 2.3 ± 0.6 | 2.2 ± 0.6 | 0.6199 |
| MCP-1 (pg/mL) | 120.0 ± 45.7 | 124.9 ± 50.7 | 0.5674 |
| Time | FM-SRP | p Value (vs. BL) | Control | p Value (vs. BL) | p Value (FM-SRP vs. Control) | |
|---|---|---|---|---|---|---|
| PPD (mm) | BL | 3.6 ± 0.5 | - | 3.5 ± 0.3 | - | 0.6189 |
| 1 M | 2.5 ± 0.3 | <0.0001 * | 3.3 ± 0.3 | 0.0097 | <0.0001 * | |
| 3 M | 2.3 ± 0.2 | <0.0001 * | 3.4 ± 0.3 | 0.0321 | <0.0001 * | |
| 6 M | 2.5 ± 0.2 | <0.0001 * | 3.3 ± 0.3 | 0.0206 | <0.0001 * | |
| 9 M | 2.5 ± 0.2 | <0.0001 * | 3.4 ± 0.3 | 0.054 | <0.0001 * | |
| BOP (%) | BL | 48.2 ± 15.4 | - | 44.6 ± 10.8 | - | 0.448 |
| 1 M | 9.5 ± 7.9 | <0.0001 * | 43.4 ± 9.2 | 0.0826 | <0.0001 * | |
| 3 M | 6.9 ± 5.6 | <0.0001 * | 43.2 ± 9.3 | 0.0289 | <0.0001 * | |
| 6 M | 6.4 ± 5.5 | <0.0001 * | 43.8 ± 9.8 | 0.2377 | <0.0001 * | |
| 9 M | 6.1 ± 4.7 | <0.0001 * | 43.5 ± 9.5 | 0.4196 | <0.0001 * | |
| PISA (mm2) | BL | 884.9 ± 395.9 | - | 884.4 ± 235.1 | - | 0.6207 |
| 1 M | 100.5 ± 92.5 | <0.0001 * | 821.4 ± 227.6 | 0.0074 | <0.0001 * | |
| 3 M | 94.1 ± 118.0 | <0.0001 * | 830.3 ± 228.9 | 0.0132 | <0.0001 * | |
| 6 M | 98.7 ± 131.8 | <0.0001 * | 828.3 ± 206.6 | 0.0057 | <0.0001 * | |
| 9 M | 66.9 ± 53.6 | <0.0001 * | 833.9 ± 197.6 | 0.0703 | <0.0001 * |
| Time | FM-SRP | p Value (vs. BL) | Control | p Value (vs. BL) | p Value (FM-SRP vs. Control) | |
|---|---|---|---|---|---|---|
| P. gingivalis | BL | 2.1 ± 1.1 | - | 1.6 ± 1.0 | - | 0.1799 |
| (log10) | 1 M | 1.0 ± 0 | <0.0001 * | 1.8 ± 2.0 | 0.2374 | 0.0014 * |
| 3 M | 1.1 ± 0.2 | <0.0001 * | 1.6 ± 0.9 | 0.4767 | 0.0308 * | |
| 6 M | 1.2 ± 0.5 | 0.0002 * | 1.7 ± 1.0 | 0.9463 | 0.0122 * | |
| 9 M | 1.1 ± 0.4 | 0.0002 * | 1.9 ± 1.1 | 0.3565 | 0.0167 * | |
| T. denticola | BL | 2.1 ± 0.9 | - | 1.9 ± 0.8 | - | 0.315 |
| (log10) | 1 M | 1.1 ± 0.3 | <0.0001 * | 1.7 ± 0.9 | 0.316 | 0.0015 * |
| 3 M | 1.2 ± 0.4 | <0.0001 * | 1.8 ± 1.0 | 0.6392 | 0.0024 * | |
| 6 M | 1.1 ± 0.3 | <0.0001 * | 1.8 ± 0.8 | 0.4297 | <0.0001 * | |
| 9 M | 1.1 ± 0.4 | 0.0002 * | 1.8 ± 0.9 | 0.5789 | 0.0026 * | |
| T. forsythia | BL | 1.8 ± 0.7 | - | 1.6 ± 0.7 | - | 0.2765 |
| (log10) | 1 M | 1.1 ± 0.2 | <0.0001 * | 1.6 ± 0.7 | 0.8748 | 0.0009 * |
| 3 M | 1.2 ± 0.4 | 0.0023 * | 1.7 ± 0.6 | 0.1812 | 0.0021 * | |
| 6 M | 1.2 ± 0.5 | 0.0027 * | 1.9 ± 0.7 | 0.1776 | 0.0003 * | |
