
Abstract
Postprandial hyperlipidaemia is an important feature of diabetic dyslipidaemia and plays an important role in the development of cardiovascular disease in individuals with type 2 diabetes. Postprandial hyperlipidaemia in type 2 diabetes is secondary to increased chylomicron production by the enterocytes and delayed catabolism of chylomicrons and chylomicron remnants. Insulin and some intestinal hormones (e.g. glucagon-like peptide-1 [GLP-1]) influence intestinal lipid metabolism. In individuals with type 2 diabetes, insulin resistance and possibly reduced GLP-1 secretion are involved in the pathophysiology of postprandial hyperlipidaemia. Several factors are involved in the overproduction of chylomicrons: (1) increased expression of microsomal triglyceride transfer protein, which is a key enzyme in chylomicron synthesis; (2) higher stability and availability of apolipoprotein B-48; and (3) increased de novo lipogenesis. Individuals with type 2 diabetes present with disorders of cholesterol metabolism in the enterocytes with reduced absorption and increased synthesis. The increased production of chylomicrons in type 2 diabetes is also associated with a reduction in their catabolism, mostly because of a reduction in activity of lipoprotein lipase. Modification of the microbiota, which is observed in type 2 diabetes, may also generate disorders of intestinal lipid metabolism, but human data remain limited. Some glucose-lowering treatments significantly influence intestinal lipid absorption and transport. Postprandial hyperlipidaemia is reduced by metformin, pioglitazone, alpha-glucosidase inhibitors, dipeptidyl peptidase 4 inhibitors and GLP-1 agonists. The most pronounced effect is observed with GLP-1 agonists, which reduce chylomicron production significantly in individuals with type 2 diabetes and have a direct effect on the intestine by reducing the expression of genes involved in intestinal lipoprotein metabolism. The effect of sodium–glucose cotransporter 2 inhibitors on intestinal lipid metabolism needs to be clarified.
Graphical abstract

Similar content being viewed by others

Introduction
For the past few years, growing evidence has shown that the intestine plays a significant role in the metabolic disorders observed in individuals with type 2 diabetes. Postprandial hyperlipidaemia is an important feature of diabetic dyslipidaemia and is likely to promote atherosclerosis [1, 2]. Although there is no consensus definition of postprandial hyperlipidaemia, it is characterised by prolonged and increased levels of lipids, especially triglycerides and triglyceride-rich lipoprotein levels, after a meal. Postprandial hyperlipidaemia is characterised by the accumulation after meals of remnant lipoprotein particles, which cross the endothelial barrier and accumulate in the arterial wall, where they have pro-atherogenic effects including rapid cholesterol accumulation in macrophages [3]. For these reasons, it is suspected that postprandial hyperlipidaemia contributes significantly to the increased cardiovascular risk in individuals with type 2 diabetes [3]. Over the past few years, data have accumulated showing that intestinal lipid metabolism is modified significantly in individuals with type 2 diabetes. Although the pathophysiology of postprandial hyperlipidaemia has not been entirely clarified in type 2 diabetes, some specific abnormalities have been described, leading to consideration of some interesting therapeutic targets for improving postprandial lipid metabolism in individuals with type 2 diabetes. In this review, after a brief overview of normal intestinal lipid metabolism and its regulation by insulin and intestinal hormones (glucagon-like peptide-1 [GLP-1], glucagon-like peptide-2 [GLP-2] and gastric inhibitory polypeptide [GIP]), disorders of intestinal lipid absorption and transport in type 2 diabetes are discussed. Finally, the effects of glucose-lowering treatments on intestinal lipid absorption and transport are described.
Overview of normal lipid absorption and intestinal lipoprotein metabolism
Intestinal digestion of dietary lipids
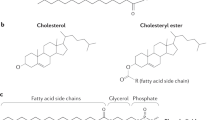
Hydrolysis of dietary lipids is performed by different lipases, including pancreatic lipase [4, 5]. In the intestinal lumen, triglycerides are hydrolysed to non-esterified fatty acids (NEFAs) and 2-monoacylglycerol. The hydrolysis of phospholipids, mostly performed by pancreatic phospholipase A2, generates NEFAs and lysophospholipids. Cholesterol is present in the intestinal lumen as both non-esterified cholesterol and cholesteryl esters and originates from the diet and from the liver through the bile [5]. Only non-esterified cholesterol can be absorbed by the intestine. Cholesteryl esters are hydrolysed in the lumen of the intestine to non-esterified cholesterol and NEFAs. About 50% of the cholesterol in the intestine is absorbed and 50% is excreted in faeces [5].
Intestinal absorption of lipids
Intestinal absorption of NEFAs and 2-monoacylglycerol across the apical membrane of enterocytes is performed both by diffusion and by transporter-mediated uptake. Diffusion occurs when the NEFA concentration in the intestinal lumen exceeds that in the enterocytes, whereas transporter-mediated uptake is effective when the NEFA concentration is lower in the intestinal lumen than in the enterocytes [6]. The major proteins involved in this transporter-mediated absorption are fatty acid translocase (CD36/FAT), which is expressed at a very high level in the duodenum and jejunum, fatty acid transporter protein 4 (FATP4) and membrane-associated fatty acid-binding protein (FABPpm) [5, 6] (Fig. 1). The intestinal absorption of cholesterol is mainly performed via the Niemann–Pick C1-like 1 (NPC1L1) protein [7], which is inhibited by the hypocholesterolaemic drug ezetimibe. NPC1L1 is also involved in plant sterol (sitosterol, campesterol) absorption. Lysophospholipids are absorbed by passive diffusion [8] (Fig. 1).

Normal lipid absorption and intestinal lipoprotein metabolism. From left to right: hydrolysis of dietary TG to NEFAs and 2-MAG and of PL to lysoPL and NEFAs; absorption in the enterocyte of NEFAs and 2-MAG through specific transporters (CD36/FAT, FATP4, FABPpm) and of FC through NPC1L1 protein; transfer of lysoPL, NEFAs, 2-MAG and FC to the ER, followed by synthesis of PL from lysoPL, synthesis of TG from NEFAs and 2-MAG, and esterification of FC to form EC; in the ER, association of lipids (PL, TG, EC) with ApoB-48 by the action of MTP, leading to the formation of PC; transfer of PC to the Golgi in PCTVs, followed by the association of PC with apoA-I to form mature chylomicrons delivered in the lymph; in the circulation, hydrolysis of chylomicrons by LPL, leading to the formation of chylomicron remnants, which are taken up in the liver via the LDL-R and LRP. 2-MAG, 2-monoacylglycerol; EC, esterified cholesterol; FC, non-esterified cholesterol (also named free cholesterol); LDL-R, LDL receptor; lysoPL, lysophospholipids; PC, pre-chylomicron; PL, phospholipids; TG, triglycerides. This figure is available as part of a downloadable slideset
Lipid metabolism in enterocytes and chylomicron synthesis
In enterocytes, the absorbed non-esterified cholesterol, NEFAs, 2-monoacylglycerol and lysophospholipids are transported to the endoplasmic reticulum (ER). Non-esterified cholesterol is esterified in the ER by acyl-coA:cholesterol acyltransferase (ACAT). Non-esterified cholesterol that is not transferred to the ER for esterification is excluded from the cytosol back to the intestinal lumen by two transporters, ATP-binding cassette G5 (ABCG5) and ATP-binding cassette G8 (ABCG8), located in the brush border [9]. ABCG5 and ABCG8 are also responsible for transfer back to the lumen of plant sterols, preventing the detrimental accumulation of plant sterols in the body (Fig. 1).
The absorbed NEFAs and 2-monoacylglycerol are transferred to the ER by specific fatty acid-binding proteins (FABPs). In the ER, 2-monoacylglycerol is esterified with NEFAs by membrane-bound monoacylglycerol acyltransferases (MGATs), leading to the formation of diacylglycerol, which is then converted to triglycerides by the action of diacylglycerol acyltransferases (DGATs) [4]. Furthermore, in the ER, diacylglycerol is combined with choline by choline transferase and with ethanolamine by ethanolamine transferase to produce phospholipids.
In the ER, apolipoprotein (Apo) B-48, synthesised only in the intestine, is associated with triglycerides by the action of microsomal triglyceride transfer protein (MTP) and with cholesterol, phospholipids and ApoA-IV to form pre-chylomicrons. ApoB-48 that is not associated with lipids is rapidly degraded by the ubiquitin–proteasome system [6, 10]. Pre-chylomicrons synthesised in the ER are then transferred to the cis-Golgi in pre-chylomicron transport vesicles (PCTVs) [6, 11] (Fig. 1). In the Golgi, ApoA-I is associated with pre-chylomicrons to form mature chylomicrons, each containing a single molecule of ApoB-48 [12]. Chylomicrons are then released from the basolateral side of the enterocyte by exocytosis and move through the lamina propria before entering the lacteals through intercellular junctions [13]. From the lacteals, chylomicrons are delivered to the collecting lymphatic vessels. Contractile actions of smooth muscle fibres surrounding lymphatic vessels and one-way valves allow the active flow of lymph from the intestine to the left subclavian vein. In the circulation, chylomicron triglycerides are hydrolysed by lipoprotein lipase (LPL), leading to the formation of chylomicron remnants, which are taken up by the liver via the LDL receptor and the LDL receptor-related protein (LRP).
Lipids within the ER that are not used to produce chylomicron can be included in cytosolic droplets associated with different proteins, including perilipins. These cytosolic lipid droplets represent a transient pool of lipids that is used for chylomicron production during fasting [4].
