
Abstract
Background
No previous systematic review has examined the physical health benefits of playing golf or caddying.
Objective
To establish the influence of golf participation and physical health in golfers and caddies. More specifically, the review intended to explore the domains of cardiovascular, metabolic and musculoskeletal health, in addition to body composition.
Design
Systematic review.
Data Sources
Electronic literature searches were conducted using PubMed, SPORTDiscus and CINAHL databases in July 2021.
Eligibility Criteria
Experimental (randomised controlled trials, quasi-experiment, pre-post) and non-experimental (case–control, cross-sectional, cohort) articles relating to health and golf, written in English and published in peer-reviewed journals.
Results
Of the 572 articles initially identified, 109 full-text articles were assessed for eligibility with 23 meeting the inclusion criteria. Sixteen articles were rated ‘good 'and seven ‘fair’. The influence of golf on physical health was mixed, although various articles displayed improvements in balance, systolic blood pressure (SBP) and diastolic blood pressure (DBP), high density lipoprotein-cholesterol (HDL-C) and the ratio of HDL to total cholesterol within golfers. Caddies observed improvements in bone mineral density (BMD), stiffness index and strength. Most of the findings indicate that playing golf or caddying does not influence body mass index (BMI); however, playing golf can positively change other body composition markers such as lean and fat mass.
Conclusion
This review demonstrated that golf participation may be an effective method for improving musculoskeletal and cardiovascular health, although mixed findings were observed. Moreover, limited longitudinal evidence suggests that playing golf can positively impact metabolic health and the influence on body composition may be parameter dependent. Additionally, the initial evidence suggests that caddying may improve musculoskeletal health. However, the studies included were limited by their methodological inconsistencies such as: study design, participant demographics and intervention prescription.
PROSPERO Registration
CRD42021267664.
Similar content being viewed by others
This is the first systematic review of literature having investigated the influence of golf and caddying on physical health. |
Golf may be beneficial for musculoskeletal, metabolic and cardiovascular health; however, findings were mixed and likely dependent on the parameters assessed, in addition to golfer’s age, baseline health status and the golf activity performed. Caddying may be effective for improvements and maintenance of lower limb muscular strength. |
Future research should consider the intervention type and duration to understand the long-term impact of golf on physical health. |
1 Introduction
The popularity of golf is ever-growing, with a 2.3 million increase in on-course participation in Great Britain and Ireland in 2020 [1], with 2.2% of the population reported to play golf bi-weekly [2]. More females are participating in golf [1], which is also a game accessible to people of all ages, from the young to the old. Beyond golf participation, caddies contribute to the sport at all levels of the game, from recreational to professional. Typically, the caddie’s roles include, but are not limited to, carrying golf bags, attending to the flag stick, and providing strategic support to the golfer [3,4,5,6].
The average age of registered golfers within the UK is 41 years [1], with a forecasted 42% of golfers within Europe being older than 60 years [7]. The World Health Organisation (WHO) [8] predicts that in less than a decade, one in six people will be older than 60 years. Whilst ageing is not a direct cause for cardiovascular diseases (CVD) [9], it is associated with biological degeneration and senescence, which heightens the risk for disease and health complications [10]. In addition, falls are more common with advancing age and with an increase in frailty [11]. Furthermore, developing musculoskeletal disorders within older adults are also rising and are amongst the most common health issues [12, 13]. Within older adults, musculoskeletal disorders such as rheumatoid arthritis and osteoarthritis are associated with increased risk of falls [13, 14]. While the population is living longer, these extra years may not be spent in good health [8], thus limiting the health span—the phase of life without disability and free from serious illness [15]. A loss of physiological function attenuates functional status and heightens the risk of mortality and morbidity [16]. In turn, preservation of physiological function is paramount in the attainment of optimal longevity, health span [15] and in delaying future age-related chronic diseases. Therefore, effective lifestyle-behavioural strategies, such as physical activity (PA), have been considered as primary approaches in the attempt to slow the declines in physical health and functional independence, in order to increase health span [16].
Physical activity is a cost-effective, non-pharmacological method for improving health, supported by a curvilinear dose–response relationship between PA level and health benefits [17]. Golf presents an opportunity to increase PA and provides improvements in risk factors for CVD and metabolic and musculoskeletal health [18]. The metabolic cost and heart-rate responses through playing golf are dependent on numerous factors. Examples include riding an electric cart compared to carrying clubs or using a pull cart [19], carrying a bag with one or two straps [20, 21], and playing on a hilly course, although this is debated between studies [19, 22]. Additionally, caddies can be expected to carry a bag of at least 12.5 kg [3], which presents an additional physical challenge to walking alone, during an on-course round of golf. General golf is considered to be a moderate-intensity activity with a metabolic doequivalent (METs) of 4.8 [18, 23], with reports that a nine-hole golf round elicits 46% of peak MET for a healthy older (64 ± 8 years) population [24]. The relative intensity of activity varies depending on health status [24] and also increases progressively with age [25]. A systematic review identified that while a single round was sufficient to achieve the American College of Sports Medicine recommendations for energy expenditure, the mode of club transportation, age and skill level of golfers all contribute to variations in PA level [26].
A scoping review was recently conducted to establish the existing body of literature related to golf and health [18]. A variety of categories were explored concerning both physical and mental health, with a recommendation for a systematic review to be conducted to further the understanding between golf and health. Moreover, the focus has long been placed on golfers, while the effect of golf caddying on health has started to receive attention [3]. Given the absence of a focused systematic review on physical health and golf derived from peer-reviewed academic literature, the present systematic review aimed to establish the influence of golf participation and physical health in golfers and caddies. More specifically, we intended to explore the domains of cardiovascular, metabolic and musculoskeletal health, in addition to body composition.
2 Methods
This systematic literature review was conducted in accordance with the recommendations for the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement [27]. The systematic review was registered using the PROSPERO International database of systematic review protocols (Registration Number: CRD42021267664).
