Four decades of developmental dysplastic hip screening according to Graf: What have we learned?
 Sebastian G. Walter1*†
Sebastian G. Walter1*†  Robert Ossendorff2† Ayla Yagdiran1 Jan Hockmann1 Rahel Bornemann2
Robert Ossendorff2† Ayla Yagdiran1 Jan Hockmann1 Rahel Bornemann2  Sonja Placzek3
Sonja Placzek3- 1Department for Orthopedic Surgery and Traumatology, University Hospital Cologne, Cologne, Germany
- 2Department for Orthopedic Surgery and Traumatology, University Hospital Bonn, Bonn, Germany
- 3Medical Service of the Health Funds (MDK), Cologne, Germany
Purpose: Sonographic hip examination according to Graf is widely accepted standard for diagnosing developmental dysplastic hips (DDH) but it is criticized for alleged intra- and interobserver variations. This review was conducted to evaluate whether objective quality criteria according to the Graf method are fulfilled within scientific literature.
Methods: A systematic literature search on Pubmed was performed using the search string: [(DDH) OR (Hip dysplasia)] AND (Graf). Studies suitable by title, abstract, manuscript, containing an image of sonographic hip examination and online accessibility were included into analysis.
Results: 131 studies were included into final analysis. Only 68 (51.9%) presented correct sonographic images according Graf’s criteria. 98 (74.8%) studies plotted alpha-angles (angle between bony roof line and base line) but only 85 (64.8%) studies beta-angles (angle between cartilage roof line and base line). Studies were contributed from 25 countries.
Conclusion: Assumingly, skepticism regarding the Graf method is based on user errors and insufficient application of the Graf quality assessment algorithm resulting in high intra- and interobserver variations. When performed correctly, the Graf method is of high diagnostic value.
Introduction
It was in 1983 when Graf introduced his technique for examination of infantile hips by ultrasound and he was confronted with skepticism from the orthopedic community. Nevertheless, his scientific approach proved to be of high diagnostic value (1, 2). Notably, the Graf method prevailed in the scientific debate and clinical practice over other ultrasound examination protocols and modifications (3, 4). Subsequently the ultrasound examination according to Graf became standard within German-speaking countries and is nowadays part of a general newborn screening (5, 6). This method proved to be powerful to detect developmental dysplastic hips (DDH) at a very early age and is therefore associated with significantly reduced rates of severe dysplasia of adults in these populations. However, there is still reluctance regarding this method in various regions of the world. It is argued both, that the method shows high intra- and interobserver variabilities and that a general screening leads to an overtreatment (7–10). Although there are several studies rejecting the first argument, the second argument could not be verified by a Cochrane review, and both arguments are still common in oral debate (11–15).
Despite the fact that the Graf method is highly standardized, we considered the argument of inter-and intraobserver reliability respective inaccuracy of sonographic imaging according to the Graf criteria as reality-based experience from clinical work of practitioners and thus potentially hazardous for treatment decisions. It was hypothesized that reluctance to the Graf method correlates with inadequate sonographic figures in scientific literature.
Materials and methods
A systematic Pubmed search was performed using the Boolean Search String: “[(DDH) OR (Hip dysplasia)] AND (Graf)” resulting in a total of 418 studies found (December 2021). All studies were evaluated according to PRISMA criteria by title, abstract and by the original manuscript whether they were referring to the Graf method for diagnosis of DDH (Figure 1) (16). Inclusion criteria were complete manuscripts being accessible and presentation of exemplary figures of sonographic hip examinations. Studies were included independently of their language. Studies with figures referring explicitly to other techniques were excluded.