| 9 M | 1.3 ± 0.5 | 0.0032 * | 1.9 ± 0.7 | 0.1373 | 0.0009 * | |
| P. intermedia | BL | 1.4 ± 0.6 | - | 1.3 ± 0.4 | - | 0.5936 |
| (log10) | 1 M | 1.1 ± 0.3 | 0.0013 * | 1.7 ± 2.0 | 0.9195 | 0.0036 * |
| 3 M | 1.1 ± 0.2 | 0.0013 * | 1.5 ± 1.0 | 0.2264 | 0.0089 * | |
| 6 M | 1.1 ± 0.2 | 0.0013 * | 1.3 ± 0.4 | 0.6485 | 0.0236 * | |
| 9 M | 1.1 ± 0.2 | 0.0013 * | 1.3 ± 0.4 | 0.4151 | 0.0132 * | |
| A. actinomycetemcomitans | BL | 1.0 ± 0.10 | - | 1.0 ± 0.12 | - | 0.9104 |
| (log10) | 1 M | 1.0 ± 0 | 0.1618 | 1.5 ± 1.9 | 0.54 | 0.1353 |
| 3 M | 1.0 ± 0 | 0.1618 | 1.1 ± 0.4 | 0.1622 | 0.1353 | |
| 6 M | 1.0 ± 0 | 0.1618 | 1.0 ± 0.02 | 0.1622 | 0.2963 | |
| 9 M | 1.0 ± 0.2 | 0.9768 | 1.0 ± 0.09 | 0.1622 | 0.9752 |
| Time | FM-SRP | p Value (vs. BL) | Control | p Value (vs. BL) | p Value (FM-SRP vs. Control) | |
|---|---|---|---|---|---|---|
| HbA1c (%) | BL | 7.4 ± 0.4 | - | 7.3 ± 0.6 | - | 0.067 |
| 1 M | 7.3 ± 0.4 | 0.0017 * | 7.4 ± 0.7 | 0.2147 | 0.9121 | |
| 3 M | 7.2 ± 0.4 | 0.0005 * | 7.5 ± 0.9 | 0.0363 | 0.275 | |
| 6 M | 7.1 ± 0.5 | <0.0001 * | 7.6 ± 1.0 | 0.0322 | 0.0291 * | |
| 9 M | 7.1 ± 0.5 | 0.0001 * | 7.4 ± 0.7 | 0.0808 | 0.0552 | |
| hs-CRP | BL | 0.19 ± 0.32 | - | 0.08 ± 0.07 | - | 0.2222 |
| (mg/dL) | 1 M | 0.06 ± 0.06 | <0.0001 * | 0.10 ± 0.11 | 0.1836 | 0.0441 * |
| 3 M | 0.09 ± 0.09 | 0.0101 | 0.07 ± 0.09 | 0.3668 | 0.5236 | |
| 6 M | 0.08 ± 0.07 | 0.0030 * | 0.07 ± 0.10 | 0.2583 | 0.6129 | |
| 9 M | 0.07 ± 0.08 | <0.0001 * | 0.12 ± 0.26 | 0.3668 | 0.7414 | |
| TNF-α | BL | 1.1 ± 0.5 | - | 0.9 ± 0.3 | - | 0.1183 |
| (pg/mL) | 1 M | 0.76 ± 0.2 | 0.0002 * | 0.9 ± 0.3 | 1 | 0.0453 * |
| 3 M | 0.8 ± 0.3 | 0.0019 * | 0.9 ± 0.3 | 0.2314 | 0.7001 | |
| 6 M | 0.9 ± 0.2 | 0.0396 | 0.9 ± 0.3 | 0.8506 | 0.8258 | |
| 9 M | 0.9 ± 0.2 | 0.0111 | 0.9 ± 0.3 | 0.3493 | 0.7833 | |
| IL-6 (pg/mL) | BL | 2.3 ± 0.6 | - | 2.2 ± 0.6 | - | 0.6199 |
| 1 M | 1.8 ± 0.7 | 0.0045 * | 2.3 ± 0.9 | 0.826 | 0.0185 * | |
| 3 M | 2.1 ± 0.6 | 0.033 | 2.1 ± 0.6 | 0.3578 | 0.7493 | |
| 6 M | 2.2 ± 0.8 | 1 | 2.4 ± 0.6 | 0.2934 | 0.3633 | |
| 9 M | 2.1 ± 0.6 | 0.4928 | 2.1 ± 0.6 | 0.9374 | 0.5814 | |
| MCP-1 | BL | 120.0 ± 45.7 | - | 124.9 ± 50.7 | - | 0.5674 |
| (pg/mL) | 1 M | 118.2 ± 36.1 | 0.1527 | 120.4 ± 51.9 | 0.4779 | 0.373 |
| 3 M | 113.9 ± 36.4 | 0.879 | 130.3 ± 65.6 | 0.5709 | 0.5748 | |