2.1 Search Terms and Criteria for Inclusion
An electronic literature search was conducted using PubMed, SPORTDiscus and CINAHL databases in July 2021, to identify available research studies that were related to golf and health. In all databases, a title and abstract search was conducted using a string of search terms that included: (Golf* OR Caddy OR Caddie OR Caddies OR Caddying) AND (Health OR Physical OR Cardiovascular OR Musculoskeletal OR MSK OR MSD OR Metabolic). Additional filters were applied to include studies only published in English. Primary source, peer-reviewed articles were eligible to be included if they contained data relating to golf and health. Specific inclusion criteria were as follows:
-
Peer-reviewed articles.
-
Primary research articles with any study designs (i.e., observational, cross-sectional, experimental studies) that presented a non-golf control group (cross-sectional) or determined changes (cohort or experimental) with statistical analyses.
-
Golfers of any age and skill level, including both competitive and recreational golfers.
-
Caddies of any age and level.
-
All forms of on-course and off-course golf (18 holes, nine holes, short-form golf, driving ranges, etc.).
-
English language studies.
-
Assessed markers of physical health pertaining to the domains of cardiovascular, metabolic, musculoskeletal health and body composition.
Conference proceedings, reviews, clinical commentaries, case reports, theses and dissertations were excluded. Titles and abstracts were reviewed independently by two authors (AJB and GGS) for relevance, followed by full-text screening to assess eligibility based on the inclusion and exclusion criteria. Reference lists of relevant reviews were screened for any additional articles that may have been missed from the electronic database search (AJB and GGS). During the review process, a third author (AKW) arbitrated any uncertainties in study inclusion.
2.2 Data Extraction
Included articles and relevant data were extracted into a custom Microsoft Excel sheet (Version 2016) by two authors independently (AJB and GGS). Extracted data included: (1) study details, such as authors, date of publication and study design; (2) participant characteristics, such as golf status (i.e., golfer or caddie), age, sex and skill level; (3) cardiovascular measurements including systolic (SBP) and diastolic blood pressure (DBP), cardiac function, inflammatory blood markers, maximum oxygen uptake (\(\dot{V}{\text{O}}_{2\max }\)) and associations with CVD risk; (4) musculoskeletal variables including balance, flexibility, muscle mass, thickness, strength and endurance, bone mineral density (BMD), bone mineral content (BMC) and physical competency measures; (5) metabolic variables including blood lipid profiles, bone metabolic markers and bone resorption rates; (6) body composition measurements including body mass index (BMI), fat mass, abdominal skinfold thickness and waist circumference.
2.3 Data Analysis and Quality Assessment
Narrative data analysis was conducted in each of the four domains described previously. The National Heart, Lung, and Blood Institute (NHLBI) risk assessments tools were used to assess the quality of included articles as per the NHLBI guidelines [28]. The quality assessment was conducted by one author (AKW) and then confirmed by a second author (AJB). If there was any uncertainty regarding the grade of study quality, the assessors conferred to reach an agreement. This tool contains 14 items with questions returning a ‘Yes’, ‘No’ or ‘Not Reported answer’.
3 Results
3.1 Study Selection
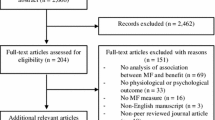
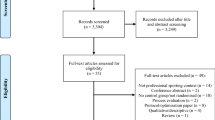
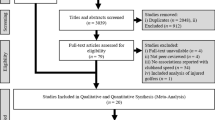
Of the 572 articles identified, 109 full-text articles were assessed for eligibility with 23 meeting criteria and included in the full-text review (Fig. 1). Sixteen articles were rated as good quality and seven fair, and no articles were considered to have any research fatal flaws. Most articles included musculoskeletal measures (N = 16) along with body composition measures (N = 15). Fewer studies included measures of a cardiovascular nature (N = 5) and metabolic markers (N = 6), whereby the focus was predominantly on blood lipid profile. There was a total of 14 non-experimental studies and nine intervention studies (Table 1). See Table 2 for summary details of the interventions employed.

PRISMA flow diagram of the exclusion process and study results
3.2 Musculoskeletal Effects
An overview of results is shown in Table 1. Sixteen studies included measures of a musculoskeletal nature, including strength and endurance measures [29,30,31,32,33,34,35,36], BMD or BMC [29, 34, 37, 38], balance and stability measures [30, 36, 39,40,41,42], muscle mass and thickness [35, 37, 43], flexibility and mobility [36], or physical competency measures [30, 32, 33, 44]. Musculoskeletal strength and endurance results were mixed, particularly amongst cross-sectional studies, where Stockdale et al. [33] observed no statistically significant differences in grip (golfers: 0.33 ± 0.06 N/kg; non-golfers: 0.29 ± 0.06 N/kg) or quadriceps strength between golfers and non-golfers (golfers: 2.78 ± 0.74 N/kg; non-golfers: 2.69 ± 0.83 N/kg). Chang et al. [29] also identified no significant difference in grip strength in golfers in comparison to control subjects. Mixed results were observed for intervention studies, whereby no significant changes were observed in grip strength in age-matched participants (golf mean difference = 0.85 kg, 95% confidence interval (CI): 0.04–1.67); control mean difference = 1.26 kg, 95% CI 0.40–2.13) [32]. Positive changes were, however, noted in one golf-training study where static back-extension time increased in the golf training group (from 93 to 101 s), whereas no change was observed for controls (91–89 s) [36].
BMD results were mostly non-significant; Chang et al. [29] noted 6.7% greater lumbar BMD in golfers than control—however, total body and hip BMD were similar. Other studies with golfers found no significant differences in BMD [37, 38]. Stability and balance measures were largely positive for golfing groups, whereby improvements were shown after training (8.9% improvement on step test [30]) and when analysed cross-sectionally in comparison to a control population [39, 41, 42]. Despite a low number of papers with muscle mass and thickness measures, results were largely positive, with increased muscle mass noted in the arms [37] and increased muscle thickness in golfers in comparison to non-golfers [43]. Mixed results were shown for physical competency measures, where no change was observed in walking speed after a golf programme [32]; however, improvements in timed up-and-go (TUG) tests were observed [33] or were greater than in non-golfers (13.3%) [30].
