
Abstract
This quasi-experimental study examined the effects of Cognitive Behavioral Group Therapy (CBGT) in alleviating anxiety and enhancing emotion regulation in community-sample Thai middle school students. Forty-seven community-sample students in Grades 7–9 with elevated SCARED scores participated in this pre-post treatment–control study. Twenty-three in the treatment group attended the eight-session 2-hour semi-weekly CBGT. The remaining were the control group. Before and after the intervention, the participants completed the measures of anxiety and emotion regulation. Data obtained were subsequently analyzed using repeated-measures and between-groups MANOVAs. At post-intervention, the treatment group reported a significant decrease in anxiety but a significant increase in emotion regulation. Furthermore, when compared with the control group, their anxiety score was significantly lower but their emotion regulation score was significantly higher, respectively. Findings supported the benefits of CBGT in reducing anxiety in Thai middle school students and in enhancing their emotion regulation skills. Therapeutic implications for anxiety reduction were discussed.
Similar content being viewed by others


Introduction
Anxiety disorders have been recognized as one of the most prevalent psychological disorders around the world (Kessler et al., 2009). Up to 20% of those inflicted by the disorders are children and adolescents (Barrett et al., 1996). The National Comorbidity Survey (i.e., Merikangas et al., 2010) reported that up to 17.8% of American adolescents sought treatment for the disorders; and 29.1% of them experienced severe anxiety to the point that their daily functions became impaired. In Thailand, adolescent anxiety has been recognized for its clinical implications. Based on the Survey on Mental Health and Migration 2011, anxiety disorders were estimated to affect approximately 15% of Thai adolescents (National Statistical Office Thailand, 2021). The effect could be beyond this estimation, given the relatively limited access to mental health services within Thailand and increased reports of adolescent anxiety during COVID-19 (e.g., Racine et al., 2020).
Without proper management, adolescent anxiety could bring about a host of debilitating psycho-social outcomes. These included substance abuse, hospitalization, and suicide (Kendall et al., 2010); adjustment difficulties, chronic stress, and low life satisfaction subsequent to anxiety during adolescence (Essau et al., 2014). Similarly, Woodward and Fergusson (2001) reported adolescents diagnosed with anxiety disorders to experience higher risks of the disorders two decades afterward. Altogether, these suggest the necessity to prevent and alleviate adolescent anxiety, either in the subclinical or clinical levels, due to their long-term negative impacts. (Rockhill et al., 2010).
Despite the aforementioned necessity, a number of adolescents afflicted with anxiety disorders were yet to obtain proper psychological support (Essau, 2005). At times, anxiety symptoms might not be readily detected but were mistaken as age-related developmental issues, resulting in erroneous diagnoses (Albano et al., 2003). Aside from these limitations, in Thailand, an access into proper assessments and psychological supports for adolescent anxiety remained limited. Additionally, misconceptions and stigmatization existed in mental health service usage (Poonyakanok & Tuicomepee, 2011). Altogether, these prevented proper psychological support for Thai adolescents experiencing anxiety.
The current study, therefore, was aimed to propose a therapeutic intervention to address anxiety in Thai middle school students. This group of adolescents underwent a transitional period between elementary and high schools. Various adjustments were required. Not only did they have to adapt to the new learning formats and increasing academic demands (Juvonen et al., 2004) but these adolescents also had to adjust to puberty and engage in identity explorations (Shaffer, 2005). Anxiety was not unanticipated (Moran, 2016). Providing a preventative measure to reduce anxiety for middle school students, who experienced escalated but sub-clinical anxiety, would be highly beneficial.
Past literature identified Cognitive Behavior Therapy (CBT; Beck, 2011) as a key intervention appropriate for this purpose (Spence et al., 2001). Empirically based and widely regarded as the gold standard treatment for anxiety (David et al., 2018), Beck (2011) conceptualized emotional experience as resulting from the root cause of cognitive processes and underlying evaluative beliefs that led to inaccurate information processing and unhelpful cognitive errors. Adolescent anxiety was shown to be instigated and perpetuated by these processes and beliefs (Cummings & Fristad, 2012).
CBT-based therapeutic intervention entailed modification of information processing and relevant cognitive errors through the engagements of therapeutic components and techniques in cognitive and behavioral domains (Bennett-Levy et al., 2004). The intervention was time-limited, structured, and problem-focused (Hollon & Beck, 1994). Therapeutic outcomes were transferable for outside-session post-intervention usages; and treatment maintenance was promising. For adolescent anxiety, up to six-year maintenance has been reported (Barrett et al., 2001).
Inherent in CBT was the cultivation of a key skill essential for emotion management, or emotion regulation skills. Compromised skills in this domain were recognized as precipitating and perpetuating anxiety (Aldao et al., 2010). With this recognition, various methods of emotion regulation have been proposed. Widely approved was cognitive reappraisal, which involved the engagement of cognitive changes to construe a potentially emotion-eliciting situation in ways that affected its emotional impact (Gross & John, 2003). In anxiety management, this entailed the reevaluation of the overestimation of the likelihood of the feared incidents and the perception of compromised control over their outcomes. Cognitive reappraisal was shown to be associated with young individuals’ anxiety. Those with high anxiety were reportedly lower in this emotional regulation skill (Suveg & Zeman, 2004). Hence, the skill was generally cultivated in CBT for adolescent anxiety.