Medium-chain fatty acids, containing 6–12 carbon atoms, do not pass through the chylomicron pathway but are directly absorbed into the portal circulation.
HDL production by the intestine
The enterocytes also produce HDL particles containing ApoA-I, phospholipids and non-esterified cholesterol via the ATP-binding cassette A1 (ABCA1) transporter located at the basolateral membrane of enterocytes [4]. It is estimated that, in humans, 13% of the total ApoA-I pool originates from the intestine [14].
The transintestinal cholesterol excretion process
The intestine is also responsible for the excretion of cholesterol into the intestinal lumen by a process called transintestinal cholesterol excretion (TICE) [15, 16]. The TICE process includes the following steps:
-
cholesterol uptake from VLDL and/or LDL by the basolateral membrane of enterocytes;
-
translocation of cholesterol from the basolateral membrane to the apical membrane of enterocytes by an unknown mechanism;
-
excretion of cholesterol into the intestinal lumen by the ABCG5/ABCG8 transporters.
Data from animal and human studies suggest that TICE could contribute to ~30% of faecal cholesterol excretion [15].
Role of insulin in intestinal lipid absorption and transport
Insulin significantly influences intestinal lipid metabolism not only directly but also indirectly by suppressing the release from adipose tissue of NEFAs, which are important components of intestinal lipoproteins.
Preclinical findings
In cultured jejunal explants from human fetuses, insulin reduces chylomicron production and ApoB-48 secretion [17]. Insulin negatively regulates expression of the gene encoding MTP and this inhibitory effect is partially mediated by the inhibition of forkhead box protein O1 (FoxO1) [18, 19]. In addition, data suggest that insulin promotes post-ER, presecretory proteolysis of ApoB-48 [20]. Moreover, insulin, by its inhibitory effect on hormone-sensitive lipase in adipose tissue, reduces plasma NEFA levels and, thus, their uptake by enterocytes, leading to a reduction in triglycerides available to be associated with ApoB-48. This reduced lipid availability may also favour ApoB-48 degradation in enterocytes (Fig. 2).

Effects of insulin and GLP-1 on lipid absorption and intestinal lipoprotein metabolism. Insulin (1) reduces plasma NEFAs by inhibiting adipose tissue hormone-sensitive lipase; (2) reduces MTP expression; (3) reduces ApoB-48 levels in the enterocyte; (4) increases LPL activity; and (5) increases expression of LDL-R and LRP. GLP-1 (a) reduces NEFA absorption; (b) reduces MTP expression; and (c) reduces ApoB-48 levels in the enterocyte. 2-MAG, 2-monoacylglycerol; EC, esterified cholesterol; FC, non-esterified cholesterol (also named free cholesterol); HS lipase, hormone-sensitive lipase; LDL-R, LDL receptor; lysoPL, lysophospholipids; PC, pre-chylomicron; PL, phospholipids; TG, triglycerides. This figure is available as part of a downloadable slideset
Clinical findings
Harbis et al reported a significant reduction in plasma ApoB-48 during a euglycaemic–hyperinsulinaemic clamp compared with the absence of insulin infusion in healthy individuals after a lipid-rich meal [21]. In healthy men, Pavlic et al observed a decrease in the production of ApoB-48-containing lipoproteins by 50–52% on insulin (+glucose) infusion compared with saline infusion, and by 16–21% when the insulin-induced lowering of NEFAs was prevented by concomitant Intralipid infusion [22]. These data suggest that insulin reduces the production of intestinal lipoproteins in part by decreasing plasma NEFA levels, but also by a direct effect.
In addition, insulin accelerates chylomicron and chylomicron remnant catabolism by increasing LPL activity and the expression of the LDL receptor and LRP [1] (Fig. 2).
Role of the intestinal hormones GLP-1, GLP-2 and GIP in intestinal lipid absorption and transport
Glucagon-like peptide-1
GLP-1, secreted by intestinal L cells in response to meals, influences intestinal lipid metabolism.
Preclinical findings
In rats, GLP-1 reduces intestinal lipoprotein production [23]. GLP-1 receptor knockout mice show increased levels of triglyceride-rich ApoB-48-containing lipoproteins after an oral fat load, confirming the role of GLP-1 in the reduction of postprandial lipids [24]. A study showing enhanced triglyceride output in mesenteric lymph in rats in response to an intraduodenal lipid bolus after injection of the GLP-1 receptor antagonist exendin 9-39 strongly suggests a physiological inhibitory effect of GLP-1 on chylomicron production [25].
Clinical findings
Acute infusion of native GLP-1 in healthy volunteers reduces postprandial triglyceride and NEFA levels following a test meal [26].
GLP-1 is likely to directly reduce postprandial hyperlipidaemia by different means. GLP-1 or the GLP-1 receptor agonist exendin-4 have been shown in animal studies to decrease intestinal NEFA absorption by reducing the expression of CD36, which is responsible for NEFA absorption [23, 27, 28]. The precise effect of GLP-1 on intestinal lipid absorption has not been studied in humans, but the dramatic decrease in post-meal plasma triglyceride and NEFA levels after injection of GLP-1 in healthy individuals suggests that GLP-1 is also likely to reduce lipid absorption in humans [26] (Fig. 2). In vitro, exendin-4 reduces the secretion of ApoB-48 from enterocytes [24]. Exendin-4 also reduces the jejunal activity of MTP in Syrian hamsters [27] (Fig. 2).
GLP-1 receptors (GLP-1Rs) are present in the central nervous system and some data indicate that GLP-1 may influence lipid metabolism through central GLP-1R activation. In mice, central GLP-1R activation by exendin-4 increases the plasma clearance of triglycerides through increased uptake of triglyceride-derived NEFAs, mostly by brown adipose tissue, accompanied by activation of brown adipose tissue and browning of white adipose tissue, via the sympathetic nervous system [29]. However, the data on the potential effect of GLP-1R activation in the central nervous system on intestinal lipid metabolism are inconsistent. Farr et al have shown that, in Syrian hamsters, there is a significant reduction in levels of postprandial triglycerides and triglyceride-rich ApoB-48-containing lipoproteins after a single intracerebroventricular injection of exendin-4, which is abolished after peripheral adrenergic receptor and central melanocortin-4 receptor inhibition [27]. However, the reduction in postprandial lipids by GLP-1 analogues was preserved in mice with specific deletion of the GLP-1R in the central nervous system, suggesting that intestinal lipid metabolism is not likely to be significantly influenced by GLP-1R activation in the brain [30].
Glucagon-like peptide-2
GLP-2, secreted by intestinal L cells in response to fat and carbohydrate intake, also plays a role in intestinal lipid metabolism.
Preclinical findings
In Syrian hamsters, GLP-2 increases intestinal lipid absorption by upregulating the expression of the NEFA transporter CD36, and enhances the production of chylomicrons [31]. GLP-2 also increases ApoB-48 synthesis in jejunal cells and intestinal MTP activity in Syrian hamsters [32].
Clinical findings
GLP-2 increases postprandial lipaemia in humans [26]. Some data suggest that the effects of GLP-2 on postprandial lipids may be mediated by an increase in nitric oxide (NO), a known mediator of GLP-2, augmenting mesenteric blood flow [32]. GLP-2 treatment significantly increases postprandial lipid accumulation and circulating ApoB-48 protein levels in wild-type mice, while these effects are abolished in neuronal NO synthase knockout mice [33]. However, administration of an NO synthase inhibitor in combination with GLP-2 in humans did not modify the increase in chylomicron secretion observed with GLP-2 alone, suggesting that NO production is not a major factor responsible for the effects of GLP-2 on intestinal lipid metabolism [34].
Thus, GLP-1 and GLP-2 have opposite effects on intestinal lipoprotein production. It has been shown that, under physiological conditions, the effects of GLP-2 predominate, but when GLP-1 activity is sustained the effects of GLP-1 prevail [35]. However, the global action of both GLP-1 and GLP-2 on intestinal lipid transport remains unclear and requires further elucidation.
Gastric inhibitory peptide
GIP, secreted by duodenal and jejunal K cells in response to nutrient intake, may also influence postprandial lipid metabolism.
Preclinical findings
After an oral fat load GIP lowers plasma triglyceride levels in rats and reduces levels of chylomicron triglycerides in lymph in dogs [36, 37]. GIP enhances LPL activity in cultured pre-adipocytes and in rat epididymal adipose tissue and increases LPL gene expression in human adipocytes in the presence of insulin [38, 39].
Clinical findings
To date there is no clear evidence of an effect of GIP on LPL in humans. In a study performed in lean and obese women, GIP had no effect on LPL activity [40]. In lean, non-diabetic and diabetic men with obesity, GIP infusion did not modify LPL gene expression in subcutaneous adipose tissue [40, 41].
Disorders of intestinal lipid absorption and transport in type 2 diabetes
Patients with type 2 diabetes show postprandial hyperlipidaemia
Postprandial hyperlipidaemia is observed in individuals with type 2 diabetes, as in those with the metabolic syndrome [1, 2, 42, 43]. In a study by Lim et al, individuals with type 2 diabetes showed increased triglyceride and ApoB-48 AUCs and incremental AUCs after a high-fat meal [2]. In this study, both abdominal visceral obesity and low HDL-cholesterol concentrations were independently associated with increased post-load excursions of triglycerides, and the triglyceride AUC was an independent factor associated with subclinical atherosclerosis (intima–media thickness, ankle–brachial index) [2].
