
Prognosis of shoulder pain in those with and without a psychological disorder: A prospective cohort study with a six-month follow-up
Abstract
BACKGROUND:
Because shoulder pain can have an unfavorable prognosis, it is important to have a better understanding of factors that may influence recovery.
OBJECTIVE:
To determine the association between recovery from shoulder pain and the presence of depression, anxiety, and pain catastrophizing.
METHODS:
In a prospective cohort study with a six months follow-up, we included patients visiting an orthopaedic department with shoulder pain. Primary outcome was recovery from shoulder pain measured with the Shoulder Pain and Disability Index at three and six months. Information about depression and anxiety (Hospital Anxiety and Depression Scale), pain catastrophizing (Pain Catastrophizing Scale), and demographic and clinical factors were collected at baseline. A linear mixed model was used to estimate the effects of depression, anxiety, pain catastrophizing, and underlying shoulder disorders on recovery.
RESULTS:
We included 190 patients. There were no statistically significant associations between the presence of depression, anxiety, and pain catastrophizing, and three- and six-month recovery. Also between the underlying shoulder disorders and recovery at three and six months, there were no statistically significant associations.
CONCLUSIONS
: We could not prove that depression, anxiety, and pain catastrophizing, as well as underlying shoulder disorders, were associated with recovery of shoulder pain at six months.
1.Introduction
Shoulder complaints comprise an important public health problem with an annual prevalence of 47% [1]. Only in 50–60% of patients with shoulder complaints, conservative treatment leads to satisfactory outcomes after 6–12 months. Moreover, more than half of these patients experience recurrence of symptoms in the long term [2, 3].
As a result, socioeconomic burdens are considerable due to extensive use of health care services, mainly for surgical interventions, and work-related costs [4, 5]. Considering the high prevalence and substantial socioeconomic burden, as well as patient’s suffering, it is important to have a better understanding of factors that may influence recovery, preferably modifiable factors, in order to identify the most optimal treatment interventions.
Currently, primary and secondary care guidelines for shoulder complaints focus their treatment strategies on biomedical interventions, e.g. corticosteroid injections, physiotherapy and surgery [6, 7]. However, shoulder complaints are a complex problem, and especially in case of chronic pain, cannot be explained solely by an obvious pathoanatomic disorder. Inside the biopsychosocial understanding of chronic pain, there is growing evidence that psychological factors may influence prognosis; In patients with non-specific low-back pain, studies have shown that the prognosis is associated with psychological factors, and treatment tailored at these psychological factors led to better treatment outcomes and was cost-effective [8]. As most musculoskeletal disorders share similar psychological prognostic factors [9], this might also apply to patients with shoulder complaints.
Psychological factors such as depression and anxiety, present in about one-fourth of patients with subacromial pain syndrome [10], and pain catastrophizing is known to influence pain experience and disability levels [10, 11]. Despite this association, two recent meta-analyses indicate that the prognosis of shoulder pain is not influenced by depression, anxiety and pain catastrophizing [12, 13]. So far, these psychological factors have only been studied in heterogeneous study populations with respect to the underlying shoulder disorders. It is known that the prognosis of different shoulder disorders varies significantly. For example, a frozen shoulder has an average recovery time of 30 months, whereas it is believed that subacromial bursitis tends to recover more quickly [14]. It is plausible that prognosis can be influenced by both psychological factors and the underlying cause of shoulder pain, however, this has yet to be established.
Therefore, the aims of this study were (i) to determine the association between recovery of shoulder pain and the presence of depression, anxiety and pain catastrophizing; and (ii) to determine the association of the underlying shoulder disorders with recovery.
2.Methods
We conducted this study in compliance with the principles of the Declaration of Helsinki. The study’s protocol was reviewed and approved by the Institutional Review Board of Zuyderland Medical Centre (IRB no. 17-N-171). Written informed consent was obtained.