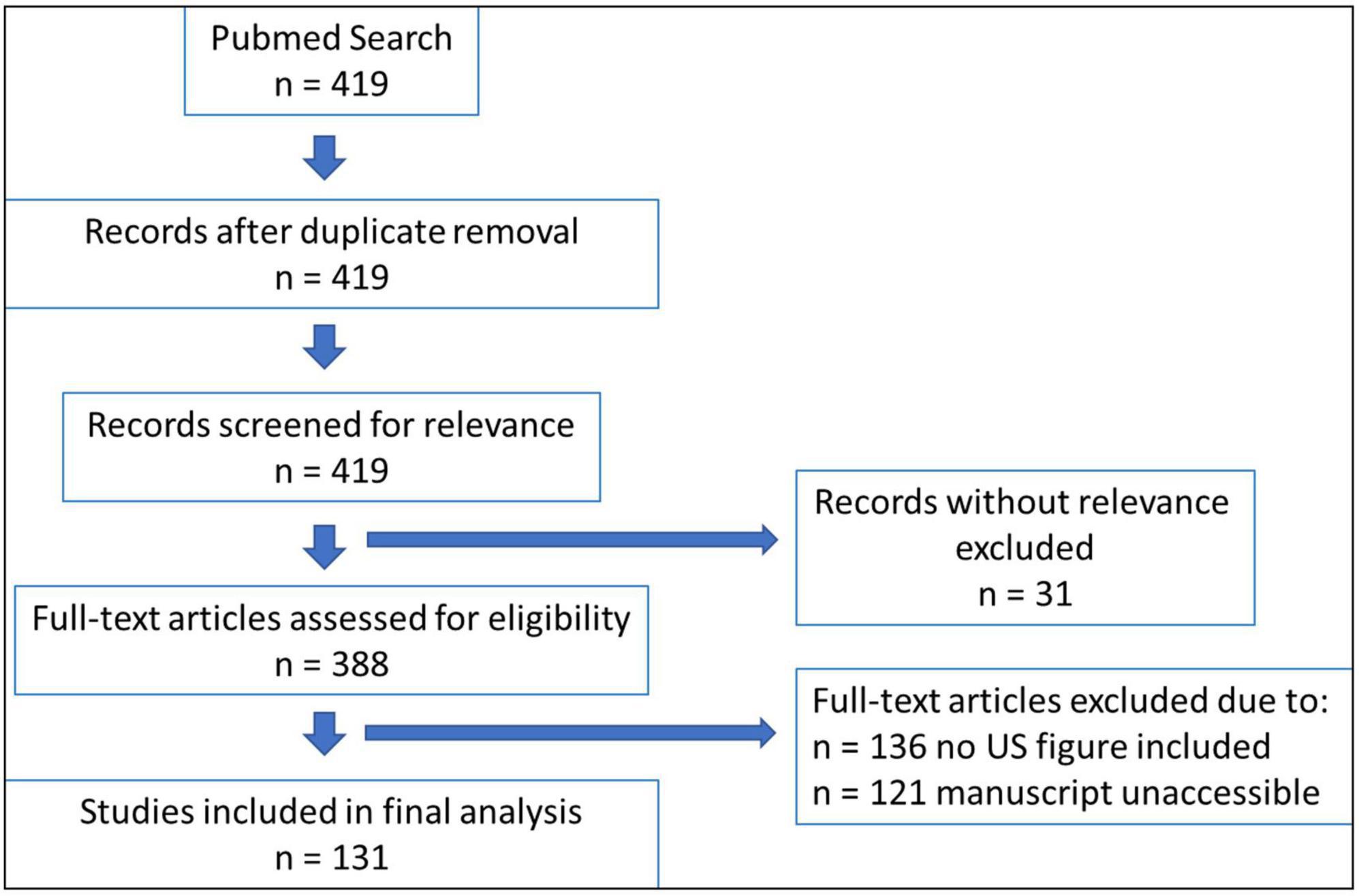
Figure 1. Study selection process according to the PRISMA scheme.
All studies were reviewed independently by two orthopedic residents. Both had participated at the official Graf instruction course and had major experiences in infantile DDH diagnosis using the Graf method. Data were extracted from each study using a standardized spreadsheet. Evaluation criteria were correct fulfillment of quality criteria according to the Graf quality assessment algorithm (A: anatomical identification: 1. Chondro-osseous border, 2. Femoral Head, 3. Synovial fold, 4. Joint Capsule, 5. Labrum, 6. Cartilage, 7. Bony roof, 8. Bony rim (turning point); B: usability check: 1. Lower limb of the Ilium, 2. Cross section through mid-portion of the bony roof, and 3. Acetabular Labrum; Figure 2). Detected errors were documented as well as a (in-)correct marking of the alpha and beta angle. Furthermore, metadata of each study such as year of publication, country of first author, age of children at primary sonographic hip examination (if applicable), treatment method (if applicable), treatment success rate (if applicable) and type of study (original vs. review) were collected.