| 6 M | 123.3 ± 72.2 | 0.4693 | 123.7 ± 49.7 | 0.8754 | 0.668 | |
| 9 M | 107.5 ± 32.8 | 0.3716 | 116.7 ± 41.0 | 0.5176 | 0.2436 | |
| BMI | BL | 26.3 ± 4.8 | - | 24.8 ± 5.3 | - | 0.3673 |
| (kg/m2) | 1 M | 26.4 ± 4.8 | 0.0957 | 24.8 ± 5.1 | 0.5817 | 0.3276 |
| 3 M | 26.3 ± 4.9 | 0.4172 | 24.8 ± 5.1 | 0.7188 | 0.3331 | |
| 6 M | 26.2 ± 4.9 | 0.4331 | 24.5 ± 5.1 | 0.2953 | 0.3021 | |
| 9 M | 26.2 ± 4.9 | 0.7971 | 24.5 ± 5.1 | 0.1322 | 0.3168 |
| Biomarker Measurements | Periodontal Clinical Measurements | |||||||
|---|---|---|---|---|---|---|---|---|
| HbA1c | hs-CRP | TNF-α | IL-6 | MCP-1 | PPD | BOP | PISA | |
| Correlation p Value | (%) | (mg/dL) | (pg/mL) | (pg/mL) | (pg/mL) | (mm) | (%) | (mm2) |
| HbA1c (%) | - | |||||||
| hs-CRP (mg/dL) | 0.5683 | - | ||||||
| <0.0001 * | ||||||||
| TNF-α (pg/mL) | 0.4823 | 0.4681 | - | |||||
| 0.0007 * | 0.0010 * | |||||||
| IL-6 (pg/mL) | 0.2316 | 0.5416 | 0.5111 | - | ||||
| 0.1215 | 0.0001 * | 0.0003 * | ||||||
| MCP-1 (pg/mL) | 0.005 | −0.068 | 0.0452 | −0.0132 | - | |||
| 0.9737 | 0.6536 | 0.7657 | 0.9303 | |||||
| PPD (mm) | 0.5629 | 0.3157 | 0.3461 | 0.0507 | 0.0477 | - | ||
| <0.0001 * | 0.0326 | 0.0185 | 0.738 | 0.753 | ||||
| BOP (%) | 0.5061 | 0.3966 | 0.397 | 0.2429 | −0.0072 | 0.7823 | - | |
| 0.0003 * | 0.0064 | 0.0063 | 0.1038 | 0.9624 | <0.0001 * | |||
| PISA (mm2) | 0.5963 | 0.4738 | 0.4763 | 0.2608 | −0.0163 | 0.8242 | 0.9353 | - |
| <0.0001 * | 0.0009 * | 0.0008 * | 0.0801 | 0.9145 | <0.0001 * | <0.0001 * | ||
| Biomarker Measurements | Periodontal Clinical Measurements | |||||||
|---|---|---|---|---|---|---|---|---|
| HbA1c | hs-CRP | TNF-α | IL-6 | MCP-1 | PPD | BOP | PISA | |
| Correlation p Value | (%) | (mg/dL) | (pg/mL) | (pg/mL) | (pg/mL) | (mm) | (%) | (mm2) |
| HbA1c (%) | - | |||||||
| hs-CRP (mg/dL) | 0.5995 | - | ||||||
| 0.0020 * | ||||||||
| TNF-α (pg/mL) | 0.6265 | 0.5997 | - | |||||
| 0.0011 * | 0.002 | |||||||
| IL-6 (pg/mL) | 0.4632 | 0.5556 | 0.6806 | - | ||||
| 0.0226 | 0.0048 | 0.0003 * | ||||||
| MCP-1 (pg/mL) | −0.2718 | −0.3011 | −0.1872 | −0.2157 | - | |||
| 0.1989 | 0.1527 | 0.3812 | 0.3114 | |||||
| PPD (mm) | 0.0967 | 0.2117 | 0.2647 | −0.0476 | −0.1439 | - | ||
| 0.6529 | 0.3208 | 0.2112 | 0.8252 | 0.5024 | ||||
| BOP (%) | 0.101 | 0.3296 | 0.2857 | 0.3287 | −0.2106 | 0.0355 | - | |