Empirical support for its effectiveness, the employment of CBT is emerging in Thailand. Despite initial studies (e.g., Bryant et al., 2011) and attempts to apply CBT to diverse populations (Petersen et al., 2016), empirical studies of CBT for adolescent anxiety remains lacking (Phokhasawadi et al., 2014). Questions have been raised as well in its cross-cultural applications (Williams et al., 2006). An investigation of CBT for adolescent anxiety in Thailand, therefore, would be highly beneficial in responding to these questions and paving the ways for subsequent relevant studies.
The delivery of CBT in the current study would be conducted in a group format (i.e., Cognitive Behavioral Group Therapy: CBGT). This well-recognized format (Corey, 2011) was selected for various reasons. To begin with, accommodating 6–8 participants (Corey, 2011), the group promised a greater number of service recipients at one time and was promising within the context in which psychological support remained limited like Thailand. The format, additionally, helped reduce stigmatization, a key barrier to the service access in the country (Poonyakanok & Tuicomepee, 2011) and also allowed exchanges and support among group participants during the relatively abstract cognitive modification. Group members could assist one another in this process through scaffolding (McLeod, 2012). With these benefits, the group format was adopted by various CBT-based anxiety intervention programs for adolescents (e.g., Lau et al., 2010; Scaini et al., 2022) and well supported by empirical evidence (Ginsburg & Drake, 2002; Herzig-Anderson et al., 2012).
The Current Study
The present quasi-experimental research study, therefore, would be conducted to examine the efficacy of CBGT in community-based middle school students with elevated anxiety. Foci would be on two key outcomes of: 1) emotion regulation and 2) anxiety. Whether the CBGT would bring about changes in participants’ capacities in emotion regulation, as captured by Gullone and Taffe’s Emotion Regulation Questionnaire for Children and Adolescents (2012), would be firstly examined. It was hypothesized that, at post intervention, emotion regulation capacities of those attending the CBGT (i.e., the treatment group) would be higher than at pre-intervention and also higher than those of the no-treatment control group.
Secondly, similar hypotheses would be tested for the participants’ anxiety, despite being in an opposite direction. At post intervention, the treatment groups’ anxiety would be lower than at pre-intervention and lower than the control group. As would be presented in the Method Section, anxiety here would be measured by the Screen for Child Anxiety Related Disorders- Child Version (SCARED-Child Version; Birmaher et al., 1997). An overall SCARED score would be used. Despite its high recognition (e.g., Crocetti et al., 2009), the usage of the SCARED five subscales remained debatable within in culturally diverse samples (Runyon et al., 2018). Therefore, an overall score, which was well-supported across cultures (e.g., Isolan et al., 2011), would be employed. The employment resonated past examinations of CBT therapeutic changes in adolescent anxiety (e.g., Scaini et al., 2022).
If the efficacy of CBGT was supported here, counsellors who provided psychological support to middle school students both within and outside school settings could employ CBGT and/or its therapeutic components as a preventative measure in assisting the students to better manage their anxiety.
Method
Participants and Procedure
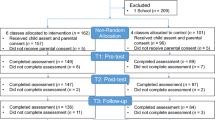
Participants were recruited only after an approval had been obtained from the institutional Ethics Review Committee for Research Involving Human Research Participants (i.e., Clearance No 259/2018). The community-based participants came from a large province in Thailand and were recruited from two public schools in its capital. These schools were selected due to their substantial sizes, co-education practices, and comparability. To prevent data contamination (Robinson et al., 2020) and to enhance practicality, students from the first school were assigned into the treatment group and those from the second school became the no-treatment control one. The two schools were contacted by the first author, who obtained their permissions for research promotions around the same period, at the beginning weeks of the same semester and academic year.
With the school permission, the researchers introduced the research study in class. An emphasis was made on the voluntary nature of its participation. Those interested were provided with a written information sheet outlining details about the study including its two participation conditions (i.e., that the students would be assigned into the treatment or control condition based on their schools and that, upon the study completion, the control group would receive a CBT-based self-help guideline for anxiety management but no therapeutic intervention due to the semester conclusion). Upon their consents, interested students also filled out a set of paper-and-pencil based screening questionnaires (i.e., SCARED and questions regarding mental health diagnoses and treatments) after class to determine their eligibility for study participation.
Those fulfilling the selection criteria (i.e., with the SCARED score within 1 SD above the local mean of 27 points or obtaining the SCARED scores of 28–39) and not receiving any mental health diagnoses nor treatments) were subsequently contacted for their parental permissions for study participation. Of 486 students responded to the screening questionnaires, 64 fitted with the inclusion criteria. Forty-seven of them (i.e., 73.23%) obtained parental permissions and participated in the study. Those ineligible or without such permissions were provided with a CBT-based self-help guideline for anxiety management.