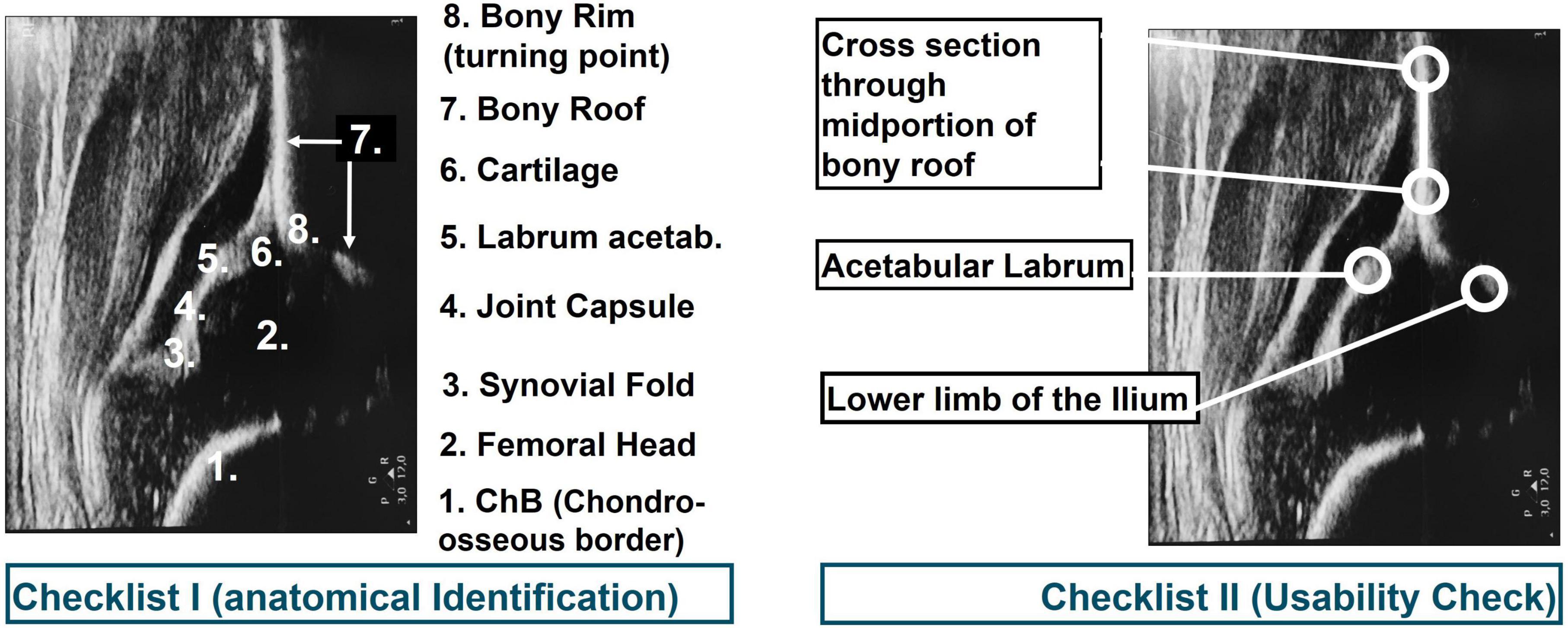
Figure 2. Checklist for correct (left) anatomical identification and (right) standard plane according to the Graf method.
For all studies, two reviewers independently extracted information; differences were resolved where necessary with the help of a third person specialized in children’s orthopedics.
Publications presenting figures of congenital hip dislocation were rated as correct as the standard plane according to Graf is not achievable in these cases. Systematic user error was assumed when illustrations in manuscripts were presented as correct according to the Graf method but did not meet the quality criteria according to the Graf method.
Statistical heterogeneity among studies was not examined due to above described figurative endpoints.