Studies in caddies mostly showed positive results, with Achilles tendon stiffness index greater in caddies across three age groups in comparison to control participants [35]. Additionally, caddies demonstrated increased quadriceps strength [34, 35], with improvements in BMD also observed [34].
3.3 Cardiovascular Effects
Five studies considered cardiovascular measures (Table 1), including DBP and SBP [36, 45, 46], resting heart rate and aerobic performance [36, 47], and risk of cardiovascular disease [48, 49]. In the large cohort study conducted by Müller-Riemenschneider et al. [46], golf was associated with increased DBP in both models evaluated (Model 1: Effect size = 2.04, 95% CI 0.44–3.64; Model 2: Effect size = 1.85, 95% CI 0.28–3.42). In other studies where SBP and DBP reduced after a golf intervention [45], it should be noted that the quality of the study was only fair, or there was a trend towards reducing a high DBP only when subjects with a pre-intervention high DBP were considered (between group differences of – 3 mmHg in favour of golf intervention) [36]. Both studies that observed a cardiovascular disease found golf was not associated with disease incidence [48, 49]. It is, however, to be noted that the cross-sectional study only made this comparison as a single time point, and thus cannot determine causality [49]. In addition, aerobic performance determined through \(\dot{V}{\text{O}}_{2\max }\) [45] or 6-min walking test did not differ between golfers and controls [50], while submaximal exercise performance improved after golf training with lower SBP, HR at 100 W [45], and lower oxygen consumption, HR and lactate at 7 METs [36].
3.4 Metabolic Effects
Six studies included measures of a metabolic nature (Table 1). This included measures of blood lipid profile (total, high-density lipoprotein cholesterol [HDL], low-density lipoprotein cholesterol [LDL] and triglycerides) [36, 46, 47, 49] or within a caddy population, measures of bone metabolic markers [34] or bone resorption rates through urinary pyridinoline and deoxypyridinoline levels [35]. Mixed results were observed for blood lipid profiles, including no significant associations with golf [46], significantly higher odds of ever having high cholesterol – although not when controlled for age [49], positive results for HDL levels (training effect-adjusted mean difference between groups 0.05 mmol/L (95% CI 0.00–0.10); HDL-C improvement of 5 mg/dL) and the ratio of HDL to total cholesterol (training effect-adjusted mean difference between groups 1.2% (95% CI 0.2–2.2)) [36, 47]. Urinary pyridinoline and deoxypyridinoline levels were found to not increase in caddies in comparison to controls pre- and post-menopause [35]. However, no significant trends were identified in bone metabolic markers [34].
3.5 Body Composition Effects
BMI data were included in 12 studies (Table 1). Mixed results were observed with no differences in BMI when considered cross-sectionally [33, 35, 39, 46, 49, 51], with only Herrick et al. [43] noting lower BMI in golfers (24.8 ± 2.5 kg·m−2) in comparison to controls (27.9 ± 3.5 kg·m−2). Longitudinal studies showed similar outcomes for BMI measurements, with significant reductions noted in fewer studies [36] than those that had no change or differences between groups [33, 34, 45, 47]. Studies that measured lean or fat mass largely found positive results, including a − 8% change in abdominal skin fold measurement [36, 37] rather than no change [29].
4 Discussion
This systematic review investigated the effects that golf participation has on physical health, specifically musculoskeletal, cardiovascular and metabolic health and body composition. Although a previous scoping review has outlined the physical health benefits that golf can provide for an individual, further research was required to systematically describe the relationship between golf participation and physical health [18]. To our knowledge, this is the first systematic review addressing the impact that golf participation, including golf play and caddying, has on cardiovascular, metabolic and musculoskeletal health, as well as body composition. Overall, the review highlighted that golf play can, in some instances, positively impact measures of physical health; however, findings across domains were mixed. Furthermore, when considering the population of golf caddies, findings highlighted that caddying may positively affect musculoskeletal health, although research remains limited in this population.
4.1 Musculoskeletal Effects
4.1.1 Muscular Strength and Size
Golf may be beneficial for the preservation of muscle mass and thickness. However, it must be noted that findings conflicted regarding the lower limbs, with one article observing similar muscle mass in young male golfers (29 ± 1 years) and controls [37]. In contrast, a later study demonstrated that older female golfers (69 ± 4 years) had larger relative quadriceps muscle thickness than non-golfers [43]. The latter observation is of particular importance, since age is associated with sex-independent reductions in the muscle/body weight ratio [52]. Sarcopenia, an age-related loss of skeletal muscle mass and strength [53], has been demonstrated through meta-analytical study to be associated with increased falls and fractures in older adults [54].
While hormonal changes are in part responsible for sarcopenia, environmental declines in PA are also contributory [53]. Golf offers the possibility for increasing PA of a light-moderate intensity [26], which may contribute towards the PA guidelines published by the WHO [55]. Thus, golf participation can be encouraged in order to achieve PA recommendations [26]. It is possible that with increasing PA that is likely to occur with on-course golf activity [56], golf may provide a stimulus for lower limb muscular hypertrophy. While this proposal relates to muscle thickness from limited research, the potential benefits of golf did not extend to muscular strength. From the four studies that investigated muscular strength in golfers, the consensus was that there was similar grip strength between golfers and non-golfers. Similarly, specific to lower body muscular strength, only two studies have been conducted and both found that golf was not beneficial for either quadriceps strength [33] or peak hip abductor force [30]. Golfers were reported to have walked the course, with one study describing that clubs were transported using a pushcart [30], which was outlined within the original methodological protocol article [57]. Although the METs for walking and pulling clubs with a cart (5.3 METs) are greater than walking while carrying clubs (4.3 METs) [23], the latter mode may require an additional effort. Indeed, caddies can be expected to carry a bag of at least 12.5 kg [3], and this may, in part, explain contrasting observations in the golfing literature, since hand grip and quadriceps strengths were greater in caddies than in non-caddies [34, 35]. Through cross-sectional observations, Hoshino et al. [35] reported in a small sample of long-term golf caddies who carry clubs that quadriceps strength was greater in caddies by 18.1 kg (difference in means) than in controls. The consequential benefits that may arise from carrying an additive load rather than solely walking are promising, and are likely to also contribute towards the PA guidelines, with the inclusion of strength-based exercise on at least 2 days per week [17, 55].