For the 47 participants, all were in middle schools, Grades 7–9. Their mean age was 13.98 years (SD = 0.57 years) and the majority (i.e., 34 or 72.3%) were female. As previously mentioned, for data contamination prevention and practicality, students from one school were assigned into the treatment group (n = 23) and the other the control one (n = 24). Pre-participation preliminary analyses indicated no significant differences between the two groups in age (t(45) = -0.77, p = 0.44), gender (χ2(1,46) = 1.14,, p = 0.34), grade levels (χ2(2,47) = 2.90, p = 0.23), Grade Point Average (t(45) = 1.35,, p = 0.18), or the anxiety scores (t(36.76) = 1.18,, p = 0.24).
Method
Prior to the intervention, both treatment and control groups completed a paper-and-pencil based demographical sheet (i.e., age, gender, current grade, and Grade Point Average (GPA) and the measures of anxiety and emotion regulation. Then, the twenty-three participants in the treatment condition were divided, based on their scheduling, into three groups (i.e., two groups of eight participants and one group of seven participants) and attended an eight-session two-hour Cognitive Behavioral Group Therapy (CBGT). The group sessions were organized semi-weekly so they would be completed prior to the participants’ final examinations. Then, after the four-week intervention, the treatment groups again completed the two measures. The twenty-four participants in the control group followed a similar procedure and timeframe. An only exception was that, as previously agreed, they did not receive CBGT but were provided with a CBT-based self-help guideline for anxiety management upon the study conclusion.
Measures
In addition to demographical information, participants responded to the measures of anxiety and emotion regulation. These measures were translated into Thai and adapted to be culturally- and age-appropriate to the participants. They were reviewed by a panel of three doctoral-level Thai psychologists, who not only examined the appropriateness of the translations and adaptations but also evaluated their Item-Objective Congruence (IOC; Gregory, 2015) for their content validity. Both measures yielded satisfactory IOCs. Details about each were as follows:
Anxiety
The Screen for Child Anxiety Related Disorders- Child Version (SCARED-Child Version; Birmaher et al., 1997) was used to measure the degree to which participants experienced anxiety. This 41-item self-report measure captured five subdomains of anxiety: 1) panic, 2) generalized anxiety, 3) separation anxiety, 4) social phobia, and 5) school avoidance. The participants responded to items in the measure on a 3-point Likert scale (i.e., 0 = “Not true or hardly ever true” to 2 = “Very true or often true”). As previously mentioned, in this study, the SCARED total score was used for questions remained regarding the usage of the five subdomain scores in culturally diverse samples (Runyon et al., 2018). The total score was calculated by summing across all of the items, which were positively worded. A higher score indicated a higher level of anxiety experienced.
In this study, a confirmation factor analysis (CFA) confirmed the hypothesized single-component model of the translated SCARED, χ2 = 956.35, df = 721, p < 0.05; CFI = 0.952; TLI = 0.946; and RMSEA = 0.027 [90% CI: 0.02, 0.03]. Additionally, the translated measure exhibited high reliability as shown in the Cronbach’s alpha estimate of 0.92) [95% CI: 0.91, 0.93].
Emotion Regulation
The Cognitive Reappraisal Subscale of the Emotion Regulation Questionnaire for Children and Adolescents (Gullone & Taffe, 2012) was used to measure the degree to which participants engaged in cognitive strategies to construe potentially emotion-eliciting situations in ways that changed their emotional impacts. The participants responded to the 6-item subscale on a 5-point Likert scale (i.e., 1 = “Strongly disagree” to 5 “Strongly agree”). The total score was calculated by summing across all of the items, which were positively worded. A higher score indicated a higher engagement of cognitive strategies for emotion regulation. In this study, a CFA confirmed the hypothesized single-component model of the translated Cognitive Reappraisal Subscale, χ2 = 5.86, df = 5, p = 0.321; CFI = 0.986; TLI = 0.959; and RMSEA = 0.057 [90% CL: 0.00, 0.21]. Additionally, the translated subscale exhibited satisfactory reliability as shown in the Cronbach’s alpha estimate of 0.70 [95% CI: 0.55, 0.80].
Therapeutic Intervention
Referring to the empirically based CBGT programs and relevant techniques (e.g., Albano & Kendall, 2002; Kendall & Suveg, 2006), the current CBGT was devised by the researchers to reduce anxiety and increase emotion regulation skills in ways that were culturally and age appropriate to Thai middle school students. The CBGT plan was reviewed by two expert CBT psychologists and piloted in two groups of participants whose characteristics were akin to study participants. Feedback from these sources were used to improve the program.
The CBGT consisted of eight two-hour sessions and ran twice a week for four weeks, amounting to a total of sixteen hours. It was applied to 23 treatment participants, who were divided into three groups based on their scheduling (i.e., one group of seven participants and two groups of eights participants). The CBGT was conducted by the first author who received a CBGT training and practicum and implemented the intervention based on the aforementioned pre-piloted tailor-made research-based program. A protocol check was engaged and confirmed during a weekly supervision from a CBGT expert to ascertain that the intervention was provided as planned.