Increased chylomicron production in type 2 diabetes
Preclinical findings
Fructose-fed hamsters, a model of insulin resistance, are characterised by overproduction of ApoB-48-containing lipoproteins [44]. A marked increase in the production of chylomicrons has been reported in Zucker rats and in Psammomys obesus gerbils, a model of insulin resistance and type 2 diabetes [45,46,47]. Increased de novo lipogenesis has been demonstrated in duodenal cells from insulin-resistant individuals with obesity in parallel with defects in insulin signalling [48].
Clinical findings
A lipoprotein kinetic study has demonstrated that, in the postprandial state, there is a twofold increase in ApoB-48 production in non-diabetic insulin-resistant individuals with obesity [49]. In this study, the ApoB-48 production rate was positively correlated with plasma insulin levels, suggesting that insulin resistance is likely to be involved [49]. In an in vivo kinetic study performed in the fed state, a significant increase in the ApoB-48 pool (×4.6) was reported in individuals with type 2 diabetes compared with control participants, which was mostly related to a marked increase in the ApoB-48 production rate (×3.6) [50].
Mechanisms of increased chylomicron production
Insulin resistance appears to be an important factor in the increase in chylomicron production in type 2 diabetes. Insulin has been shown to inhibit ApoB-48 lipoprotein production in chow-fed hamsters but not in insulin-resistant fructose-fed hamsters [51]. Using hyperperinsulinaemic–euglycaemic clamps, Nogueira et al demonstrated that the inhibitory effect of insulin on intestinal ApoB-48 lipoprotein production is abolished in individuals with type 2 diabetes [52]. Different mechanisms are likely to be involved in the increase in chylomicron production observed in type 2 diabetes.
Increased expression and activity of intestinal MTP
-
Preclinical findings: Several studies have shown increased expression and activity of intestinal MTP in animal models of insulin resistance and type 2 diabetes, associated with oversecretion of chylomicrons [45, 53, 54].
-
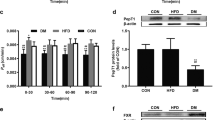
Clinical findings: Veilleux et al reported increased protein levels of MTP in small intestine sections from diabetic patients with obesity undergoing bariatric surgery [48]. Phillips et al showed significantly higher levels of mRNA encoding MTP in the duodenum of individuals with type 2 diabetes than non-diabetic individuals, which was positively correlated with chylomicron lipid enrichment [54]. In individuals with type 2 diabetes and obesity, alteration of intestinal intracellular insulin signalling has been observed in parallel with increased expression of MTP, suggesting that the inhibitory effect of insulin on the gene encoding MTP is abolished in this situation of insulin resistance [48] (Fig. 3).

Disorders of intestinal lipid metabolism in type 2 diabetes. (1) Increased expression and activity of intestinal MTP; (2) increased stability and availability of ApoB-48; (3) possible increased de novo lipogenesis (increased expression of MGAT and DGAT); (4) increased activity of hormone-sensitive lipase because of insulin resistance, leading to increased plasma NEFA levels available for intestinal lipogenesis; (5) increased chylomicron production by the enterocyte secondary to (1), (2), (3) and (4); and (6) reduced LPL activity because of insulin resistance, leading to reduced chylomicron catabolism. 2-MAG, 2-monoacylglycerol; EC, esterified cholesterol; FC, non-esterified cholesterol (also named free cholesterol); HS lipase, hormone-sensitive lipase; lysoPL, lysophospholipids; PC, pre-chylomicron; PL, phospholipids; TG, triglycerides. This figure is available as part of a downloadable slideset
Increased stability and availability of ApoB-48
Increased availability and stability of ApoB-48 are also observed in insulin resistance and type 2 diabetes. Cultured enterocytes from insulin-resistant fructose-fed hamsters synthesise and secrete more ApoB-48 than control chow-fed hamsters, with 90 min pulse–chase labelling experiments showing greater persistence of newly synthesised ApoB-48 in fructose-fed hamsters (30% vs 15%) and a smaller reduction in ApoB-48 levels during the chase (7% vs 30%), indicating enhanced ApoB-48 stability in enterocytes from insulin-resistant animals [44] (Fig. 3). Increased secretion of ApoB-48 is observed in jejunal explants from Psammomys obesus gerbils, a model of insulin resistance [47]. This is abolished in the presence of proteasomal inhibitors in the culture medium, suggesting that the increase in ApoB-48 in enterocytes is due to reduced proteasomal degradation activity [47].
It has also been suggested that, in insulin resistance and type 2 diabetes, the higher concentration of lipids available in enterocytes stabilises ApoB-48 and prevents its proteolytic degradation via the ubiquitin-dependent proteasomal pathway [6, 10].
Increased de novo lipogenesis
Several data indicate that there is an increase in de novo lipogenesis in enterocytes in type 2 diabetes.
-
Preclinical findings: The intracellular levels of non-esterified cholesterol, esterified cholesterol and triglycerides are significantly increased in enterocytes isolated from insulin-resistant fructose-fed hamsters, suggesting increased lipogenesis [44]. Increased activity of MGAT and DGAT, two key enzymes involved in triglyceride synthesis, and increased expression of FABP, responsible for the transfer of absorbed fatty acids to the ER, have been observed in jejunal explants from Psammomys obesus gerbils with insulin resistance with or without diabetes, with a parallel increase in triglyceride production [47]. Increased expression of MGAT, DGAT and the mature form of sterol regulatory element-binding protein 1c (SREBP-1c), a transcription factor promoting lipogenesis, has also been observed in intestinal cells in animal models of diabetes [51, 55] (Fig. 3).
-
Clinical findings: Some human studies have found increased expression of SREBP-1c, ApoA-IV and FABP in the intestines of insulin-resistant individuals with obesity [48, 56] (Fig. 3). However, a study performed in young non-diabetic men with insulin resistance did not find any increase in the expression of SREBP-1c, FABP, DGAT or MGAT in the duodenum [57]. It has been suggested that the discrepancies between studies might be due to the different levels of insulin resistance in the populations studied, with increased expression of factors and enzymes involved in lipogenesis seen only in more severe insulin resistance or relative insulin deficiency [57].
Increased NEFA plasma levels
Insulin resistance is also characterised by enhanced plasma levels of NEFAs, which may serve as substrates for lipid synthesis in enterocytes (Fig. 3). In individuals who are morbidly obese with and without diabetes, increased fatty acid uptake from the circulation into the jejunum has been demonstrated without any modification of intestinal blood flow [58]. This indicates that higher fatty acid availability in insulin-resistant states may also be involved in the overproduction of chylomicrons.
Thus, increased production of chylomicrons by the intestine is an important feature not only in individuals with type 2 diabetes but also in non-diabetic insulin-resistant individuals, indicating that insulin resistance is likely to be the main factor involved in its pathophysiology. However, data suggest that, in type 2 diabetes, hyperglycaemia itself may amplify chylomicron overproduction. In healthy men, duodenal co-infusion of glucose with Intralipid or fructose with Intralipid induces a significant increase in ApoB-48 production [59]. Furthermore, hyperglycaemia caused by glucose infusion in healthy men leads to an increase in the production of ApoB-48-containing lipoproteins [60]. Therefore, hyperglycaemia may also contribute to the chylomicron overproduction observed in type 2 diabetes, but its precise involvement, if any, remains to be clarified.
Delayed chylomicron catabolism in type 2 diabetes
Delayed chylomicron catabolism is also likely to be involved in diabetic postprandial hyperlipidaemia. Duez et al did not observe delayed catabolism of ApoB-48 in non-diabetic insulin-resistant men with obesity [49]; however, several other studies in similar populations have reported data indicating the presence of reductions in chylomicron catabolism [61,62,63]. Several kinetic studies have reported reduced fractional catabolic rates of ApoB-48 in insulin-resistant individuals with obesity and individuals with type 2 diabetes [50, 62, 63]. This may be related to the reduction in LPL activity observed in type 2 diabetes [1]. Because insulin activates LPL, reduced LPL activity may be due to a ‘relative’ insulin deficiency and/or insulin resistance in type 2 diabetes (Fig. 3). Furthermore, individuals with type 2 diabetes and non-diabetic insulin-resistant individuals show increased plasma levels of ApoC-III, an inhibitor of LPL, which may also contribute to delayed chylomicron catabolism [64].
Modification of cholesterol absorption in type 2 diabetes
In vitro, high glucose levels increase NPC1L1 expression in enterocytes [65]. Increased levels of NPC1L1 mRNA and decreased levels of ABCG5 and ABCG8 mRNA have also been found in the duodenum of individuals with type 2 diabetes [66]. These data suggest the presence of increased cholesterol absorption in type 2 diabetes. However, reduced plasma levels of campesterol, a marker of cholesterol absorption, have been reported in individuals with the metabolic syndrome and those with type 2 diabetes, in parallel with increased plasma levels of lathosterol, a marker of cholesterol biosynthesis, suggesting reduced cholesterol absorption and increased cholesterol synthesis in these individuals [67, 68]. Kinetic studies using stable isotopes have demonstrated reduced cholesterol absorption and increased cholesterol synthesis in individuals with type 2 diabetes [69, 70]. Because several data indicate the presence of increased expression of SREBP-1c, which is involved in cholesterol biosynthesis, an increase in cholesterol synthesis may be the initial step leading to reduced intestinal cholesterol absorption, as a compensatory mechanism.