Results
The Pubmed Search resulted in 419 listed publications. Of these, 31 studies were excluded due to missing relevance. Another 135 studies did not contain a figure of a sonographic hip examination and for 121 studies the manuscript was not accessible online. 131 studies were included into final analysis for this review. Studies are listed by Pubmed-ID in Table 1. In 63 studies (48.1%) quality criteria according to Graf were not met. The majority of these studies insufficiently depicted anatomical landmarks. In 43 studies, pictures were presented without the possibility to identify all eight anatomical landmarks (e.g., images without a chondro-osseous border, cartilaginous roof not identified, joint capsule confused with intermuscular septum, etc.). 13 studies (9.9%) presented images that were not within the standard plane. A tilting error was detected in 7 studies (5.3%) only. The α-angle measurement was shown in 98 studies (74.8%), the β-angle was determined graphically in 86 studies (65.6%). We observed incorrectly plotted lines for the α-angle in 26 studies (19.8%). In most cases, the line through the os ilium was correct but the angulation line indicating the bony roof angle (α-angle) was plotted into the osseous parts of the acetabulum instead of running tangential beneath it.
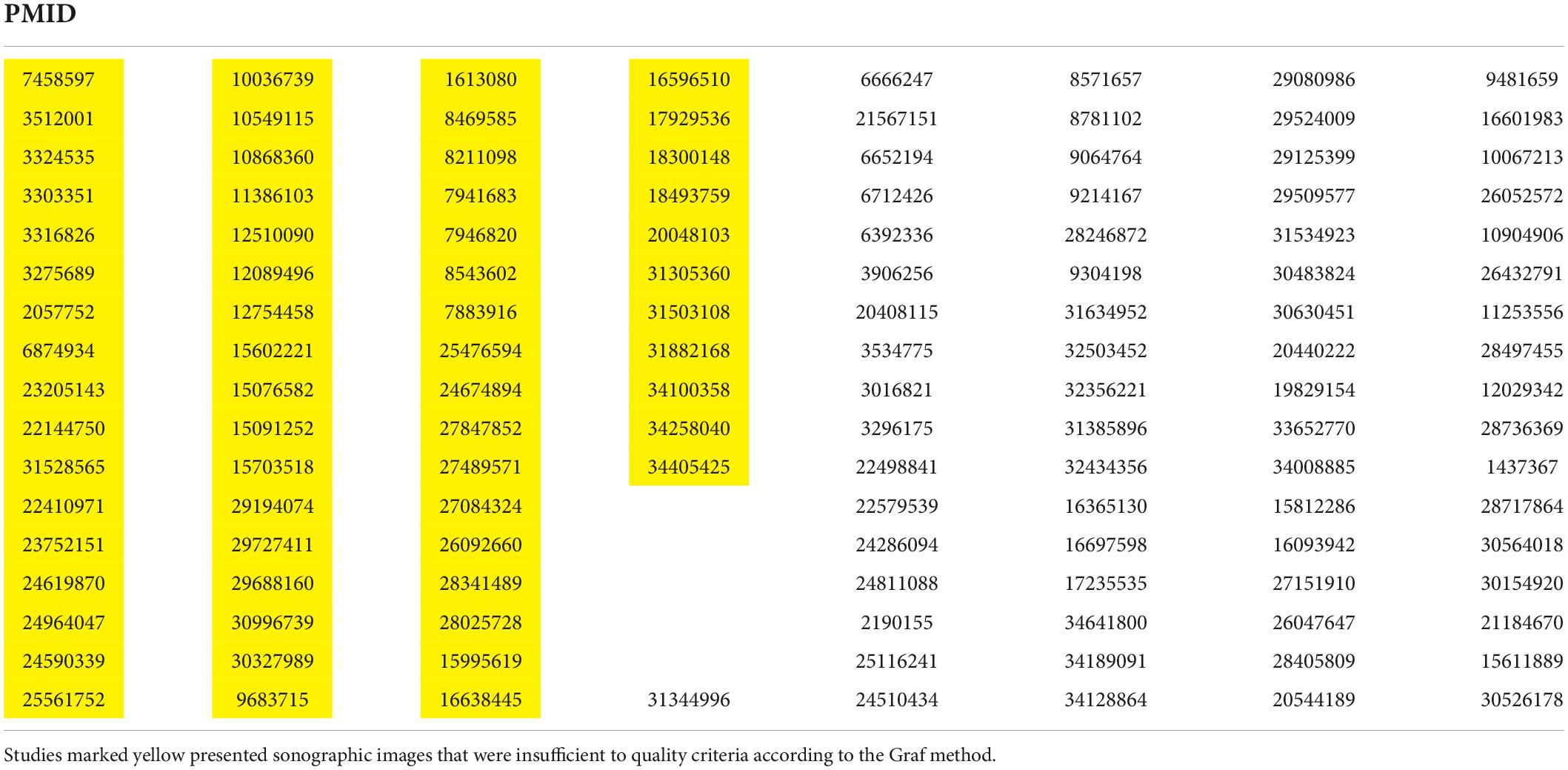
Table 1. Pubmed-IDs (PMID) of all 131 analyzed studies.