An overview of the CBGT employed here was provided in Table 1. Overall, the program was divided into three phases. The first phase (Sessions 1–3) involved cultivating therapeutic alliance and orienting group members toward CBGT. Additionally, psychoeducation about anxiety was provided. Participants were equipped with initial information about anxiety, its relevant components and impacts, the perpetuating role of behavioral avoidance, and behavioral skills (i.e., relaxation strategies) that helped reduce the avoidance. In the second phase (Sessions 4–6), cognitive strategies for anxiety reduction were introduced. The last phase (Sessions 7–8) focused on skill consolidation. Then, the participants integrated the cognitive and behavioral skills introduced to better manage potential anxiety-provoking situations in preparation for relapse prevention. Throughout these phases, self-monitoring and homework were assigned to assist the participants to generalize the skills and knowledge obtained. Problem-solving was also engaged to enhance therapeutic gains.
Data Analysis
Data analyses were conducted using repeated-measures and between-groups multivariate analyses of variance (MANOVAs), with time and group as independent variables. Dependent variables were emotion regulation and anxiety. Preliminary analyses for MANOVAs assumptions (e.g., homogeneity of covariance matrices (i.e., Box’s M = 11.45, p = 0.41), absences of multivariate outliers and multicollinearity (i.e., the association of the two dependent variables were 0.39, p < 0.01)) (Hair et al., 2010) were confirmed. Therefore, repeated-measures and between-groups MANOVAs were conducted.
Results
An overall outcome of the repeated-measures and between-groups MANOVAs were shown in Table 2. There, group and time had significant main effects, with a relatively large effect size (Cohen, 1992), Wilk’s Lamda F(2, 44) = 21.71, p < 0.001, η2 = 0.50. Outcomes of further analyses indicated significant interaction effects on both anxiety, F(1, 45) = 18.94, p < 0.001, η2 = 0.30 (See Table 3) and emotion regulation, F(1, 45) = 22.76, p = 0.001, η2 = 0.34 (see Figs. 1 and 2).

The interaction effect on anxiety

The interaction effect on emotion regulation
Given the significant interaction effects, Scheffe post-hoc analyses were performed. As there were multiple comparisons, the critical value was adjusted to 0.025 to minimize Type I error (Mayers, 2013). Time-wise, when compared to pre-intervention, the CBGT (i.e., treatment) group reported significant decreases in anxiety, t(22) = -5.67, p < 0.025, g = 1.49, 95% [CI:0.85,2.14] but a significant increase in emotion regulation, t(22) = 5.74, p < 0.025, g = 1.12, 95% [CI:0.50,1.74] at post-intervention. No significant changes in these variables across the two points in time in the non-CBGT (i.e., control) group. Additionally, between-group comparisons suggested that, when compared with the non-CBGT, the CBGT group reported significantly lower anxiety, t(45) = -3.80, p < 0.025, d = 1.11, 95% CI [0.49, 1.72] but higher emotion regulation, t(45) = 2.72, p < 0.025, d = 0.79, 95% CI [0.20, 1.39] at post-treatment (Table 4).
Discussion
The present study examined the effectiveness of CBGT in Thai community-based middle school students who experienced elevated anxiety. Results indicated that the intervention was effective in reducing their anxiety and increasing their emotion regulation skills beneficial for anxiety management. Specifically, lower anxiety but higher emotion regulation was reported at post-intervention for the treatment group, who also scored then lower in anxiety but higher in emotion regulation than the control group.
The current findings were consistent with CBT assumptions that cognitive modification, with support from behavioral techniques, could enhance emotion regulation skills and alleviate anxiety (Beck, 2011). These findings were also consistent with Western empirical evidence of CBT effectiveness in these two domains (Aldao et al., 2010; Suveg et al., 2006, 2009; Trosper et al., 2009) and provided support to CBT cultural transferability. Next, relevant CBT components contributed to therapeutic gains here would be outlined to clarify the gains and to enhance the transferability.
CBGT Key Components
With CBT key emphasis on cognitive modification, CBGT cognitive component played an essential role in the therapeutic gains demonstrated here. Of particular importance were psychoeducation and cognitive restructuring. For the former, with relatively limited mental health service access, enhancing participants’ accurate understanding of anxiety through psychoeducation was particularly important. Participants were assisted to recognize the nature and contributing factors of anxiety. Such recognition was beneficial in normalizing the emotional experience and its symptoms as well as in reducing relevant threats and stigmatization (Alvarez et al., 2018).
Psychoeducation was conducted to enhance the participants’ acceptance of their anxiety and to reduce potential guilts and shames from its stigmatization. Additionally, with an understanding of relevant factors contributing to anxiety, the participants were likely to became more accurate in their therapeutic goal setting. Rather than aiming to totally eradicating anxiety, the participants were assisted recognized its potential benefits (e.g., the emotional response could be informative) and to set up an appropriate goal for its management. Likewise, psychoeducation about anxiety symptoms and their roles in anxiety maintenance (e.g., behavioral avoidance) was anticipated to contribute to the participants’ increased awareness and monitoring of these symptoms (Whitfield, 2010). Psychoeducation also provided rationales for subsequent treatment components (e.g., gradual exposure).