Potential influence of microbiota
Many studies have shown that type 2 diabetes is associated with significant modification of gut microbiota, with fewer bacteria producing butyrate, an important small-chain fatty acid (SCFA), and more bacteria producing lipopolysaccharides (LPS) [71].
Increased production of LPS by some Gram-negative bacteria is observed in type 2 diabetes [72]. LPS have been shown to have proinflammatory effects and to activate intestinal mucosal mast cells, leading to increased intestinal permeability and fat absorption in mice [73, 74].
Several data, mostly from animal studies, suggest that the modification of microbiota in type 2 diabetes may modify intestinal lipid metabolism.
Preclinical findings
Dysbiosis of the gut microbiota in mice is associated with increased expression of genes encoding for enzymes involved in lipogenesis and chylomicron production (DGAT, acetyl-coA carboxylase [ACC], fatty acid synthase [FAS] and MTP) [75]. Improvement of gut microbiota in hamsters fed a high-fat diet supplemented with soybean-derived sterols induces significant reductions in plasma triglyceride, total cholesterol and non-HDL-cholesterol levels, increased intestinal production of SCFAs, increased faecal excretion of sterols and increased expression of NPC1L1 and ABCG5/ABCG8, suggesting that improvement of gut microbiota induces modifications of lipid metabolism, including a potential reduction in total cholesterol absorption [76].
Clinical findings
Some human studies have reported a possible link between gut microbiota and fasting plasma lipids in individuals with obesity, such as higher triglyceride levels in those with a low bacterial gene count, indicative of dysbiosis of the gut microbiota [77, 78]; however, limited data are available on postprandial lipids. In a study of individuals with the metabolic syndrome, a diet and lifestyle intervention followed for 14 days induced significant modifications of gut microbiota, in parallel with significant reductions in plasma triglyceride levels and chylomicrons [79]. However, it is difficult to conclude from this study that the reduction in chylomicrons was directly related to modification of gut microbiota.
Although human data are still lacking, dysbiosis of gut microbiota in type 2 diabetes may influence intestinal lipid metabolism by different mechanisms:
-
Increased production of LPS may increase intestinal permeability and lipid absorption and, through low-grade inflammation, promote intestinal insulin resistance, which may increase chylomicron production.
-
Reduced production of SCFAs, which have anti-inflammatory effects and stimulate GLP-1 production, may be responsible for reduced GLP-1 secretion, which may lead to increased lipid absorption and chylomicron production [80].
-
The gut microbiota can transform primary bile acids into secondary bile acids, which increase GLP-1 production [81]. In dysbiosis of gut microbiota, the transformation of primary bile acids into secondary bile acids is reduced, which may decrease GLP-1 production, with direct consequences for intestinal lipid metabolism.
The transintestinal cholesterol excretion process
Little information is available on TICE in insulin-resistant states or diabetes. A 45% increase in macrophage-derived cholesterol faecal excretion has been observed in insulin-resistant hamsters, suggesting possible upregulation of TICE [82]. However, further studies are needed to clarify whether TICE is modified in individuals with type 2 diabetes.
Effects of glucose-lowering treatments on intestinal lipid absorption and transport
As well as reducing hyperglycaemia, some glucose-lowering drugs also modify intestinal lipid metabolism.
Metformin
Several studies have shown that metformin treatment influences postprandial lipid metabolism. Jeppesen et al reported a significant reduction in postprandial triglyceride levels in individuals with type 2 diabetes after 10 weeks’ treatment with metformin (2.55 g/day), with 32% and 26% reductions in chylomicrons and chylomicron remnants, respectively [83]. Gutierrez-Repiso et al showed that the increased expression of SREBP-1c and ApoA-IV (apolipoprotein bound with chylomicrons) in the jejunal cells of insulin-resistant individuals with obesity was abolished by metformin treatment, indicating that metformin may have a direct effect on the expression of genes involved in intestinal lipid metabolism [56]. The effect of metformin on intestinal lipid metabolism may also be indirect through delayed gastric emptying [84] and increased GLP-1 secretion [85].
Sulfonylureas and glinides
Sulfonylureas and glinides appear to have a limited effect or no effect on intestinal lipid metabolism. Glipizide has been shown to reduce postprandial hyperlipidaemia in very badly controlled patients with type 2 diabetes (mean HbA1c 120 mmol/mol [13.1%]) [86]; however, nateglinide and glibenclamide did not have any effect on postprandial triglyceride levels in ‘more usual’ type 2 diabetes patients (mean HbA1c 60 mmol/mol [7.6%]) [87].
Glitazones (thiazolidinediones)
In non-diabetic overweight individuals, pioglitazone (45 mg/day) induced a significant 22% reduction in the postprandial triglyceride AUC [88]. In a double-blind controlled study performed in 22 individuals with type 2 diabetes, pioglitazone (45 mg/day) reduced the postprandial triglyceride AUC by 33% and the postprandial ApoB-48 AUC by 58% compared with glibenclamide (5 mg/day) [89]. The mechanisms responsible for improved postprandial lipidaemia with pioglitazone treatment remain unclear but it has been suggested that increased insulin sensitivity plays a major role [89]. In contrast, rosiglitazone appears to have a weaker effect or no effect, or sometimes a detrimental effect, on postprandial lipid metabolism. In individuals with type 2 diabetes, rosiglitazone has been reported to result in a significant reduction in the incremental postprandial triglyceride AUC but not the total postprandial triglyceride AUC in one study [90] but in an increase in the postprandial triglyceride AUC and ApoB-48 AUC in two other studies [91, 92].
Alpha-glucosidase inhibitors
The alpha-glucosidase inhibitor acarbose reduces postprandial triglyceride levels. Hanefeld et al reported a significant 20% reduction in 1 h postprandial triglyceride levels in type 2 diabetes patients after 24 weeks’ treatment with acarbose (300 mg/day) [93]. Ogawa et al reported a significant reduction in postprandial triglyceride levels and chylomicrons after a single dose of acarbose (100 mg) or after 8 weeks’ treatment with acarbose (300 mg/day) in both normotriglyceridaemic and hypertriglyceridaemic type 2 diabetes patients [94]. The mechanisms involved in the postprandial hypotriglyceridaemic effect of acarbose remain unprecise. In vitro, acarbose reduces ApoB-48 secretion, suggesting that it may reduce chylomicron synthesis [95]. In addition, acarbose significantly reduces postprandial NEFA levels in type 2 diabetes patients [94], which may reduce intestinal lipogenesis.
Dipeptidyl peptidase 4 inhibitors
Dipeptidyl peptidase 4 (DPP-4) inhibitors reduce postprandial lipid levels.
Preclinical findings
In mice, systemic inhibition of DPP-4 activity with sitagliptin reduces triglyceride excursions during a lipid tolerance test, with a parallel increase in plasma GLP-1 levels [96].
Clinical findings
In a double-blind crossover study performed in patients with type 2 diabetes, 6 weeks’ treatment with sitagliptin (100 mg/day) significantly reduced the postprandial AUCs for triglycerides, ApoB-48 and NEFAs in parallel with a significant increase in postprandial GLP-1 and GIP levels [97]. Compared with placebo, vildagliptin (50 mg twice daily) administered for 4 weeks in patients with type 2 diabetes induced a significant reduction in the postprandial AUCs for total triglycerides, chylomicron triglycerides and chylomicron ApoB-48 as well as a significant increase in postprandial GLP-1 [98]. Treatment with alogliptin (25 mg/day) for 16 weeks induced a significant reduction in postprandial total triglyceride levels, chylomicron triglycerides and chylomicron ApoB-48 in patients with type 2 diabetes [99]. Xiao et al performed a lipoprotein kinetic study of healthy men in a constant fed state, combined with a pancreatic clamp with somatostatin to prevent the effects of incretins on insulin and glucagon secretion, and found a significant reduction in the production of triglyceride-rich ApoB-48-containing lipoproteins after one dose of sitagliptin [100].
As suggested by animal and human studies, the postprandial hypolipidaemic effect of DPP-4 inhibitors is likely to be related to the increase in plasma GLP-1 levels (see below). It has also been suggested that the decrease in postprandial plasma glucagon levels (and the increase in the postprandial insulin/glucagon ratio) may also lead to a reduction in postprandial NEFA levels, which may reduce intestinal lipogenesis [97].
GLP-1 agonists
Treatment with GLP-1 agonists significantly influences intestinal lipid metabolism.
Preclinical findings
Significant reductions in ApoB-48 secretion and intestinal MTP activity after treatment with the GLP-1 agonist exendin-4 have been reported in vitro [24]. In vitro, liraglutide reduces the expression of genes encoding for enzymes involved in chylomicron production: ApoB-48, DGAT1 and MTP [101]. Furthermore, LPL activity in adipose tissue is significantly increased in mice after short-term treatment with liraglutide [101].
Clinical findings
A significant reduction in the AUCs of triglycerides and ApoB-48 after a standardised fat-rich meal has been reported in type 2 diabetes patients after treatment with liraglutide (1.8 mg/day), independently of gastric emptying and NEFA plasma levels [102]. In a randomised study performed in 20 patients with type 2 diabetes, a significant reduction in postprandial triglycerides was observed after 2 weeks’ treatment with exenatide (5 μg twice a day in the first week, 10 μg twice a day in the second week) or liraglutide (0.6 mg/day in the first week and 1.2 mg/day in the second week) [103]. In a randomised, double-blind crossover trial performed in type 2 diabetes patients, 12 weeks’ treatment with oral semaglutide (up to 14 mg/day) induced significant reductions in the AUCs of postprandial triglycerides, ApoB-48 and VLDL compared with placebo [104]. Thus, all the data indicate that treatment with GLP-1 agonists significantly reduces postprandial lipid levels.