A large proportion of studies originated from Europe and German-speaking countries (Germany 29 studies; Austria 17 studies; Turkey 22 studies; Canada 8 studies; United States 7 studies; China 6 studies; United Kingdom and Brazil 5 studies each; Italy and Netherlands 4 studies each; Romania 3 studies; Croatia, France, Japan, Norway, Poland, Switzerland, Taiwan 2 studies each; Denmark, Egypt, Iran, Mongolia, Serbia, Singapore, Sweden 1 study each). German-speaking countries had a significantly higher rate (p = 0.02) of correct sonographic images than other countries (percentages of correct sonographic images: Germany: 62.1%, Austria: 70.6%, Turkey: 54.5%, United Kingdom: 40.0%, United States: 14.3%, Brazil: 20%, China: 66.7%, Netherlands: 50.0%, Italy: 50.0%, Canada: 0%).
There were 14 review articles (10.7%) and 117 original works (89.3%). 105 studies (80.1%) contributed data to the age of children at sonographic hip examination. In all but 10 studies the age was less than 3 months. Among the 10 studies reporting on children more than 6 months of age at sonographic hip examination, there were cases of initial failed therapy, delayed diagnosed included accounting for late (mostly secondary) examination. Maximum ages reported for sonographic hip examination were 83 weeks respective 5 years.
Discussion
Hip dysplasia represents a pre-arthritic deformity and it is estimated that 10–15% of patients requiring hip arthroplasty beneath the age of 50 do so because of dysplastic hips (17, 18). Without doubt the introduction of standardized hip sonography by Graf in the early 1980s has significantly contributed to fewer cases of severe hip dysplasia in adults requiring extensive surgery (5, 19).
Although universal infantile hip screening programs in German-speaking countries have shown to be very successful, there is still significant reluctance regarding this established method. Overtreatment in DDH therapy is suspected (20). Yet, it is essential to differentiate between different degrees of DDH. While IIa hips according to Graf may mature into type I hips without additional treatment, it is general consent that Graf type III and IV hips need to be treated to prevent severe dysplasia in adults and identification of these hips is based on clinical examination and sonographic imaging according to the Graf method. Nevertheless, there are authors claiming, that those hips will turn healthy after some months of follow-up, basing their conclusion on sparse data (21). Principally, dislocated or instable hips (Graf type III or IV) can be treated either by closed reduction or by Pavlik harness (22, 23). Closed reduction yields the advantage of immediate reposition control (24).
Although the Graf method is the most known and widespread technique for sonographic examination of pediatric hips, there is partial dissent on which classification or sonographic method is to be used for diagnosis of DDH. So far, no study demonstrated superiority regarding specifity and sensitivity of other sonographic examination protocols over the Graf method. In contrast, there is evidence indicating that criteria according to Graf (α-angle) are better reproducible than femoral head coverage as used in the Terjesen classification (3). Furthermore, a study by Roposch and colleagues described in an illustrative manner the controversies among orthopedic surgeons from different regions and countries (25).
This current review aims to identify reasons why the standardized method according to Graf is still matter of debate regarding reproducibility and practicability. Although authors within analyzed studies (Tab. 1) referred to the Graf method, a large percentage (48.1%) of these studies did not fulfill basic criteria for performing the Graf method. Therefore, it becomes evident that the term Graf is widely known but the underlying method is not applied correctly in the scientific and subsequently the clinician community that orientates on recent advances and publications in this field. Hence, this might explain why the Graf method remains subject to criticism regarding intra- and interrater variability.
A higher rate of correct images was found in publications originating from German-speaking countries, which might be explained by a higher density of trainings on this method and the integration of this method into an obligatory pediatric screening programs. Unfortunately, the rate of incorrect sonographic images in scientific publications per year did not decrease since the introduction of the Graf method.