A key aspect of the cognitive intervention and the current study was emotion regulation skill training. After the participants obtained an understanding of the cognitive and emotional components of anxiety, they were assisted to engage in cognitive restructuring. Attempts were made to illustrate to them the key thesis of CBT, the impact of cognitions on emotional and behavioral outcomes. The illustration was conducted quite concretely (e.g., through a series of movie narrations), taking into considerations the participants’ emerging formal operation (e.g., Piaget, 1970), in preparation for cognitive restructuring. There, a game “Thought Pattern Monster Hunter” was introduced so that group members could practice detecting thought patterns that perpetuated or aggravated their anxiety. The members came up with the terms of the group consensus in identifying the thought patterns to make them concrete and meaningful. For example, one group agreed to label a repetitive catastrophic thinking as “Mr. Wheel” and an all-or-nothing thinking as “the Black-and-White Thinking Monster”. The group leader monitored to ascertain that group members well understood these personifications and relevant strategies for their managements.
Behavioral interventions helped reinforce the cognitive interventions and emotion regulation strategies introduced. Relaxation strategies, for example, were introduced to assist group members to manage their somatic responses to anxiety (Beidas et al., 2010) and to prevent an escalation of anxiety due to these responses (Huberty, 2012a, b). To assist the participants in identifying these somatic responses, the participants colored in a drawing of a human body to identify the areas in which they were impacted by these responses prior to engaging in relevant management strategies. Lastly, the participants were gradually assisted to face, rather than avoid, their fears in order to reduce the perpetuating impact of behavior avoidance (Cummings & Fristad, 2012).
Group Activities and Therapeutic Processes
Age-appropriate hand-on activities that promised to capture the participants’ interests (e.g., games and videoclips) were used in supporting the processes outlined above, particularly psychoeducation. Videoclips portraying relatable characters with experiences of anxiety were presented and to instigate the group exchanges. Examples included an animal character that used to choke on water so severely that it became fearful and avoid the water. Highlighted then was the group consensus that the avoidance prevented the character from learning that the choking might not necessarily reoccur. The story was revisited subsequently during the cognitive restructuring to reduce an overestimation of the feared incident and during the introduction of gradual exposure.
A hand-on activity was also used to consolidate the group members’ learning about the four interrelated components of anxiety (i.e., cognitions, emotions, behaviors, and physiological responses). After discussing these components, a flash card with a descriptor of each component would be presented to the entire group, who would assist each other to identify which component the descriptor belonged (e.g., “hand trembling” fell under physiological responses). Then, to facilitate the exchanges and practices, the members were divided into smaller groups of 2–3 members and practiced identifying the descriptors together. The activity assisted the group members to better distinguish anxiety responses. Of key importance was the distinction between cognitions and emotions, which was a foundation for cognitive restructuring and emotion regulation skill enhancement.
After each of the activities, a summary was made to emphasize key messages to ascertain learning consolidation. Information transmission was gradual with constant monitoring and checking for group members’ comprehension. Attempts were made to minimize usage of technical terms; and, as previously outlined, participants were encouraged to come up with group-consensus terms that helped capture the key concepts introduced. These, together with substantial time allocated for each activity, assisted in participants’ consolidation of the information conveyed in the group.
Throughout CBGT, homework was assigned so that group members could practice in- session lessons and to generalize therapuetic gains to their daily environments (Beidas et al., 2010). Support was also provided to facilitate homework engagement. For example, an eye-cating ruler-like measure labelled “Mood Meter Ruler,” was given to each member so that they could refer to a scale of 0 to 10 in evaluating their moods during their homework engagements. This ruler-like measure helped provide group members, whose formal operation (Piaget, 1970) was emerging, with a visual reference when discussing moods and emotional experiences, which were relatively abstract.
Additionally, although overall the participants well adhered to the assignments, occasions of non-compliances occurred. The group leader would explore reasons for the non-compliances. After the exploration, she would invite group members to brainstorm on possible solutions. All possibilities would be listed and evaluated before the non-compliant members would select the solutions of their preferences. Concurrently, the benefits of homework assignments were clarified and verbal reinforcement was given to enhance the adherences. The entire process was conducted in a non-judgmental stance and with a respect for the group members’ unique personal circumstances.
Lastly, the group format of the current CBGT intervention appeared to assist in therapeutic changes in various ways. To begin with, through members’ interactions, the group helped normalize the participants’ experiences of anxiety and potential senses of alienation (Herzig-Anderson et al., 2012). Additionally, based on their interactions and group activities, participants helped one another expand their worldviews, contributed to one another’s coping resources, and reduced overall threat perception of anxiety-provoking situations. The group leader attempted to enhance this by providing a safe environment where participants could openly discuss their experiences. This was due to the recognition and respect of the members’ needs for emerging identity and autonomy (Shaffer, 2005).
Limitations and Recommendations for Future Research and Applications.
Although current findings brought about promises in cross-cultural CBGT applications, findings from this initial study should be viewed with various considerations. First, a quasi-experimental design was used for practicality and to prevent data contamination. Random assignment was not employed; and characteristics of each participant group could confound the findings. This, together with a lack of an active-control group and follow-up assessments, rendered the scope of the finding outcomes. Lastly, that an overall SCARED score was employed here instead of its five subdomain scores (i.e., due to their potential cross-cultural limitations (Runyon et al., 2018)) prevented the examinations of changes in each subdomain of anxiety brought about by CBGT.