Additionally, drawing comparisons between golfers and caddies is challenging as the conflicting findings may be due, but not limited to, the differences in the transportation of clubs, the volume of activity completed, and/or the participant demographics. Indeed, the exercise stimulus may not have been sufficient in the longitudinal study [30] and the older aged population used by Stockdale et al. [33] (see Tables 1 and 2 for descriptions). Moreover, previous research has indicated that the step count completed by golfers was 11,948 ± 1,781 per round [58], while caddies have been reported to complete 20,499 ± 812 per round [34]. While the variation in activity is noteworthy, it is of course important to note that the golf course and skill level would influence this.
4.1.2 Balance
Most studies that investigated balance demonstrated a positive influence from golf. Proactive balance tests, described as anticipation of predicted disturbances [59], including functional reach, were greater in golfers [39], and the TUG test was faster in golfers than in non-golfers [33], improving by 13.3% after 12 weeks of golf practice [30]. As noted by Stockdale et al. [33], physical performance from the TUG test indicated that non-golfers were below the threshold and consequently classed as sarcopenic, whereas the golfers exceeded this threshold for the prediction of sarcopenia. As a test of functional ability [60], the TUG test is an important predictor of falls in seniors [61], and the potential benefits from golf for superior functional ability are welcomed. Other performance tests, such as the Berg Balance Scale (BBS), considered the gold-standard for balance assessments [59, 62], indicated further benefits of golf. Schachten and Jansen [40] found that 10 weeks of golf training improved BBS in middle-aged stroke survivors. Still, similar improvements were also noted for the parallel social communications group, although this study lacked randomisation into each treatment arm. In contrast, a two-group pre-test post-test golf intervention for 20 weeks suggested static and dynamic balance did not differ [36]. Thus, more intervention studies are required with adequate randomisation to determine the influence of golf on functional balance tests. One study reported a significantly lower incidence rate ratio (IRR) of falls for golfers compared with other leisure-time physical activities (LTPAs) when PA of multiple intensities was considered [44]. Although this association was dampened after controlling for LTPA and history of falls, this may suggest that a prominent element of golf (i.e., PA) is an important and mediating factor in the risk of falls. This information is of significant clinical relevance, since falls are the second leading cause of unintentional mortality [63]. The number of deaths from falls within England during 2019 increased with age and totalled 6,138 in those > 40 years of age [64]. The ramifications for golf to aid in the preservation of muscular performance and balance are promising, with the intention of maintaining functional ability and, by extension, healthy ageing [65].
4.1.3 Bone Mineral Density
Studies identified within the review highlight that playing golf has minimal effects on total body BMD or BMC [29, 37, 38]. The influence of regional BMD is contradictory, however, with Chang et al. [29] reporting 6.7% greater lumbar spine BMD in female elite golfers compared to controls. However, Jang et al. [38] and Dorado et al. [37] reported no differences in spine BMD when comparing male golfers participating in screen golf against control subjects. It should be noted that screen golf does not take into consideration walking on the golf course and the transportation of golf clubs; therefore, this may explain the conflicting findings. However, the reporting of transportation of clubs in other studies was lacking, thus it is not clear at present whether walking a course whilst carrying is influential. Sex differences may also be contributory, since the rate of production and loss in BMD differs between women and men [66]. This may help to provide some insight as to why Chang et al. [29] observed greater spine BMD in golfers, while male golfers [38] of a similar and younger age were comparable to controls.
In consideration of golf caddies, positive findings were observed in relation to BMD and Achilles stiffness index [34, 35]. Specifically, Goto and colleagues [34] reported that female golf caddies, at a pre-menopausal stage, significantly increased lumbar spine BMD at 6 and 12 months and proximal femur BMD following 12 months of caddying. When taking into consideration the activity levels of these two groups, caddies walked over threefold the distance of the desk workers. Moreover, since oestrogen deficiency plays a key role in a net loss of bone [67], bone production in the pre-menopausal state may be important for the preservation of BMD, facilitated by caddying.
4.2 Cardiovascular Effects
From the limited literature exploring the influence of golf on blood pressure, the findings may be conditional on both the training intervention and baseline blood pressure. Two studies observed reductions in SBP and DBP [45, 47], which represent beneficial changes since high blood pressure is a modifiable risk factor for CVD [68]. However, the participants completed the golf training as a vacation, and thus stress may confound the association between golf training and markers of health, as suggested by the authors, concomitant with reduced fibroblast growth factor 21 (FGF-21) [47]. In contrast, a longer intervention of 20 weeks, which may better represent the influence of sustained golf play, suggested that blood pressure did not change based on group data [36]. However, subgroup analysis in those with the highest blood pressures observed -3 mmHg in DBP in the golf group compared to controls. While this observation is not supported by cross-sectional research having shown a positive association between golf and DBP [46], it may support the proposition through meta-analysis that those with hypertension may benefit the most from endurance training [69]. Moreover, the long-term impact of golf on CVD risk requires further substantiation, since one article identified no significant association with CVD incidence [48]. Additional work, whilst not included in the review due to a lack of a no-golf comparator/reference group, suggests that mortality is approximately 60% compared to that of the estimated general population [70]. Thus, future work is required to determine the long-term health implications and associated risk for CVD following golf participation.
Cardiorespiratory fitness (\(\dot{V}{\text{O}}_{2\max }\)) is a strong predictor of mortality in men and women [71]. However, \(\dot{V}{\text{O}}_{2\max }\) did not change after 1 week [45] or 20 weeks [36] of golf training, and nor did maximum power output (Wmax) [45]. It is possible that the intensity of golf was not sufficient to induce central adaptations in left ventricular function [45] and/or peripheral adaptation to elicit changes in aerobic fitness. However, low volume, high-intensity interval exercise in older men has yielded benefits in \(\dot{V}{\text{O}}_{2\max }\) [72] and peak power output [73]. Nonetheless, studies in this review did observe improvements in submaximal exercise performance [36, 45] and, thus, this suggests less cardiovascular demand with superior exercise economy after the golf training, despite no changes in \(\dot{V}{\text{O}}_{2\max }\).