It has to be admitted that this review evaluated only representative images in analyzed publications and may thus be subject to bias. However, authors are keen to select most representative and accurate images to demonstrate their measurement and method of data acquisition in order to support their findings and scientific theory. If those images are erroneous, it is justifiable to conclude that a majority of other measurements are incorrect as well. Yet, it is highly questionable if every incorrect image led to an incorrect treatment.
A large percentage of initially detected publications was not accessible online and thus excluded from final analysis. This may bias the results of this study. However, this problem of limited access to certain original manuscripts is a general problem for all researchers and clinicians researching on DDH. These online inaccessible manuscripts cannot portray correct or incorrect images to the community and therefore cannot not change the overall impression of inadequate application of the Graf method.
One study published by Graf himself in 1980 was included in this review for historical reasons, although the Graf method was finally introduced in 1983 (Figure 3). For reasons of publishing rights and collegiality no examples from analyzed publications were shown in this manuscript.
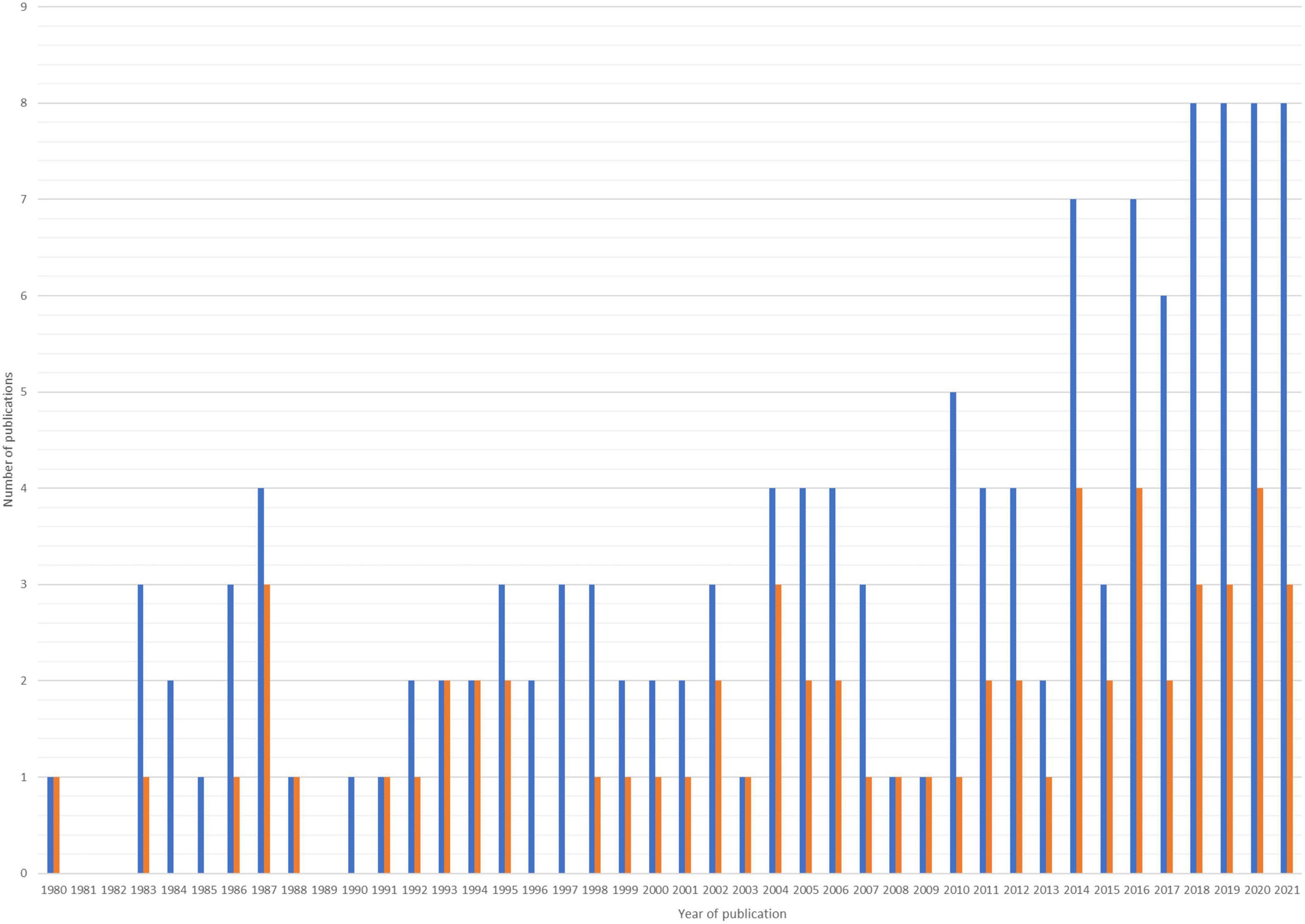
Figure 3. Publications by year. Blue are publications in a certain year and orange are publications with incorrect sonographic images according to the Graf method. Only publications that were analyzed in this review were included in this chart.