Future research may improve upon the present study by addressing these limitations. First, it may employ a randomized control trial design with an active treatment group. Then, the confounding effects of participants’ characteristics could be minimized and the effectiveness of the CBGT could be compared with other therapeutic interventions. Seconding, follow-up assessments would clarify whether the effects of the intervention persist after its conclusion. Lastly, further investigations on changes in the five subdomains of anxiety as introduced by CBGT would further clarify its efficacy in detail.
Despite areas for additional investigations, implications could be drawn from this initial study. Practitioners could apply CBGT proposed here for preventive and therapeutic measures of adolescent anxiety. The benefits of the group format employed (Mifsud & Rapee, 2005) appeared generalizable. Subsequent studies could consider the format as well as group activities and processes outlined here in enhancing therapeutic intervention. Mental health practitioners (e.g., counselors and psychologists) could apply CBGT in their services to middle school students encountering anxiety. Similarly, school personnel aiming at providing a school-based intervention (Mychailyszyn et al., 2011) to these students as a preventative measure could apply the CBGT key therapeutic components (e.g., psychoeducation, cognitive restructuring, relaxation training) and refer to its group dynamics as well as the accepting and respectful stances in supporting these students in their anxiety management.
References
Albano, A. M., Chorpita, B. F., & Barlow, D. H. (2003). Childhood anxiety disorders. In E. J. Mash & R. A. Barkley (Eds.), Child psychopathology (pp. 279–329). Guilford Press.
Albano, A. M., & Kendall, P. C. (2002). Cognitive behavioural therapy for children and adolescents with anxiety disorders: Clinical research advances. International Review of Psychiatry, 14(2), 129–134. https://doi.org/10.1080/09540260220132644
Aldao, A., Nolen-Hoeksema, S., & Schweizer, S. (2010). Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review, 30(2), 217–237. https://doi.org/10.1016/j.cpr.2009.11.004
Alvarez, E., Puliafico, A., Leonte, K. G., & Albano, A. M. (2018). Psychotherapy for anxiety disorders in children and adolescents.
Barrett, P. M., Dadds, M. R., & Rapee, R. M. (1996). Family treatment of childhood anxiety: A controlled trial. Journal of Consulting and Clinical Psychology, 64(2), 333–342. https://doi.org/10.1037/0022-006X.64.2.333
Barrett, P. M., Duffy, A. L., Dadds, M. R., & Rapee, R. M. (2001). Cognitive–behavioral treatment of anxiety disorders in children: Long-term (6-year) follow-up. Journal of Consulting and Clinical Psychology, 69(1), 135–141. https://doi.org/10.1037/0022-006X.69.1.135
Beck, J. S. (2011). Cognitive behavior therapy: Basics and beyond. Guilford Press.
Beidas, R. S., Benjamin, C. L., Puleo, C. M., Edmunds, J. M., Kendall, P. C. J. C., & Practice, B. (2010). Flexible applications of the coping cat program for anxious youth. 17(2), 142–153. https://doi.org/10.1016/j.cbpra.2009.11.002
Bennett-Levy, J. E., Butler, G. E., Fennell, M. E., Hackman, A. E., Mueller, M. E., & Westbrook, D. E. (2004). Oxford guide to behavioural experiments in cognitive therapy. Oxford University Press. https://doi.org/10.1093/med:psych/9780198529163.001.0001
Birmaher, B., Khetarpal, S., Brent, D., Cully, M., Balach, L., Kaufman, J., & Neer, S. M. (1997). The screen for child anxiety related emotional disorders (SCARED): Scale construction and psychometric characteristics. Journal of the American Academy of Child & Adolescent Psychiatry, 36(4), 545–553. https://doi.org/10.1097/00004583-199704000-00018
Bryant, R. A., Ekasawin, S., Chakrabhand, S., Suwanmitri, S., Duangchun, O., & Chantaluckwong, T. (2011). A randomized controlled effectiveness trial of cognitive behavior therapy for post-traumatic stress disorder in terrorist-affected people in Thailand. World Psychiatry : Official Journal of the World Psychiatric Association (WPA), 10(3), 205–209. https://doi.org/10.1002/j.2051-5545.2011.tb00058.x
Cohen, J. (1992). Quantitative methods in psychology: A power primer. Psychological Bulletin, 112(1), 155–159.
Corey, G. (2011). Theory and practice of group counseling. Nelson Education.
Crocetti, E., Klimstra, T., Keijsers, L., Hale, W. W., & Meeus, W. (2009). Anxiety trajectories and identity development in adolescence: A five-wave longitudinal study. Journal of Youth and Adolescence, 38(6), 839–849.