4.3 Metabolic Effects
Several metabolic variables were investigated (Table 1) but with mixed findings, making it challenging to propose a consensus concerning metabolic health parameters. However, more frequently investigated was the blood lipid profile, with reports of no association with golf and triglycerides, HDL cholesterol and LDL cholesterol [46]. Intervention studies, however, reported increased HDL-C [47] and the ratio of HDL to total cholesterol [36] following golf training. This is encouraging since HDL is an important predictor of CVD risk and higher HDL is inversely associated with coronary heart disease [74, 75]. However, although cross-sectional analysis golfers were at greater odds of being diagnosed with high cholesterol than non-golfers [49], this difference was abolished when controlling for both age and physical activity, which may be stronger determinants of total cholesterol than golf participation.
The disparity in results relating to blood lipid profile may be due in part to study designs. Both intervention studies, irrespective of duration, provided positive results after golf training, whereas the cross-sectional studies, which are likely influenced by confounding between-subject variables, were negligible or negative. Thus, additional confirmatory studies concerning long-term golf play and metabolic health are required.
4.4 Body Composition Effects
Most cross-sectional [33, 39, 46, 49, 51] and intervention [45, 47] studies indicated that playing golf or caddying [34, 35] does not impact BMI. Some studies, however, have suggested the contrary, that BMI was lower in golfers than controls [43], reduced following a 20-week golf season [36], or increased by 0.7% following at least 15 × 90-min golf classes over a 5-month period [31]. Nevertheless, the true physiological significance of a 0.17 kg.m2 increase as reported in the latter warrants mention. These studies observing changes in BMI were in the minority, but the contradiction may arise from the methodological inconsistencies of the golf interventions and participant demographics, making it difficult to draw sound conclusions in relation to the impact of within-subject long-term golf play and BMI. Indeed, BMI is associated with all-cause mortality in a J-shaped relationship [76], and an apparent lack of evidence to suggest golf produces a universal change in BMI, which could be inferred as both beneficial and deleterious depending on baseline BMI.
BMI may not be suitable for differentiating fat mass from lean mass, especially when assessing BMI change [77]. The influence of golf on body composition from cross-sectional studies was equally undecided as to whether golf is beneficial [29, 37, 38, 46]. From intervention studies, fat mass did not differ between golfers and controls in two intervention studies; however, they were only 1 week in duration [45, 47]. In contrast, a more substantial intervention period of 20 weeks yielded reductions in abdominal skinfold thickness and waist circumference [36]. These observations are of particular importance since central adiposity/waist circumference is a key component of the metabolic syndrome [78], which represents a constellation of risk factors associated with greater risk for developing CVD and type 2 diabetes mellitus [79]. Before a stronger conclusion can be elucidated, however, more intervention studies that are of sufficient duration are necessary.
4.5 Strengths and Limitations
The current review provides valuable insight into the health benefits of playing golf and caddying; however, there are some noteworthy limitations to consider. Whilst efforts were made to ensure a rigorous and thorough search process, it is possible that some articles may have been missed, which may include peer-reviewed journal articles not written in English. The reviewed studies provided a variety of study designs and wide heterogeneity. Additionally, the golfers and caddies differed in sex, age and sample size, and, as a result, a meta-analysis was not feasible at this moment in time. The review was limited to four outcome-measure categories in relation to health; therefore, there may be other outcome measures relevant to the health benefits of golf and caddying. However, the intention was to focus on physical health; other studies should continue to establish the influence of golf on mental health and wellbeing.
The NHLBI risk assessments tools demonstrated that the quality of included studies was ‘fair’ to ‘good’. In relation to intervention studies, approximately 70% were rated ‘good’, suggesting the current evidence is strong. While many longitudinal studies were rated ‘good’, these studies varied considerably with regard to: heterogeneity of participants, duration of the intervention (1 week to 12 months), golf activity performed, and frequency of activity. It is, therefore, difficult to draw sound recommendations regarding duration, activity and frequency of golf interventions to improve health. A limited number of studies (N = 2) investigated the health benefits of caddying; nevertheless, the initial evidence suggests that golf caddying may have a positive impact on musculoskeletal health. To draw stronger conclusions within this area, however, additional longitudinal research is required, particularly within the male population. Furthermore, a limited number of studies (N = 5) reported specifically that golfers or caddies walked the course [30, 33, 34, 36, 48], and only two studies indicated the golfers’ club transportation method [30, 48, 57]. As previously discussed, the metabolic demand of golf varies depending on the golfer’s club transportation choice and if they walk the course or use a motorized golf cart [23, 26]. Therefore, future golf course participation-related studies should take into consideration golfers’ and caddies’ mode of transportation (e.g., walking or using a motorised cart) and club transportation (e.g., carrying clubs, pulling or pushing a cart) on the golf course, when initially recruiting their sample. In addition, this information should be reported within studies to improve clarity, which will enable appropriate between-study key findings. Moreover, whilst beyond the direct scope of this review, interest has increased relating to the adverse effects of golf participation pertaining to injuries and musculoskeletal and cardiovascular risks, in addition to skin-related issues associated with golf participation [3, 18, 80, 81]. Accordingly, more studies are required to fully understand the depth and breadth of the impact that golf has on both players and caddies [3].
Beyond the limitations, this review is the first to systematically collate the literature in relation to the health benefits of playing golf and caddying. Thus, this review advances our understanding of the potential impact that playing golf and caddying can have on body composition and musculoskeletal, cardiovascular and metabolic health.
4.6 Conclusions
Golf may be an effective method for improving musculoskeletal, cardiovascular and metabolic health. Additionally, most of the evidence suggests that playing golf does not influence body composition (BMI). Yet, there was also evidence to suggest that golf was not beneficial for the domains studied, although this may be dependent on: the sample of golfers, study design, the length of the intervention, and the frequency of activity. Consequently, the influence of playing golf on physical health requires further study with consideration of such methodological factors. Furthermore, the initial evidence suggests that golf caddying may positively impact musculoskeletal health; however, it would be appropriate to conduct further investigations within this area due to the limited literature at present.