Several studies have demonstrated an impact of GLP-1 agonists on postprandial lipid metabolism and reported data suggesting direct effects. In an in vivo lipoprotein kinetic study performed in healthy men receiving infusions of a high-fat, mixed macronutrient liquid formula in the duodenum, Xiao et al showed that a single injection of exenatide (10 μg) significantly reduced the production rate of triglyceride-rich ApoB-48-containing lipoproteins [105]. A lipoprotein kinetic study performed in patients with type 2 diabetes during constant feeding with micro-meals showed that after 6 months’ treatment with liraglutide (1.2 mg/day) there was a significant reduction in ApoB-48 production (−50%) and an increase in ApoB-48 catabolism (+39%) [101]. Taskinen et al reported that 16 weeks’ treatment with liraglutide at a higher dose of 1.8 mg/day reduced by 60% the production rate of chylomicron ApoB-48 after a fat-rich mixed meal, independently of the observed improvement in insulin sensitivity [106]. Whyte et al found that 4 weeks’ treatment with lixisenatide in patients with type 2 diabetes significantly increased the clearance of chylomicron triglycerides, leading to a reduction in pool size [107].
Sodium–glucose cotransporter 2 inhibitors
Data on the effect of sodium–glucose cotransporter 2 inhibitors on postprandial lipid metabolism are scarce. Six months’ treatment with empagliflozin (10 mg/day) significantly reduced 1 h and 2 h postprandial triglyceride levels and remnant-like particle cholesterol levels in patients with type 2 diabetes [108]. In a Japanese multicentre study, no modification of chylomicron cholesterol levels was observed after 3 months’ treatment with canagliflozin (100 mg/day) [109]. However, in that study, chylomicron cholesterol was not measured after a meal (or a fat load test), which does not exclude an effect of canagliflozin on postprandial lipids.
The remaining questions and perspectives for the future
This review provides an overview of the modification of intestinal lipid metabolism in type 2 diabetes and the known intestinal effects of glucose-lowering treatments. However, several questions remained unanswered.
As a direct effect of insulin resistance per se is very likely to be involved in the postprandial dyslipidaemia observed in type 2 diabetes, it will be important to study whether factors associated with insulin resistance, such as modified plasma levels of adipokines (e.g. retinol-binding protein 4 and adiponectin), also play a direct role. Studies are also needed to determine how modification of gut microbiota in type 2 diabetes may influence intestinal lipid metabolism. More information is needed on the potential role of glucagon in intestinal lipid metabolism in patients with type 2 diabetes. In healthy individuals, acute administration of glucagon does not modify plasma triglyceride levels or the production of ApoB-48-containing lipoproteins [110, 111]. However, the potential role of chronic hyperglucagonaemia in postprandial lipid metabolism needs to be clarified in patients with type 2 diabetes. This point is important, as new glucose-lowering agents with glucagon agonist activity are in development.
Furthermore, multireceptor agonists for the treatment of type 2 diabetes are being developed. It will be important to study the effects of the GLP-1/glucagon and GLP-1/GIP dual agonists and the GLP-1/glucagon/GIP triagonist on intestinal lipid metabolism.
Abbreviations
- ABCA1:
-
ATP-binding cassette A1
- ABCG5:
-
ATP-binding cassette G5
- ABCG8:
-
ATP-binding cassette G8
- ACAT:
-
acyl-coA:cholesterol acyltransferase
- Apo:
-
Apolipoprotein
- CD36/FAT:
-
Fatty acid translocase
- DGAT:
-
Diacylglycerol acyltransferase
- DPP-4:
-
Dipeptidyl peptidase 4
- ER:
-
Endoplasmic reticulum
- FABP:
-
Fatty acid-binding protein
- FABPpm:
-
Membrane-associated fatty acid-binding protein
- FATP4:
-
Fatty acid transporter protein 4
- GIP:
-
Gastric inhibitory polypeptide
- GLP-1:
-
Glucagon-like peptide-1
- GLP-1R:
-
Glucagon-like peptide-1 receptor
- GLP-2:
-
Glucagon-like peptide-2
- LPL:
-
Lipoprotein lipase
- LPS:
-
Lipopolysaccharides
- LRP:
-
LDL receptor-related protein
- MGAT:
-
Monoacylglycerol acyltransferase
- MTP:
-
Microsomal triglyceride transfer protein
- NEFA:
-
Non-esterified fatty acid
- NO:
-
Nitric oxide
- NPC1L1:
-
Niemann–Pick C1-like 1
- PCTV:
-
Pre-chylomicron transport vesicle
- SCFA:
-
Small-chain fatty acid
- SREBP-1c:
-
Sterol regulatory element-binding protein 1c
- TICE:
-
Transintestinal cholesterol excretion
References
Vergès B (2015) Pathophysiology of diabetic dyslipidaemia: where are we? Diabetologia. 58(5):886–899. https://doi.org/10.1007/s00125-015-3525-8
Lim S, Kim YJ, Khang AR, Eckel RH (2021) Postprandial dyslipidemia after a standardized high-fat meal in BMI-matched healthy individuals, and in subjects with prediabetes or type 2 diabetes. Clin Nutr 40(11):5538–5546. https://doi.org/10.1016/j.clnu.2021.09.004
Chait A, Ginsberg HN, Vaisar T, Heinecke JW, Goldberg IJ, Bornfeldt KE (2020) Remnants of the Triglyceride-Rich Lipoproteins, Diabetes, and Cardiovascular Disease. Diabetes. 69(4):508–516. https://doi.org/10.2337/dbi19-0007
Hussain MM (2014) Intestinal lipid absorption and lipoprotein formation. Curr Opin Lipidol 25(3):200–206. https://doi.org/10.1097/MOL.0000000000000084
Iqbal J, Hussain MM (2009) Intestinal lipid absorption. Am J Physiol Endocrinol Metab 296(6):E1183–E1194. https://doi.org/10.1152/ajpendo.90899.2008
Mansbach CM, Gorelick F (2007) Development and physiological regulation of intestinal lipid absorption. II. Dietary lipid absorption, complex lipid synthesis, and the intracellular packaging and secretion of chylomicrons. Am J Physiol Gastrointest Liver Physiol 293(4):G645–G650. https://doi.org/10.1152/ajpgi.00299.2007
Wang LJ, Song BL (2012) Niemann-Pick C1-Like 1 and cholesterol uptake. Biochim Biophys Acta 1821(7):964–972. https://doi.org/10.1016/j.bbalip.2012.03.004
Stahl A, Gimeno RE, Tartaglia LA, Lodish HF (2001) Fatty acid transport proteins: a current view of a growing family. Trends Endocrinol Metab 12(6):266–273. https://doi.org/10.1016/S1043-2760(01)00427-1
Wang J, Mitsche MA, Lütjohann D, Cohen JC, Xie XS, Hobbs HH (2015) Relative roles of ABCG5/ABCG8 in liver and intestine. J Lipid Res 56(2):319–330. https://doi.org/10.1194/jlr.M054544
Black DD (2007) Development and physiological regulation of intestinal lipid absorption. I. Development of intestinal lipid absorption: cellular events in chylomicron assembly and secretion. Am J Physiol Gastrointest Liver Physiol 293(3):G519–G524. https://doi.org/10.1152/ajpgi.00189.2007
Kumar NS, Mansbach CM (1999) Prechylomicron transport vesicle: isolation and partial characterization. Am J Phys 276(2):G378–G386. https://doi.org/10.1152/ajpgi.1999.276.2.G378
Giammanco A, Cefalù AB, Noto D, Averna MR (2015) The pathophysiology of intestinal lipoprotein production. Front Physiol 6:61. https://doi.org/10.3389/fphys.2015.00061
Xiao C, Stahel P, Nahmias A, Lewis GF (2020) Emerging role of lymphatics in the regulation of intestinal lipid mobilization. Front Physiol 10:1604. https://doi.org/10.3389/fphys.2019.01604
Chétiveaux M, Croyal M, Ouguerram K et al (2020) Effect of fasting and feeding on apolipoprotein A-I kinetics in preβ1-HDL, α-HDL, and triglyceride-rich lipoproteins. Sci Rep 10(1):15585. https://doi.org/10.1038/s41598-020-72323-w
Jakulj L, van Dijk TH, de Boer JF et al (2016) Transintestinal Cholesterol Transport Is Active in Mice and Humans and Controls Ezetimibe-Induced Fecal Neutral Sterol Excretion. Cell Metab 24(6):783–794. https://doi.org/10.1016/j.cmet.2016.10.001
Grefhorst A, Verkade HJ, Groen AK (2019) The TICE Pathway: Mechanisms and Lipid-Lowering Therapies. Methodist Debakey Cardiovasc J 15(1):70–76. https://doi.org/10.14797/mdcj-15-1-70
Levy E, Sinnett D, Thibault L, Nguyen TD, Delvin E, Ménard D (1996) Insulin modulation of newly synthesized apolipoproteins B-100 and B-48 in human fetal intestine: gene expression and mRNA editing are not involved. FEBS Lett 393(2–3):253–258. https://doi.org/10.1016/0014-5793(96)00896-4