Cummings, C. M., & Fristad, M. A. J. J. o. a. c. p. (2012). Anxiety in children with mood disorders: a treatment help or hindrance? 40(3), 339–351. https://doi.org/10.1007/s10802-011-9568-5
David, D., Cristea, I., & Hofmann, S. G. (2018). Why cognitive behavioral therapy is the current gold standard of psychotherapy. Frontiers in Psychiatry, 9, 4. https://doi.org/10.3389/fpsyt.2018.00004
Essau, C. (2005). Frequency and patterns of mental health services utilization among adolescents with anxiety and depressive disorders. 22(3), 130-137. https://doi.org/10.1002/da.20115
Essau, C. A., Lewinsohn, P. M., Olaya, B., & Seeley, J. R. J. J. o. a. d. (2014). Anxiety disorders in adolescents and psychosocial outcomes at age 30. 163, 125–132. https://doi.org/10.1016/j.jad.2013.12.033
Ginsburg, G. S., & Drake, K. L. (2002). School-based treatment for anxious african-american adolescents: A controlled pilot study. Journal of the American Academy of Child and Adolescent Psychiatry, 41(7), 768–775. https://doi.org/10.1097/00004583-200207000-00007
Gregory, R. J. (2015). Psychological Testing: History, principle, and application. Pearson.
Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348–362. https://doi.org/10.1037/0022-3514.85.2.348
Gullone, E., & Taffe, J. (2012). The Emotion Regulation Questionnaire for Children and Adolescents (ERQ–CA): A psychometric evaluation. Psychological Assessment, 24(2), 409–417. https://doi.org/10.1037/a0025777
Hair, J. F., Black, W. C., Babin, B. J., Anderson, R. E., & Tatham, R. J. P. (2010). L.(2010). Multivariate data analysis.
Herzig-Anderson, K., Colognori, D., Fox, J. K., Stewart, C. E., & Masia Warner, C. (2012). School-based anxiety treatments for children and adolescents. Child and Adolescent Psychiatric Clinics of North America, 21(3), 655–668. https://doi.org/10.1016/j.chc.2012.05.006
Hollon, S. D., & Beck, A. T. (1994). Cognitive and cognitive-behavioral therapies. In A. E. Bergin & S. L. Garfield (Eds.), Handbook of psychotherapy and behavior change (pp. 428–466). Wiley.
Huberty, T. J. (2012a). Anxiety and depression in children and adolescents: Assessment, intervention, and prevention: Springer Science & Business Media.
Huberty, T. J. (2012b). The Developmental Psychopathology of Anxiety. In Anxiety and Depression in Children and Adolescents (pp. 29–53): Springer.
Isolan, L., Salum, G. A., Osowski, A. T., Amaro, E., & Manfro, G. G. (2011). Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED) in Brazilian children and adolescents. Journal of Anxiety Disorders, 25(5), 741–748. https://doi.org/10.1016/j.janxdis.2011.03.015
Juvonen, J., Le, V.-N., Kaganoff, T., & Augustine, C. H. (2004) Louay Constant Focus on the Wonder Years: Challenges Facing the American Middle School
Kendall, P. C., & Suveg, C. (2006). Treating anxiety disorders in youth. The Guilford Press.
Kendall, P. C., Compton, S. N., Walkup, J. T., Birmaher, B., Albano, A. M., Sherrill, J., . . ., & Gosch, E. (2010). Clinical characteristics of anxiety disordered youth. Journal of Anxiety Disorders, 24(3), 360-365. https://doi.org/10.1016/j.janxdis.2010.01.009
Kessler, R. C., Aguilar-Gaxiola, S., Alonso, J., Chatterji, S., Lee, S., Ormel, J., ..., & Wang, P. S. (2009). The global burden of mental disorders: an update from the WHO World Mental Health (WMH) surveys. Epidemiology and Psychiatric Sciences, 18(1), 23-33. https://doi.org/10.1017/S1121189X00001421
Lau, W. Y., Chan, C. K. Y., Li, J. C. H., & Au, T. K. F. (2010). Effectiveness of group cognitive-behavioral treatment for childhood anxiety in community clinics. Behaviour Research and Therapy, 48(11), 1067–1077. https://doi.org/10.1016/j.brat.2010.07.007
Mayers, A. (2013). Introduction to statistics and SPSS in psychology.
McLeod, S. A. (2012). Zone of proximal development. www.simplypsychology.org/Zone-of-Proximal-Development.html.
Merikangas, K. R., He, J. P., Burstein, M., Swanson, S. A., Avenevoli, S., Cui, L., Benjet, C., Georgiades, K., & Swendsen, J. (2010). Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication—Adolescent Supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry, 49(10), 980–989. https://doi.org/10.1016/j.jaac.2010.05.017
Mifsud, C., & Rapee, R. M. (2005). Early intervention for childhood anxiety in a school setting: Outcomes for an economically disadvantaged population. Journal of the American Academy of Child & Adolescent Psychiatry, 44(10), 996–1004. https://doi.org/10.1097/01.chi.0000173294.13441.87
Moran, K. (2016). Anxiety in the classroom: Implications for middle school teachers. Middle School Journal, 47(1), 27–32. https://doi.org/10.1080/00940771.2016.1059727
Mychailyszyn, M. P., Beidas, R. S., Benjamin, C. L., Edmunds, J. M., Podell, J. L., Cohen, J. S., & Kendall, P. C. (2011). Assessing and Treating Child Anxiety in Schools. Psychology in the Schools, 48(3), 223–232. https://doi.org/10.1002/pits.20548
National Statistical Office Thailand. (2021). The Survey on Mental Health and Migration 2011. http://www.nso.go.th/sites/2014en/Pages/survey/Social/Health/Mental-Health-and-Migration.aspx.