References
Articles included in the systematic review are denoted as *
R & A. 2020 GB&I Golf Participation Report. 2021.https://www.randa.org/en/news/2021/05/gbandi-golf-participation-report. Accessed 19 Jan 2022.
England Golf. Growing the Game of Golf in England. The Strategic Plan 2017/21. 2017. https://www.englandgolf.org/wp-content/uploads/2018/08/England-Golf-2017-21-Strategy.pdf
Adams KJ, Sevene T, Walsh J, et al. The golf caddie—the forgotten worker. J Phys Act Res. 2020;5:41–4. https://doi.org/10.12691/jpar-5-1-8.
Caddie Hall of Fame. About Caddying. https://caddiehalloffame.org/about-caddying. Accessed 19 Jan 2022.
Carey LM, Stone JA, Lavallee D. “Teamwork Done to a Tee”: a golf caddie’s perspective on their perceived role and associated skills. Int J Golf Sci. 2021;9:1–19.
Lavallee D, Bruce D, Gorley T. The golfer–caddie partnership: an exploratory investigation into the role of the caddie. Athl Insight Online J Sport Psychol. 2004;6:20–35.
Statista. Golf in Europe. 2021. https://www.statista.com/study/40473/golf-in-europe/. Accessed 19 Jan 2022.
World Health Organization (WHO). Ageing and health. 2021.https://www.who.int/news-room/fact-sheets/detail/ageing-and-health. Accessed 22 Oct 2021.
Strait JB, Lakatta EG. Aging-associated cardiovascular changes and their relationship to heart failure. Heart Fail Clin. 2012;8:143–64. https://doi.org/10.1016/j.hfc.2011.08.011.
North BJ, Sinclair DA. The intersection between aging and cardiovascular disease. Circ Res. 2012;110:1097–108. https://doi.org/10.1161/CIRCRESAHA.111.246876.
World Health Organization (WHO). WHO Global Report on Falls Prevention in Older Age. 2008.
Stubbs B, Binnekade TT, Soundy A, et al. Are older adults with chronic musculoskeletal pain less active than older adults without pain? A systematic review and meta-analysis. Pain Med. 2013;14:1316–31. https://doi.org/10.1111/pme.12154.
Afrin N, Honkanen R, Koivumaa-Honkanen H, et al. Role of musculoskeletal disorders in falls of postmenopausal women. Osteoporos Int. 2018;29:2419–26. https://doi.org/10.1007/s00198-018-4631-5.
Rubenstein LZ, Josephson KR. Falls and their prevention in elderly people: what does the evidence show? Med Clin North Am. 2006;90:807–24. https://doi.org/10.1016/j.mcna.2006.05.013.
Seals DR, Melov S. Translational Geroscience: Emphasizing function to achieve optimal longevity. Aging (Albany NY). 2014;6:718–30. https://doi.org/10.18632/aging.100694.
Seals DR, Justice JN, Larocca TJ. Physiological geroscience: targeting function to increase healthspan and achieve optimal longevity. J Physiol. 2016;594:2001–24. https://doi.org/10.1113/jphysiol.2014.282665.
Uk Government. UK Chief Medical Officers’ Physical Activity Guidelines. 2019.
Murray AD, Daines L, Archibald D, et al. The relationships between golf and health: a scoping review. Br J Sports Med. 2017;51:12–9. https://doi.org/10.1136/bjsports-2016-096625.
Kras JM, Larsen BT. A comparison of the health benefits of walking and riding during a round of golf. Int Sport J. 2002;6:112.
Ikeda ER, Cooper L, Gulick P, et al. The metabolic cost of carrying a single- versus double-strap golf bag. J strength Cond Res. 2008;22:974–7. https://doi.org/10.1519/JSC.0b013e31816f6f2e.
Holland CJ, Godwin MS. The metabolic demand of external load carriage in golfers: a comparison of a single versus double-strap golf bag. J Sports Med Phys Fitness. 2019;59:1963–7. https://doi.org/10.23736/S0022-4707.19.09668-3.
Zunzer SC, von Duvillard SP, Tschakert G, et al. Energy expenditure and sex differences of golf playing. J Sports Sci. 2013;31:1045–53. https://doi.org/10.1080/02640414.2013.764465.
Ainsworth BE, Haskell WL, Herrmann SD, et al. 2011 compendium of physical activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011;43:1575–81. https://doi.org/10.1249/MSS.0b013e31821ece12.
Dobrosielski DA, Brubaker PH, Berry MJ, et al. The metabolic demand of golf in patients with heart disease and in healthy adults. J Cardiopulm Rehabil. 2002;22:96–104. https://doi.org/10.1097/00008483-200203000-00008.
Broman G, Johnsson L, Kaijser L. Golf : a high intensity interval activity for elderly men. Aging Clin Exp Res. 2004;16:375–81.
Luscombe J, Murray AD, Jenkins E, et al. A rapid review to identify physical activity accrued while playing golf. BMJ Open. 2017;7: e018993. https://doi.org/10.1136/bmjopen-2017-018993.
Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst Rev. 2015;4:1–9.
The National Heart, Lung and Blood Institute (NHLBI) Risk Assessment Tool. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. Accessed 30 Jul 2021.
*Chang RPY, Briffa KN, Edmondston SJ. Bone mineral density and body composition in elite female golf and netball players. Eur J Sport Sci. 2013;13:183–90. https://doi.org/10.1080/17461391.2011.606840.
*Du Bois AM, Marcione NA, Powers CM, et al. The effects of a comprehensive golf training program on measures of physical performance and dynamic balance in older military veterans. Int J Golf Sci. 2021;9:1–16.
*Podstawski R, Markowski P, Choszcz D, et al. Effectiveness of martial arts training vs. Other types of physical activity: differences in body height, body mass, bmi and motor abilities. South African J Res Sport Phys Educ Recreat. 2017;39:111–33. https://doi.org/10.10520/EJC-65341570a.