Vergès B (2010) Abnormal hepatic apolipoprotein B metabolism in type 2 diabetes. Atherosclerosis. 211(2):353–360. https://doi.org/10.1016/j.atherosclerosis.2010.01.028
Lin MC, Gordon D, Wetterau JR (1995) Microsomal triglyceride transfer protein (MTP) regulation in HepG2 cells: insulin negatively regulates MTP gene expression. J Lipid Res 36(5):1073–1081. https://doi.org/10.1016/S0022-2275(20)39865-5
Ginsberg HN, Fisher EA (2009) The ever-expanding role of degradation in the regulation of apolipoprotein B metabolism. J Lipid Res 50(Suppl):S162–S166. https://doi.org/10.1194/jlr.R800090-JLR200
Harbis A, Defoort C, Narbonne H et al (2001) Acute hyperinsulinism modulates plasma apolipoprotein B-48 triglyceride-rich lipoproteins in healthy subjects during the postprandial period. Diabetes. 50(2):462–469. https://doi.org/10.2337/diabetes.50.2.462
Pavlic M, Xiao C, Szeto L, Patterson BW, Lewis GF (2010) Insulin acutely inhibits intestinal lipoprotein secretion in humans in part by suppressing plasma free fatty acids. Diabetes. 59(3):580–587. https://doi.org/10.2337/db09-1297
Qin X, Shen H, Liu M et al (2005) GLP-1 reduces intestinal lymph flow, triglyceride absorption, and apolipoprotein production in rats. Am J Physiol Gastrointest Liver Physiol 288(5):G943–G949. https://doi.org/10.1152/ajpgi.00303.2004
Hsieh J, Longuet C, Baker CL et al (2010) The glucagon-like peptide 1 receptor is essential for postprandial lipoprotein synthesis and secretion in hamsters and mice. Diabetologia. 53(3):552–561. https://doi.org/10.1007/s00125-009-1611-5
Nahmias A, Stahel P, Tian L, Xiao C, Lewis GF (2021) GLP-1 (Glucagon-Like Peptide-1) Is Physiologically Relevant for Chylomicron Secretion Beyond Its Known Pharmacological Role. Arterioscler Thromb Vasc Biol 41(6):1893–1900. https://doi.org/10.1161/ATVBAHA.121.316311
Meier JJ, Gethmann A, Götze O et al (2006) Glucagon-like peptide 1 abolishes the postprandial rise in triglyceride concentrations and lowers levels of non-esterified fatty acids in humans. Diabetologia. 49(3):452–458. https://doi.org/10.1007/s00125-005-0126-y
Farr S, Baker C, Naples M et al (2015) Central Nervous System Regulation of Intestinal Lipoprotein Metabolism by Glucagon-Like Peptide-1 via a Brain-Gut Axis. Arterioscler Thromb Vasc Biol 35(5):1092–1100. https://doi.org/10.1161/ATVBAHA.114.304873
Dai Y, Dai D, Wang X, Ding Z, Li C, Mehta JL (2014) GLP-1 agonists inhibit ox-LDL uptake in macrophages by activating protein kinase A. J Cardiovasc Pharmacol 64(1):47–52. https://doi.org/10.1097/FJC.0000000000000087
Kooijman S, Wang Y, Parlevliet ET et al (2015) Central GLP-1 receptor signalling accelerates plasma clearance of triacylglycerol and glucose by activating brown adipose tissue in mice. Diabetologia. 58(11):2637–2646. https://doi.org/10.1007/s00125-015-3727-0
Varin EM, Mulvihill EE, Baggio LL et al (2019) Distinct Neural Sites of GLP-1R Expression Mediate Physiological versus Pharmacological Control of Incretin Action. Cell Rep 27(11):3371–3384.e3. https://doi.org/10.1016/j.celrep.2019.05.055
Hsieh J, Longuet C, Maida A et al (2009) Glucagon-like peptide-2 increases intestinal lipid absorption and chylomicron production via CD36. Gastroenterology. 137(3):997–1005, 1005.e1-4. https://doi.org/10.1053/j.gastro.2009.05.051
Hsieh J, Trajcevski KE, Farr SL et al (2015) Glucagon-Like Peptide 2 (GLP-2) Stimulates Postprandial Chylomicron Production and Postabsorptive Release of Intestinal Triglyceride Storage Pools via Induction of Nitric Oxide Signaling in Male Hamsters and Mice. Endocrinology. 156(10):3538–3547. https://doi.org/10.1210/EN.2015-1110
Grande EM, Raka F, Hoffman S, Adeli K (2022) GLP-2 Regulation of Dietary Fat Absorption and Intestinal Chylomicron Production via Neuronal Nitric Oxide Synthase (nNOS) Signaling. Diabetes 71(7):1388–1399. https://doi.org/10.2337/db21-1053
Xiao C, Stahel P, Morgantini C, Nahmias A, Dash S, Lewis GF (2019) Glucagon-like peptide-2 mobilizes lipids from the intestine by a systemic nitric oxide-independent mechanism. Diabetes Obes Metab 21(11):2535–2541. https://doi.org/10.1111/dom.13839
Hein GJ, Baker C, Hsieh J, Farr S, Adeli K (2013) GLP-1 and GLP-2 as yin and yang of intestinal lipoprotein production: evidence for predominance of GLP-2-stimulated postprandial lipemia in normal and insulin-resistant states. Diabetes. 62(2):373–381. https://doi.org/10.2337/db12-0202
Wasada T, McCorkle K, Harris V, Kawai K, Howard B, Unger RH (1981) Effect of gastric inhibitory polypeptide on plasma levels of chylomicron triglycerides in dogs. J Clin Invest 68(4):1106–1107. https://doi.org/10.1172/JCI110335
Ebert R, Nauck M, Creutzfeldt W (1991) Effect of exogenous or endogenous gastric inhibitory polypeptide (GIP) on plasma triglyceride responses in rats. Horm Metab Res 23(11):517–521. https://doi.org/10.1055/s-2007-1003745
Eckel RH, Fujimoto WY, Brunzell JD (1979) Gastric inhibitory polypeptide enhanced lipoprotein lipase activity in cultured preadipocytes. Diabetes. 28(12):1141–1142. https://doi.org/10.2337/diab.28.12.1141
Kim SJ, Nian C, McIntosh CHS (2010) GIP increases human adipocyte LPL expression through CREB and TORC2-mediated trans-activation of the LPL gene. J Lipid Res 51(11):3145–3157. https://doi.org/10.1194/jlr.M006841
Ranganath LR, Beety JM, Morgan LM (1999) Inhibition of insulin, glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) secretion by octreotide has no effect on post-heparin plasma lipoprotein lipase activity. Horm Metab Res 31(4):262–266. https://doi.org/10.1055/s-2007-978729
Thondam SK, Daousi C, Wilding JPH et al (2017) Glucose-dependent insulinotropic polypeptide promotes lipid deposition in subcutaneous adipocytes in obese type 2 diabetes patients: a maladaptive response. Am J Physiol Endocrinol Metab 312(3):E224–E233. https://doi.org/10.1152/ajpendo.00347.2016
Shojaee-Moradie F, Ma Y, Lou S, Hovorka R, Umpleby AM (2013) Prandial hypertriglyceridemia in metabolic syndrome is due to an overproduction of both chylomicron and VLDL triacylglycerol. Diabetes. 62(12):4063–4069. https://doi.org/10.2337/db13-0935
Curtin A, Deegan P, Owens D, Collins P, Johnson A, Tomkin GH (1996) Elevated triglyceride-rich lipoproteins in diabetes. A study of apolipoprotein B-48. Acta Diabetol 33(3):205–210. https://doi.org/10.1007/BF02048544
Haidari M, Leung N, Mahbub F et al (2002) Fasting and postprandial overproduction of intestinally derived lipoproteins in an animal model of insulin resistance. Evidence that chronic fructose feeding in the hamster is accompanied by enhanced intestinal de novo lipogenesis and ApoB48-containing lipoprotein overproduction. J Biol Chem 277(35):31646–31655. https://doi.org/10.1074/jbc.M200544200
Phillips C, Owens D, Collins P, Tomkin GH (2002) Microsomal triglyceride transfer protein: does insulin resistance play a role in the regulation of chylomicron assembly? Atherosclerosis. 160(2):355–360. https://doi.org/10.1016/S0021-9150(01)00721-3
Lally S, Owens D, Tomkin GH (2007) The different effect of pioglitazone as compared to insulin on expression of hepatic and intestinal genes regulating post-prandial lipoproteins in diabetes. Atherosclerosis. 193(2):343–351. https://doi.org/10.1016/j.atherosclerosis.2006.09.031
Zoltowska M, Ziv E, Delvin E et al (2003) Cellular aspects of intestinal lipoprotein assembly in Psammomys obesus: a model of insulin resistance and type 2 diabetes. Diabetes. 52(10):2539–2545. https://doi.org/10.2337/diabetes.52.10.2539
Veilleux A, Grenier E, Marceau P, Carpentier AC, Richard D, Levy E (2014) Intestinal lipid handling: evidence and implication of insulin signaling abnormalities in human obese subjects. Arterioscler Thromb Vasc Biol 34(3):644–653. https://doi.org/10.1161/ATVBAHA.113.302993
Duez H, Lamarche B, Uffelman KD, Valero R, Cohn JS, Lewis GF (2006) Hyperinsulinemia is associated with increased production rate of intestinal apolipoprotein B-48-containing lipoproteins in humans. Arterioscler Thromb Vasc Biol 26(6):1357–1363. https://doi.org/10.1161/01.ATV.0000222015.76038.14