Petersen, T. J., Sprich, S. E., & Wilhelm, S. (Eds.). (2016). The Massachusetts general hospital handbook of cognitive behavioral therapy. Humana Press.
Phokhasawadi, S., Pornchaikate, A., & Wattanapailin,A. (2014). Cognitive behavior therapy to reduce symptoms of anxiety disorders with adolescents: Evidence-Based nursing. Journal of Nursing Science, 32(4), 7–14. https://he02.tci-thaijo.org/index.php/ns/article/view/28507.
Piaget, J. (1970). Science of education and the psychology of the child. Trans. D. Coltman.
Poonyakanok, T., & Tuicomepee, A. (2011). Review article: Stigma in context of professional psychological help seeking. Journal of Mental Health of Thailand., 19(1), 66–74.
Racine, N., Cooke, J. E., Eirich, R., Korczak, D. J., McArthur, B., & Madigan, S. (2020). Child and adolescent mental illness during COVID-19: A rapid review. Psychiatry Research, 292, 113307.
Robinson, K., Allen, F., Darby, J., Fox, C., Gordon, A. L., Horne, J. C., ..., & Logan, P. A. (2020). Contamination in complex healthcare trials: the falls in care homes (FinCH) study experience. BMC medical research methodology, 20(1), 1-6.
Rockhill, C., Kodish, I., DiBattisto, C., Macias, M., Varley, C., & Ryan, S. (2010). Anxiety disorders in children and adolescents. Current Problems in Pediatric and Adolescent Health Care, 40(4), 66–99. https://doi.org/10.1016/j.cppeds.2010.02.002
Runyon, K., Chesnut, S. R., & Burley, H. (2018). Screening for childhood anxiety: A meta-analysis of the screen for child anxiety related emotional disorders. Journal of Affective Disorders, 240, 220–229. https://doi.org/10.1016/j.jad.2018.07.049
Scaini, S., Rossi, F., Rapee, R. M., Bonomi, F., Ruggiero, G. M., & Incerti, A. (2022). The cool kids as a school-based universal prevention and early intervention program for anxiety: Results of a pilot study. International Journal of Environmental Research and Public Health, 19(2), 941. https://doi.org/10.3390/ijerph19020941
Shaffer, D. R. (2005). Social and personality development (5th ed.). Thomson Wadsworth.
Spence, S. H., Rapee, R., McDonald, C., & Ingram, M. (2001). The structure of anxiety symptoms among preschoolers. Behaviour Research and Therapy, 39(11), 1293–1316. https://doi.org/10.1016/S0005-7967(00)00098-X
Suveg, C., Kendall, P. C., Comer, J. S., & Robin, J. (2006). Emotion-focused cognitive-behavioral therapy for anxious youth: A multiple-baseline evaluation. Journal of Contemporary Psychotherapy, 36(2), 77–85.
Suveg, C., Sood, E., Comer, J. S., & Kendall, P. C. (2009). Changes in emotion regulation following cognitive-behavioral therapy for anxious youth. Journal of Clinical Child & Adolescent Psychology, 38(3), 390–401.
Suveg, C., & Zeman, J. (2004). Emotion regulation in children with anxiety disorders. Journal of Clinical Child and Adolescent Psychology, 33(4), 750–759. https://doi.org/10.1207/s15374424jccp3304_10
Trosper, S. E., Buzzella, B. A., Bennett, S. M., & Ehrenreich, J. T. (2009). Emotion regulation inyouth with emotional disorders: Implications for a unified treatment approach. Clinical Child and Family Psychology Review, 12(3), 234–254.
Whitfield, G. (2010). Group cognitive–behavioural therapy for anxiety and depression. Advances in Psychiatric Treatment, 16(3), 219–227. https://doi.org/10.1192/apt.bp.108.005744
Williams, M. M., Foo, K. H., & Haarhoff, B. A. (2006). Cultural considerations in using cognitive behaviour therapy with Chinese people: A case study of an elderly Chinese woman with generalised anxiety disorder.
Woodward, L. J., & Fergusson, D. M. (2001). Life course outcomes of young people with anxiety disorders in adolescence. Journal of the American Academy of Child & Adolescent Psychiatry, 40(9), 1086–1093. https://doi.org/10.1097/00004583-200109000-00018
Funding
This research was funded by the 90th Anniversary of Chulalongkorn University Scholarship, Graduate School, Chulalongkorn University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declared that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chonthannathi, B., Pisitsungkagarn, K. & Jurukasemthawee, S. The Effects of Cognitive Behavioral Group Therapy on Anxiety and Emotion Regulation in Thai Middle School Students. Int J Adv Counselling 44, 569–585 (2022). https://doi.org/10.1007/s10447-022-09482-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10447-022-09482-0