In conclusion, the Graf method is known for four decades but there are still major reservations and skepticism among clinicians and scientists around the globe regarding this method, which may be partly based on incorrect sonographic images in scientific publications. When performed correctly, however, the Graf method is of high diagnostic value.
Author contributions
SP and SW contributed to the study conception and design. SW wrote the first draft of the manuscript. All authors performed the material preparation, data collection and analysis, commented on previous versions of the manuscript, and read and approved the final manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Harcke HT, Grissom LE. Performing dynamic sonography of the infant hip. AJR Am J Roentgenol. (1990). 155:837–44.
2. Löer F, Casser HR, Straub A. Veränderte Indikationsstellung zur Röntgenuntersuchung der Säuglingshüfte nach Einführung der Sonographie. In: Frank W, Eyb R editors. Die Sonogr der Orthopädie. Vienna: Springer (1988). p. 167–71. doi: 10.1007/978-3-7091-3348-4_26
3. Peterlein CD, Schüttler KF, Lakemeier S, Timmesfeld N, Görg C, Fuchs-Winkelmann S, et al. Reproducibility of different screening classifications in ultrasonography of the newborn hip. BMC Pediatr. (2010) 10:98. doi: 10.1186/1471-2431-10-98
4. Falliner A, Schwinzer D, Hahne HJ, Hedderich J, Hassenpflug J. Comparing ultrasound measurements of neonatal hips using the methods of Graf and Terjesen. J Bone Joint Surg Br. (2006) 88:104–6. doi: 10.1302/0301-620X.88B1.16419
5. Thaler M, Biedermann R, Lair J, Krismer M, Landauer F. Cost-effectiveness of universal ultrasound screening compared with clinical examination alone in the diagnosis and treatment of neonatal hip dysplasia in Austria. J Bone Joint Surg Br. (2011) 93:1126–30. doi: 10.1302/0301-620X.93B8
6. Von Kries R, Ihme N, Oberle D, Lorani A, Stark R, Altenhofen L, et al. Effect of ultrasound screening on the rate of first operative procedures for developmental hip dysplasia in Germany. Lancet. (2003) 362:1883–7. doi: 10.1016/S0140-6736(03)14957-4
7. Dias JJ, Thomas IH, Lamont AC, Mody BS, Thompson JR. The reliability of ultrasonographic assessment of neonatal hips. J Bone Joint Surg Br. (1993) 75:479–82. doi: 10.1302/0301-620X.75B3.8496227
8. Paton RW. Screening in developmental dysplasia of the hip (DDH). Surgeon. (2017) 15:290–6. doi: 10.1016/J.SURGE.2017.05.002
9. Hareendranathan AR, Mabee M, Punithakumar K, Noga M, Jaremko JL. A technique for semiautomatic segmentation of echogenic structures in 3D ultrasound, applied to infant hip dysplasia. Int J Comput Assist Radiol Surg. (2016) 11:31–42. doi: 10.1007/S11548-015-1239-5
10. Jaremko JL, Mabee M, Swami VG, Jamieson L, Chow K, Thompson RB. Potential for change in US diagnosis of hip dysplasia solely caused by changes in probe orientation: patterns of alpha-angle variation revealed by using three-dimensional US. Radiology. (2014) 273:870–8. doi: 10.1148/RADIOL.14140451
11. Shorter D, Hong T, Osborn DA. Cochrane Review: screening programmes for developmental dysplasia of the hip in newborn infants. Evid Based Child Health. (2013) 8:11–54. doi: 10.1002/EBCH.1891
12. Jejurikar N, Moscona-Mishy L, Rubio M, Cavallaro R, Castañeda P. What is the interobserver reliability of an ultrasound-enhanced physical examination of the hip in infants? A prospective study on the ease of acquiring skills to diagnose hip dysplasia. Clin Orthop Relat Res. (2021) 479:1889–96. doi: 10.1097/CORR.0000000000001863