| 0.6386 | 0.1158 | 0.1759 | 0.1168 | 0.3232 | 0.8692 | |||
| PISA (mm2) | 0.4163 | 0.613 | 0.5801 | 0.3777 | −0.2454 | 0.2121 | 0.6809 | - |
| 0.043 | 0.0014 * | 0.0030 * | 0.0688 | 0.2477 | 0.3197 | 0.0003 * | ||
| Biomarker Measurements | Periodontal Clinical Measurements | |||||||
|---|---|---|---|---|---|---|---|---|
| HbA1c | hs-CRP | TNF-α | IL-6 | MCP-1 | PPD | BOP | PISA | |
| Correlation p Value | (%) | (mg/dL) | (pg/mL) | (pg/mL) | (pg/mL) | (mm) | (%) | (mm2) |
| HbA1c (%) | - | |||||||
| hs-CRP (mg/dL) | 0.3187 | - | ||||||
| 0.1483 | ||||||||
| TNF-α (pg/mL) | −0.0603 | 0.0543 | - | |||||
| 0.79 | 0.8104 | |||||||
| IL-6 (pg/mL) | −0.0006 | 0.4608 | 0.3428 | - | ||||
| 0.998 | 0.0309 | 0.1184 | ||||||
| MCP-1 (pg/mL) | 0.1211 | 0.0781 | 0.4395 | 0.2158 | - | |||
| 0.5912 | 0.7299 | 0.0407 | 0.3348 | |||||
| PPD (mm) | 0.2595 | −0.2422 | −0.2454 | −0.0434 | 0.1627 | - | ||
| 0.2435 | 0.2775 | 0.2711 | 0.8478 | 0.4694 | ||||
| BOP (%) | 0.0466 | −0.0155 | −0.1414 | 0.355 | −0.0034 | 0.2917 | - | |
| 0.837 | 0.9452 | 0.5303 | 0.1049 | 0.988 | 0.1878 | |||
| PISA (mm2) | 0.0822 | 0.0028 | −0.135 | 0.3774 | −0.0164 | 0.4531 | 0.8257 | - |
| 0.7161 | 0.99 | 0.5491 | 0.0834 | 0.9423 | 0.0342 | <0.0001 * | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Komatsu, S.; Oshikiri, S.; Nagano, T.; Yashima, A.; Matsushima, Y.; Shirakawa, S.; Komatsu, K.; Mokubo, A.; Gomi, K. Effects of One-Stage Full-Mouth Scaling and Root Planing with Azithromycin on Diabetes and Periodontal Disease: A Randomized Controlled Trial. Antibiotics 2022, 11, 1266. https://doi.org/10.3390/antibiotics11091266
Komatsu S, Oshikiri S, Nagano T, Yashima A, Matsushima Y, Shirakawa S, Komatsu K, Mokubo A, Gomi K. Effects of One-Stage Full-Mouth Scaling and Root Planing with Azithromycin on Diabetes and Periodontal Disease: A Randomized Controlled Trial. Antibiotics. 2022; 11(9):1266. https://doi.org/10.3390/antibiotics11091266
Chicago/Turabian StyleKomatsu, Sho, Shotaro Oshikiri, Takatoshi Nagano, Akihiro Yashima, Yuji Matsushima, Satoshi Shirakawa, Katsutoshi Komatsu, Akiko Mokubo, and Kazuhiro Gomi. 2022. "Effects of One-Stage Full-Mouth Scaling and Root Planing with Azithromycin on Diabetes and Periodontal Disease: A Randomized Controlled Trial" Antibiotics 11, no. 9: 1266. https://doi.org/10.3390/antibiotics11091266