Hogue JC, Lamarche B, Tremblay AJ, Bergeron J, Gagné C, Couture P (2007) Evidence of increased secretion of apolipoprotein B-48-containing lipoproteins in subjects with type 2 diabetes. J Lipid Res 48(6):1336–1342. https://doi.org/10.1194/jlr.M600548-JLR200
Federico LM, Naples M, Taylor D, Adeli K (2006) Intestinal insulin resistance and aberrant production of apolipoprotein B48 lipoproteins in an animal model of insulin resistance and metabolic dyslipidemia: evidence for activation of protein tyrosine phosphatase-1B, extracellular signal-related kinase, and sterol regulatory element-binding protein-1c in the fructose-fed hamster intestine. Diabetes. 55(5):1316–1326. https://doi.org/10.2337/db04-1084
Nogueira JP, Maraninchi M, Béliard S et al (2012) Absence of acute inhibitory effect of insulin on chylomicron production in type 2 diabetes. Arterioscler Thromb Vasc Biol 32(4):1039–1044. https://doi.org/10.1161/ATVBAHA.111.242073
Lewis GF, Uffelman K, Naples M, Szeto L, Haidari M, Adeli K (2005) Intestinal lipoprotein overproduction, a newly recognized component of insulin resistance, is ameliorated by the insulin sensitizer rosiglitazone: studies in the fructose-fed Syrian golden hamster. Endocrinology. 146(1):247–255. https://doi.org/10.1210/en.2004-1143
Phillips C, Mullan K, Owens D, Tomkin GH (2006) Intestinal microsomal triglyceride transfer protein in type 2 diabetic and non-diabetic subjects: the relationship to triglyceride-rich postprandial lipoprotein composition. Atherosclerosis. 187(1):57–64. https://doi.org/10.1016/j.atherosclerosis.2005.08.020
Sasase T, Morinaga H, Yamamoto H et al (2007) Increased fat absorption and impaired fat clearance cause postprandial hypertriglyceridemia in Spontaneously Diabetic Torii rat. Diabetes Res Clin Pract 78(1):8–15. https://doi.org/10.1016/j.diabres.2007.02.020
Gutierrez-Repiso C, Rodriguez-Pacheco F, Garcia-Arnes J et al (2015) The expression of genes involved in jejunal lipogenesis and lipoprotein synthesis is altered in morbidly obese subjects with insulin resistance. Lab Investig 95(12):1409–1417. https://doi.org/10.1038/labinvest.2015.115
Couture P, Tremblay AJ, Kelly I, Lemelin V, Droit A, Lamarche B (2014) Key intestinal genes involved in lipoprotein metabolism are downregulated in dyslipidemic men with insulin resistance. J Lipid Res 55(1):128–137. https://doi.org/10.1194/jlr.M040071
Koffert J, Ståhle M, Karlsson H et al (2018) Morbid obesity and type 2 diabetes alter intestinal fatty acid uptake and blood flow. Diabetes Obes Metab 20(6):1384–1390. https://doi.org/10.1111/dom.13228
Xiao C, Dash S, Morgantini C, Lewis GF (2013) Novel role of enteral monosaccharides in intestinal lipoprotein production in healthy humans. Arterioscler Thromb Vasc Biol 33(5):1056–1062. https://doi.org/10.1161/ATVBAHA.112.300769
Xiao C, Dash S, Morgantini C, Lewis GF (2016) Intravenous Glucose Acutely Stimulates Intestinal Lipoprotein Secretion in Healthy Humans. Arterioscler Thromb Vasc Biol 36(7):1457–1463. https://doi.org/10.1161/ATVBAHA.115.307044
Mamo JC, Watts GF, Barrett PH, Smith D, James AP, Pal S (2001) Postprandial dyslipidemia in men with visceral obesity: an effect of reduced LDL receptor expression? Am J Physiol Endocrinol Metab 281(3):E626–E632. https://doi.org/10.1152/ajpendo.2001.281.3.E626
Chan DC, Watts GF, Barrett PH, Mamo JCL, Redgrave TG (2002) Markers of triglyceride-rich lipoprotein remnant metabolism in visceral obesity. Clin Chem 48(2):278–283. https://doi.org/10.1093/clinchem/48.2.278
Wong ATY, Chan DC, Pang J, Watts GF, Barrett PHR (2014) Plasma apolipoprotein B-48 transport in obese men: a new tracer kinetic study in the postprandial state. J Clin Endocrinol Metab 99(1):E122–E126. https://doi.org/10.1210/jc.2013-2477
Béliard S, Nogueira JP, Maraninchi M et al (2009) Parallel increase of plasma apoproteins C-II and C-III in Type 2 diabetic patients. Diabet Med 26(7):736–739. https://doi.org/10.1111/j.1464-5491.2009.02757.x
Malhotra P, Boddy CS, Soni V et al (2013) D-Glucose modulates intestinal Niemann-Pick C1-like 1 (NPC1L1) gene expression via transcriptional regulation. Am J Physiol Gastrointest Liver Physiol 304(2):G203–G210. https://doi.org/10.1152/ajpgi.00288.2012
Lally S, Tan CY, Owens D, Tomkin GH (2006) Messenger RNA levels of genes involved in dysregulation of postprandial lipoproteins in type 2 diabetes: the role of Niemann-Pick C1-like 1, ATP-binding cassette, transporters G5 and G8, and of microsomal triglyceride transfer protein. Diabetologia. 49(5):1008–1016. https://doi.org/10.1007/s00125-006-0177-8
Chan DC, Watts GF, Barrett PHR, O’Neill FH, Redgrave TG, Thompson GR (2003) Relationships between cholesterol homoeostasis and triacylglycerol-rich lipoprotein remnant metabolism in the metabolic syndrome. Clin Sci (Lond) 104(4):383–388. https://doi.org/10.1042/CS20020298
Ooi EMM, Ng TWK, Chan DC, Watts GF (2009) Plasma markers of cholesterol homeostasis in metabolic syndrome subjects with or without type-2 diabetes. Diabetes Res Clin Pract 85(3):310–316. https://doi.org/10.1016/j.diabres.2009.06.003
Gylling H, Miettinen TA (1997) Cholesterol absorption, synthesis, and LDL metabolism in NIDDM. Diabetes Care 20(1):90–95. https://doi.org/10.2337/diacare.20.1.90
Simonen PP, Gylling HK, Miettinen TA (2002) Diabetes contributes to cholesterol metabolism regardless of obesity. Diabetes Care 25(9):1511–1515. https://doi.org/10.2337/diacare.25.9.1511
Larsen N, Vogensen FK, van den Berg FWJ et al (2010) Gut microbiota in human adults with type 2 diabetes differs from non-diabetic adults. PLoS One 5(2):e9085. https://doi.org/10.1371/journal.pone.0009085
Creely SJ, McTernan PG, Kusminski CM et al (2007) Lipopolysaccharide activates an innate immune system response in human adipose tissue in obesity and type 2 diabetes. Am J Physiol Endocrinol Metab 292(3):E740–E747. https://doi.org/10.1152/ajpendo.00302.2006
Cani PD, Bibiloni R, Knauf C et al (2008) Changes in gut microbiota control metabolic endotoxemia-induced inflammation in high-fat diet-induced obesity and diabetes in mice. Diabetes. 57(6):1470–1481. https://doi.org/10.2337/db07-1403
Sato H, Zhang LS, Martinez K et al (2016) Antibiotics Suppress Activation of Intestinal Mucosal Mast Cells and Reduce Dietary Lipid Absorption in Sprague-Dawley Rats. Gastroenterology. 151(5):923–932. https://doi.org/10.1053/j.gastro.2016.07.009
Jin Y, Wu Y, Zeng Z et al (2016) From the Cover: Exposure to Oral Antibiotics Induces Gut Microbiota Dysbiosis Associated with Lipid Metabolism Dysfunction and Low-Grade Inflammation in Mice. Toxicol Sci 154(1):140–152. https://doi.org/10.1093/toxsci/kfw150
Li X, Zhang Z, Cheng J et al (2019) Dietary supplementation of soybean-derived sterols regulates cholesterol metabolism and intestinal microbiota in hamsters. J Funct Foods 59:242–250. https://doi.org/10.1016/j.jff.2019.05.032
Le Chatelier E, Nielsen T, Qin J et al (2013) Richness of human gut microbiome correlates with metabolic markers. Nature. 500(7464):541–546. https://doi.org/10.1038/nature12506
Cotillard A, Kennedy SP, Kong LC et al (2013) Dietary intervention impact on gut microbial gene richness. Nature. 500(7464):585–588. https://doi.org/10.1038/nature12480
Guevara-Cruz M, Flores-López AG, Aguilar-López M et al (2019) Improvement of Lipoprotein Profile and Metabolic Endotoxemia by a Lifestyle Intervention That Modifies the Gut Microbiota in Subjects With Metabolic Syndrome. J Am Heart Assoc 8(17):e012401. https://doi.org/10.1161/JAHA.119.012401
Tolhurst G, Heffron H, Lam YS et al (2012) Short-chain fatty acids stimulate glucagon-like peptide-1 secretion via the G-protein-coupled receptor FFAR2. Diabetes. 61(2):364–371. https://doi.org/10.2337/db11-1019
Thomas C, Gioiello A, Noriega L et al (2009) TGR5-mediated bile acid sensing controls glucose homeostasis. Cell Metab 10(3):167–177. https://doi.org/10.1016/j.cmet.2009.08.001