13. Simon EA, Saur F, Buerge M, Glaab R, Roos M, Kohler G. Inter-observer agreement of ultrasonographic measurement of alpha and beta angles and the final type classification based on the Graf method. Swiss Med Wkly. (2004) 134:671–7. doi: 10.5167/UZH-19372
14. Rosendahl K, Aslaksen A, Lie RT, Markestad T. Reliability of ultrasound in the early diagnosis of developmental dysplasia of the hip. Pediatr Radiol. (1995) 25:219–24. doi: 10.1007/BF02021541
15. Ulziibat M, Munkhuu B, Schmid R, Baumann T, Essig S. Implementation of a nationwide universal ultrasound screening programme for developmental dysplasia of the neonatal hip in Mongolia. J Child Orthop. (2020) 14:273. doi: 10.1302/1863-2548.14.200029
16. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Rev Esp Nutr Humana y Diet. (2016) 20:148–60. doi: 10.1186/2046-4053-4-1/TABLES/4
17. Jacobsen S, Sonne-Holm S. Hip dysplasia: a significant risk factor for the development of hip osteoarthritis. A cross-sectional survey. Rheumatology. (2005) 44:211–8. doi: 10.1093/rheumtology/keh436
18. Graf R. Hip sonography: background; technique and common mistakes; results; debate and politics; challenges. HIP Int. (2017) 27:215–9. doi: 10.5301/hipint.5000514
19. Gray A, Elbourne D, Dezateux C, King A, Quinn A, Gardner F. Economic evaluation of ultrasonography in the diagnosis and management of developmental hip dysplasia in the United Kingdom and Ireland. J Bone Joint Surg Am. (2005) 87:2472–9. doi: 10.2106/JBJS.D.01997
20. Bialik V, Bialik GM, Wiener F. Prevention of overtreatment of neonatal hip dysplasia by the use of ultrasonography. J Pediatr Orthop B. (1998) 7:39–42. doi: 10.1097/01202412-199801000-00007
21. Sakkers R, Pollet V. The natural history of abnormal ultrasound findings in hips of infants under six months of age. J Child Orthop. (2018) 12:302–7. doi: 10.1302/1863-2548.12.180056
22. Walter SG, Bornemann R, Koob S, Ossendorff R, Placzek R. Closed reduction as therapeutic gold standard for treatment of congenital hip dislocation. Z Orthop Unfall. (2020) 158:475–80. doi: 10.1055/a-0979-2346
23. Cashman JP, Round J, Taylor G, Clarke NMP. The natural history of developmental dysplasia of the hip after early supervised treatment in the Pavlik harness. A prospective, longitudinal follow-up. J Bone Joint Surg Br. (2002) 84:418–25. doi: 10.1302/0301-620X.84B3.12230
24. Walter SG, Endler CHJ, Remig AC, Luetkens JA, Bornemann R, Placzek R. Risk factors for failed closed reduction in dislocated developmental dysplastic hips. Int Orthop. (2020) 44:2343–8. doi: 10.1007/s00264-020-04655-1
Keywords: Graf, DDH, hip, ultrasound, dysplasia
Citation: Walter SG, Ossendorff R, Yagdiran A, Hockmann J, Bornemann R and Placzek S (2022) Four decades of developmental dysplastic hip screening according to Graf: What have we learned? Front. Pediatr. 10:990806. doi: 10.3389/fped.2022.990806
Received: 10 July 2022; Accepted: 19 August 2022;
Published: 15 September 2022.
Edited by:
Thomas Baumann, Other, Solothurn, SwitzerlandReviewed by:
Katharina Gather, Universitätsklinikum Heidelberg, GermanyVito Pavone, University of Catania, Italy
Copyright © 2022 Walter, Ossendorff, Yagdiran, Hockmann, Bornemann and Placzek. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sebastian G. Walter, sebastianwalter01@gmail.com; orcid.org/0000-0002-6203-8616
†These authors have contributed equally to this work