*Shimada H, Lee S, Akishita M, et al. Effects of golf training on cognition in older adults: a randomised controlled trial. J Epidemiol Community Health. 2018;72:944–50. https://doi.org/10.1136/jech-2017-210052.
*Stockdale A, Webb N, Wootton J, et al. Muscle strength and functional ability in recreational female golfers and less active non-golfers over the age of 80 years. Geriatrics. 2017. https://doi.org/10.3390/geriatrics2010012.
*Goto S, Ishima M, Shimizu M, et al. A longitudinal study for femoral neck bone mineral density increases in premenopausal caddies using dual-energy X-ray absorptiometry. J Bone Miner Metab. 2001;19:125–30. https://doi.org/10.1007/s007740170051.
*Hoshino H, Kushida K, Yamazaki K, et al. Effect of physical activity as a caddie on ultrasound measurements of the Os calcis: a cross-sectional comparison. J Bone Miner Res. 1996;11:412–8. https://doi.org/10.1002/jbmr.5650110316.
*Parkkari J, Natri A, Kannus P, et al. A controlled trial of the health benefits of regular walking on a golf course. Am J Med. 2000;109:102–8. https://doi.org/10.1016/s0002-9343(00)00455-1.
*Dorado C, Sanchis Moysi J, Vicente G, et al. Bone mass, bone mineral density and muscle mass in professional golfers. J Sports Sci. 2002;20:591–7. https://doi.org/10.1080/026404102320183149.
*Jang J-H, Jee Y-S, Oh H-W. Frequency-effect of playing screen golf on body composition and golf performance in middle-aged men. J Exerc Rehabil. 2014;10:271–8. https://doi.org/10.12965/jer.140140.
*Gao KL, Hui-Chan CWY, Tsang WWN. Golfers have better balance control and confidence than healthy controls. Eur J Appl Physiol. 2011;111:2805–12. https://doi.org/10.1007/s00421-011-1910-7.
*Schachten T, Jansen P. The effects of golf training in patients with stroke: a pilot study. Int Psychogeriatrics. 2015;27:865–73. https://doi.org/10.1017/S1041610214002452.
*Tsang WWN, Hui-Chan CWY. Effects of exercise on joint sense and balance in elderly men: Tai Chi versus golf. Med Sci Sports Exerc. 2004;36:658–67. https://doi.org/10.1249/01.mss.0000122077.87090.2e.
*Tsang WWN, Hui-Chan CWY. Static and dynamic balance control in older golfers. J Aging Phys Act. 2010;18:1–13. https://doi.org/10.1123/japa.18.1.1.
*Herrick I, Brown S, Agyapong-Badu S, et al. Anterior thigh tissue thickness measured using ultrasound imaging in older recreational female golfers and sedentary controls. Geriatr. 2017. https://doi.org/10.3390/geriatrics2010010.
*Merom D, Stanaway FF, Handelsman DJ, et al. Swimming and other sporting activities and the rate of falls in older men: longitudinal findings from the Concord Health and Ageing in Men Project. Am J Epidemiol. 2014;180:830–7. https://doi.org/10.1093/aje/kwu199.
*Neumayr G, Lechleitner P. Effects of a one-week vacation with various activity programs on cardiovascular parameters. J Sports Med Phys Fitness. 2018;59:335–9. https://doi.org/10.23736/S0022-4707.18.08221-X.
*Müller-Riemenschneider F, Hong Y, Tan KHX, et al. The association of different types of leisure time physical activities with cardiometabolic outcomes in Singapore-findings from the multi-ethnic cohort study. Int J Environ Res Public Health. 2020. https://doi.org/10.3390/ijerph17239030.
*Neumayr G, Engler C, Lunger L, et al. Effects of a one-week vacation with various activity programs on metabolism and adipokines. Int J Sports Med. 2021;42:703–7. https://doi.org/10.1055/a-1297-4669.
*Porter AK, Schilsky S, Evenson KR, et al. The association of sport and exercise activities with cardiovascular disease risk: the atherosclerosis risk in communities (ARIC) study. J Phys Act Health. 2019;16:698–705. https://doi.org/10.1123/jpah.2018-0671.
*Stenner B, Mosewich AD, Buckley JD, et al. Associations between markers of health and playing golf in an Australian population. BMJ open Sport Exerc Med. 2019;5: e000517. https://doi.org/10.1136/bmjsem-2019-000517.
*Stroehlein JK, Vieluf S, Zimmer P, et al. Learning to play golf for elderly people with subjective memory complaints: feasibility of a single-blinded randomized pilot trial. BMC Neurol. 2021;21:200. https://doi.org/10.1186/s12883-021-02186-9.
*Webb N, Rowsome K, Ewings S, et al. A ‘Movement Screening Test’ of functional control ability in female recreation golfers and non-golfers over the age of 80 years: a reliability study. J Funct Morphol Kinesiol. 2018. https://doi.org/10.3390/jfmk3040054.
Proctor DN, Balagopal P, Nair KS. Symposium: the roles of nutrition, development and hormone sensitivity in the regulation of protein metabolism age-related sarcopenia in humans is associated with reduced synthetic rates of specific muscle proteins 1,2. J Nutr. 1998;128:351–5.
Walston JD. Sarcopenia in older adults. Curr Opin Rheumatol. 2012;24:623–7. https://doi.org/10.1097/BOR.0b013e328358d59b.
Yeung SSY, Reijnierse EM, Pham VK, et al. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. 2019;10:485–500. https://doi.org/10.1002/jcsm.12411.
World Health Organization (WHO). Physical activity. 2020. https://www.who.int/news-room/fact-sheets/detail/physical-activity. Accessed 19 Jan 2022.
Sorbie GG, Beaumont AJ, Williams AK, et al. The impact of the closure and reopening of golf courses in the United Kingdom on Wellbeing During the COVID-19 Pandemic: a multi-study approach. Front Sport Act Liv. 2021;3: 622171. https://doi.org/10.3389/fspor.2021.622171.
Du Bois AM, Marcione NA, Castle SC, et al. The golf intervention for veterans exercise (GIVE) study: Golf training program and study design—a methodological protocol. Int J Golf Sci. 2019;7:1–16.