Briand F, Thiéblemont Q, Muzotte E, Sulpice T (2012) High-fat and fructose intake induces insulin resistance, dyslipidemia, and liver steatosis and alters in vivo macrophage-to-feces reverse cholesterol transport in hamsters. J Nutr 142(4):704–709. https://doi.org/10.3945/jn.111.153197
Jeppesen J, Zhou MY, Chen YD, Reaven GM (1994) Effect of metformin on postprandial lipemia in patients with fairly to poorly controlled NIDDM. Diabetes Care 17(10):1093–1099. https://doi.org/10.2337/diacare.17.10.1093
Sato D, Morino K, Nakagawa F et al (2017) Acute Effect of Metformin on Postprandial Hypertriglyceridemia through Delayed Gastric Emptying. Int J Mol Sci 18(6):E1282. https://doi.org/10.3390/ijms18061282
Preiss D, Dawed A, Welsh P et al (2017) Sustained influence of metformin therapy on circulating glucagon-like peptide-1 levels in individuals with and without type 2 diabetes. Diabetes Obes Metab 19(3):356–363. https://doi.org/10.1111/dom.12826
Jeppesen J, Zhou MY, Chen YD, Reaven GM (1994) Effect of glipizide treatment on postprandial lipaemia in patients with NIDDM. Diabetologia. 37(8):781–787. https://doi.org/10.1007/BF00404335
Vakkilainen J, Mero N, Schweizer A, Foley JE, Taskinen MR (2002) Effects of nateglinide and glibenclamide on postprandial lipid and glucose metabolism in type 2 diabetes. Diabetes Metab Res Rev 18(6):484–490. https://doi.org/10.1002/dmrr.324
Mieszczanska H, Kaba NK, Francis CW et al (2007) Effects of pioglitazone on fasting and postprandial levels of lipid and hemostatic variables in overweight non-diabetic patients with coronary artery disease. J Thromb Haemost 5(5):942–949. https://doi.org/10.1111/j.1538-7836.2007.02442.x
Al Majali K, Cooper MB, Staels B, Luc G, Taskinen MR, Betteridge DJ (2006) The effect of sensitisation to insulin with pioglitazone on fasting and postprandial lipid metabolism, lipoprotein modification by lipases, and lipid transfer activities in type 2 diabetic patients. Diabetologia. 49(3):527–537. https://doi.org/10.1007/s00125-005-0092-4
van Wijk JPH, de Koning EJP, Castro Cabezas M, Rabelink TJ (2005) Rosiglitazone improves postprandial triglyceride and free fatty acid metabolism in type 2 diabetes. Diabetes Care 28(4):844–849. https://doi.org/10.2337/diacare.28.4.844
Chappuis B, Braun M, Stettler C et al (2007) Differential effect of pioglitazone (PGZ) and rosiglitazone (RGZ) on postprandial glucose and lipid metabolism in patients with type 2 diabetes mellitus: a prospective, randomized crossover study. Diabetes Metab Res Rev 23(5):392–399. https://doi.org/10.1002/dmrr.715
James AP, Watts GF, Mamo JCL (2005) The effect of metformin and rosiglitazone on postprandial lipid metabolism in obese insulin-resistant subjects. Diabetes Obes Metab 7(4):381–389. https://doi.org/10.1111/j.1463-1326.2004.00407.x
Hanefeld M, Fischer S, Schulze J et al (1991) Therapeutic potentials of acarbose as first-line drug in NIDDM insufficiently treated with diet alone. Diabetes Care 14(8):732–737. https://doi.org/10.2337/diacare.14.8.732
Ogawa S, Takeuchi K, Ito S (2004) Acarbose lowers serum triglyceride and postprandial chylomicron levels in type 2 diabetes. Diabetes Obes Metab 6(5):384–390. https://doi.org/10.1111/j.1462-8902.2004.00362.x
Nakano T, Inoue I, Seo M, Takahashi S, Komoda T, Katayama S (2009) Acarbose attenuates postprandial hyperlipidemia: investigation in an intestinal absorptive cell model. Metabolism. 58(5):583–585. https://doi.org/10.1016/j.metabol.2009.02.003
Varin EM, Hanson AA, Beaudry JL et al (2020) Hematopoietic cell- versus enterocyte-derived dipeptidyl peptidase-4 differentially regulates triglyceride excursion in mice. JCI Insight 5(16):140418. https://doi.org/10.1172/jci.insight.140418
Tremblay AJ, Lamarche B, Deacon CF, Weisnagel SJ, Couture P (2011) Effect of sitagliptin therapy on postprandial lipoprotein levels in patients with type 2 diabetes. Diabetes Obes Metab 13(4):366–373. https://doi.org/10.1111/j.1463-1326.2011.01362.x
Matikainen N, Mänttäri S, Schweizer A et al (2006) Vildagliptin therapy reduces postprandial intestinal triglyceride-rich lipoprotein particles in patients with type 2 diabetes. Diabetologia. 49(9):2049–2057. https://doi.org/10.1007/s00125-006-0340-2
Eliasson B, Möller-Goede D, Eeg-Olofsson K et al (2012) Lowering of postprandial lipids in individuals with type 2 diabetes treated with alogliptin and/or pioglitazone: a randomised double-blind placebo-controlled study. Diabetologia. 55(4):915–925. https://doi.org/10.1007/s00125-011-2447-3
Xiao C, Dash S, Morgantini C, Patterson BW, Lewis GF (2014) Sitagliptin, a DPP-4 inhibitor, acutely inhibits intestinal lipoprotein particle secretion in healthy humans. Diabetes. 63(7):2394–2401. https://doi.org/10.2337/db13-1654
Vergès B, Duvillard L, Pais de Barros JP et al (2018) Liraglutide Reduces Postprandial Hyperlipidemia by Increasing ApoB48 (Apolipoprotein B48) Catabolism and by Reducing ApoB48 Production in Patients With Type 2 Diabetes Mellitus. Arterioscler Thromb Vasc Biol 38(9):2198–2206. https://doi.org/10.1161/ATVBAHA.118.310990
Hermansen K, Bækdal TA, Düring M et al (2013) Liraglutide suppresses postprandial triglyceride and apolipoprotein B48 elevations after a fat-rich meal in patients with type 2 diabetes: a randomized, double-blind, placebo-controlled, cross-over trial. Diabetes Obes Metab 15(11):1040–1048. https://doi.org/10.1111/dom.12133
Voukali M, Kastrinelli I, Stragalinou S et al (2014) Study of postprandial lipaemia in type 2 diabetes mellitus: exenatide versus liraglutide. J Diabetes Res 2014:304032. https://doi.org/10.1155/2014/304032
Dahl K, Brooks A, Almazedi F, Hoff ST, Boschini C, Baekdal TA (2021) Oral semaglutide improves postprandial glucose and lipid metabolism, and delays gastric emptying, in subjects with type 2 diabetes. Diabetes Obes Metab 23(7):1594–1603. https://doi.org/10.1111/dom.14373
Xiao C, Bandsma RHJ, Dash S, Szeto L, Lewis GF (2012) Exenatide, a glucagon-like peptide-1 receptor agonist, acutely inhibits intestinal lipoprotein production in healthy humans. Arterioscler Thromb Vasc Biol 32(6):1513–1519. https://doi.org/10.1161/ATVBAHA.112.246207
Taskinen MR, Björnson E, Matikainen N et al (2021) Effects of liraglutide on the metabolism of triglyceride-rich lipoproteins in type 2 diabetes. Diabetes Obes Metab 23(5):1191–1201. https://doi.org/10.1111/dom.14328
Whyte MB, Shojaee-Moradie F, Sharaf SE et al (2019) Lixisenatide Reduces Chylomicron Triacylglycerol by Increased Clearance. J Clin Endocrinol Metab 104(2):359–368. https://doi.org/10.1210/jc.2018-01176
Sawada T, Uzu K, Hashimoto N et al (2020) Empagliflozin’s Ameliorating Effect on Plasma Triglycerides: Association with Endothelial Function Recovery in Diabetic Patients with Coronary Artery Disease. J Atheroscler Thromb 27(7):644–656. https://doi.org/10.5551/jat.50807
Kamijo Y, Ishii H, Yamamoto T et al (2019) Potential Impact on Lipoprotein Subfractions in Type 2 Diabetes. Clin Med Insights Endocrinol Diabetes 12:1179551419866811. https://doi.org/10.1177/1179551419866811
Xiao C, Pavlic M, Szeto L, Patterson BW, Lewis GF (2011) Effects of acute hyperglucagonemia on hepatic and intestinal lipoprotein production and clearance in healthy humans. Diabetes. 60(2):383–390. https://doi.org/10.2337/db10-0763
Dash S, Xiao C, Stahel P, Koulajian K, Giacca A, Lewis GF (2018) Evaluation of the specific effects of intranasal glucagon on glucose production and lipid concentration in healthy men during a pancreatic clamp. Diabetes Obes Metab 20(2):328–334. https://doi.org/10.1111/dom.13069
Author’s relationships and activities
The author declares that there are no relationships or activities that might bias, or be perceived to bias, this review.
Contribution statement
The author was the sole contributor to this paper
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Slideset of figures
(PPTX 699 kb)
Rights and permissions
About this article

Cite this article
Vergès, B. Intestinal lipid absorption and transport in type 2 diabetes. Diabetologia 65, 1587–1600 (2022). https://doi.org/10.1007/s00125-022-05765-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-022-05765-8