Kobriger SL, Smith J, Hollman JH, et al. The contribution of golf to daily physical activity recommendations: how many steps does it take to complete a round of golf? Mayo Clin Proc. 2006;81:1041–3. https://doi.org/10.4065/81.8.1041.
Bergquist R, Weber M, Schwenk M, et al. Performance-based clinical tests of balance and muscle strength used in young seniors: a systematic literature review. BMC Geriatr. 2019;19:1–14. https://doi.org/10.1186/s12877-018-1011-0.
Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39:142–8. https://doi.org/10.1111/j.1532-5415.1991.tb01616.x.
Power V, Van De Ven P, Nelson J, et al. Predicting falls in community-dwelling older adults: a systematic review of task performance- based assessment tools. Psychother Pr Res. 2014;35:3–15.
Southard V, Dave M, Davis MG, et al. The Multiple Tasks Test as a predictor of falls in older adults. Gait Posture. 2005;22:351–5. https://doi.org/10.1016/j.gaitpost.2004.11.013.
World Health Organization (WHO). Falls. 2021. https://www.who.int/news-room/fact-sheets/detail/falls#:~:text=Theproblem&text=Anestimated 684 000 fatal,death%2Cafter roadtraffic injuries. Accessed 19 Jan 2022.
Office for National Statistics (ONS). Deaths from falls by age and local authority. 2021. https://www.ons.gov.uk/aboutus/transparencyandgovernance/freedomofinformationfoi/deathsfromfallsbyageandlocalauthority. Accessed 23 Jan 2022.
World Health Organization (WHO). World Report on Ageing and Health. 2015.
Alswat KA. Gender disparities in osteoporosis. J Clin Med Res. 2017;9:382–7. https://doi.org/10.14740/jocmr2970w.
Khosla S, Oursler MJ, Monroe DG. Estrogen and the skeleton. Trends Endocrinol Metab. 2012;23:576–81. https://doi.org/10.1016/j.tem.2012.03.008.
Fuchs FD, Whelton PK. High blood pressure and cardiovascular disease. Hypertension. 2020. https://doi.org/10.1161/HYPERTENSIONAHA.119.14240.
Cornelissen VA, Smart NA. Exercise training for blood pressure: a systematic review and meta-analysis. J Am Heart Assoc. 2013;2:1–9. https://doi.org/10.1161/JAHA.112.004473.
Farahmand B, Broman G, de Faire U, et al. Golf: a game of life and death–reduced mortality in Swedish golf players. Scand J Med Sci Sports. 2009;19:419–24. https://doi.org/10.1111/j.1600-0838.2008.00814.x.
Imboden MT, Harber MP, Whaley MH, et al. Cardiorespiratory fitness and mortality in healthy men and women. J Am Coll Cardiol. 2018;72:2283–92. https://doi.org/10.1016/j.jacc.2018.08.2166.
Grace F, Herbert P, Elliott AD, et al. High intensity interval training (HIIT) improves resting blood pressure, metabolic (MET) capacity and heart rate reserve without compromising cardiac function in sedentary aging men. Exp Gerontol. 2018;109:75–81. https://doi.org/10.1016/j.exger.2017.05.010.
Sculthorpe N, Herbert P, Grace F. One session of high-intensity interval training (HIIT) every 5 days, improves muscle power but not static balance in lifelong sedentary ageing men. Medicine (Baltimore). 2017;96:1–8. https://doi.org/10.1097/MD.0000000000006040.
Rader DJ, Hovingh GK. HDL and cardiovascular disease. Lancet. 2014;384:618–25. https://doi.org/10.1016/S0140-6736(14)61217-4.
Kannel WB, Dawber TR, Friedman GD, et al. Risk factors in coronary heart disease: the Framingham Study. Ann Intern Med. 1964. https://doi.org/10.7326/0003-4819-61-5-888.
Bhaskaran K, Santos-dos I, Leon DA, et al. Association of BMI with overall and cause-specific mortality: a population-based cohort study of 36 million adults in the UK. Lancet Diabetes Endocrinol. 2018;6:944–53. https://doi.org/10.1016/S2213-8587(18)30288-2.
Cornier MA, Després JP, Davis N, et al. Assessing adiposity: a scientific statement from the american heart association. Circulation. 2011;124:1996–2019. https://doi.org/10.1161/CIR.0b013e318233bc6a.
Alberti KGMM, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation. Int Circ. 2009;120:1640–5. https://doi.org/10.1161/CIRCULATIONAHA.109.192644.
Wilson PWF, D’Agostino RB, Parise H, et al. Metabolic syndrome as a precursor of cardiovascular disease and type 2 diabetes mellitus. Circulation. 2005;112:3066–72. https://doi.org/10.1161/CIRCULATIONAHA.105.539528.
Smith JA, Hawkins A, Grant-Beuttler M, et al. Risk factors associated with low back pain in golfers: a systematic review and meta-analysis. Sports Health. 2018;10:538–46. https://doi.org/10.1177/1941738118795425.
Robinson PG, Murray IR, Duckworth AD, et al. Systematic review of musculoskeletal injuries in professional golfers. Br J Sports Med. 2019;53:13–8. https://doi.org/10.1136/bjsports-2018-099572.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest
Graeme G. Sorbie, Alexander J. Beaumont, Ashley K. Williams and David Lavallee declare that they have no conflicts of interest relevant to the content of this review.
Ethics approval
Full ethics approval was granted from Abertay University School of Health Sciences Ethics Committee.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
GGS, AJB and AKW wrote the first draft of the manuscript. GGS and AJB conducted database searches and article identification. Data extraction was conducted by GGS, AJB and AKW, and methodological quality assessments were conducted by AKW and then confirmed by AJB. DL revised the original manuscript.
Data availability
There are no underlying data to share.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sorbie, G.G., Beaumont, A.J., Williams, A.K. et al. Golf and Physical Health: A Systematic Review. Sports Med 52, 2943–2963 (2022). https://doi.org/10.1007/s40279-022-01732-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-022-01732-w