2.1Study design and setting
This prospective cohort study with a follow-up of six months was conducted at two different clinics of the orthopaedic department of a regional hospital in the province of Limburg, The Netherlands. This orthopaedic department is characterised by two different clinics: an outpatient and an outreach clinic. The difference between the two clinics is that the outreach clinic, a joint initiative with the regional general practice organization, focuses on substitution of orthopaedic care from the hospital setting to a primary care setting, predominantly for low complexity orthopaedic complaints. All patients were seen by an orthopedic surgeon with imaging depending on the complaint. Applied treatment was based on guidelines for Dutch orthopedic surgeons [15].
2.2Participants
A consecutive sample of patients with shoulder pain, visiting the department for the first time, was included if they met the following criteria: unilateral shoulder complaints considered to be of musculoskeletal origin, and aged
2.3Data collection
During a four months study period (December 2018 and March 2019) patients were included, and data was collected from their Electronic Medical Records (EMR) and distributed questionnaires. Information about the patients’ sex, age, and hand dominance was collected, as well as information about their shoulder diagnosis, affected side, duration of complaints, complaint onset, previous episode(s) and previous treatments. At the time of first consultation in the clinic, the baseline questionnaire was completed. At three and six months follow-up questionnaires were sent to the patients by post accompanied by a reply-paid envelope. In case of non-response after one week, patients received a reminder by post.
2.4Outcome measures
The primary outcome measure was measured at baseline and prospectively at three and six months after inclusion, while the potential prognostic factors were measured only at baseline.
2.4.1Primary outcome measure
To assess recovery, the Shoulder Pain and Disability Index (SPADI) as primary outcome measure was used. This questionnaire consists of 13 items divided into two subcategories pain and limitation in activities, and comprises five pain-related items and eight disability-related items, caused by shoulder problems during the last week. Answer options are based on a Numerical Rating Scale (NRS), whereas 0
2.4.2Potential psychological prognostic factors
The Hospital Anxiety and Depression Scale (HADS) and Pain Catastrophizing Scale (PCS) were used to evaluate psychological prognostic factors. The HADS was used to measure the core symptoms of anxiety and depression and can be used in a population aged 16–80 [20]. The scale examines feelings over the past four weeks and consists of 14 items, equally divided over a subscale for depression and one for anxiety. Patients answer the questions using a 4-point Likert scale (0–3), with a maximum total score of 21 of both subscales. The higher the patient scores, the more complaints the patient experiences. Cronbach’s alpha for the anxiety subscale varies from 0.68 to 0.93 (mean 0.83) and for the depression subscale from 0.67 to 0.90 (mean 0.82) [21]. A cut-off value of
The PCS was used to assess pain catastrophizing, described as an exaggerated negative orientation towards noxious stimuli [22]. It plays an important role in the experience of pain and its coping. The PCS consists of 13 statements that contain thoughts and feelings that patients may experience when having pain. The items are divided into the categories rumination (4 items), magnification (3 items), and helplessness (6 items), where each item is scored on a 5-point scale (0–4), with a maximum score of 52 for all 13 items together [23]. A cut-off of
Questionnaires were considered incomplete when more than two items were missing in one subscale of the SPADI [24], more than two items missing in the PCS [22, 25], or more than half of the items missing in one subscale of the HADS [26]. In case fewer items were missing, the SPADI was calculated by dividing the sum score only by answered items [24], while for the PCS and HADS, an average score of the other subscale items was imputed for the absent item [22, 25, 26].
2.4.3Other potential prognostic factors
Also non-psychological potential prognostic factors were assessed. As shown in Fig. 1 they were divided into five subcategories: demographic, clinical, shoulder diagnosis, and orthopaedic clinic. These factors included both self-selected potential factors and those selected from the literature:
Figure 1.
Potential factors influencing recovery. AC: acromioclavicular disorder; CSI: corticosteroid injection; GH: glenohumeral disorder; HADS: Hospital Anxiety and Depression Scale; PCS: Pain Catastrophizing Scale; SAPS: subacromial pain syndrome; SPADI: Shoulder Pain and Disability Index.
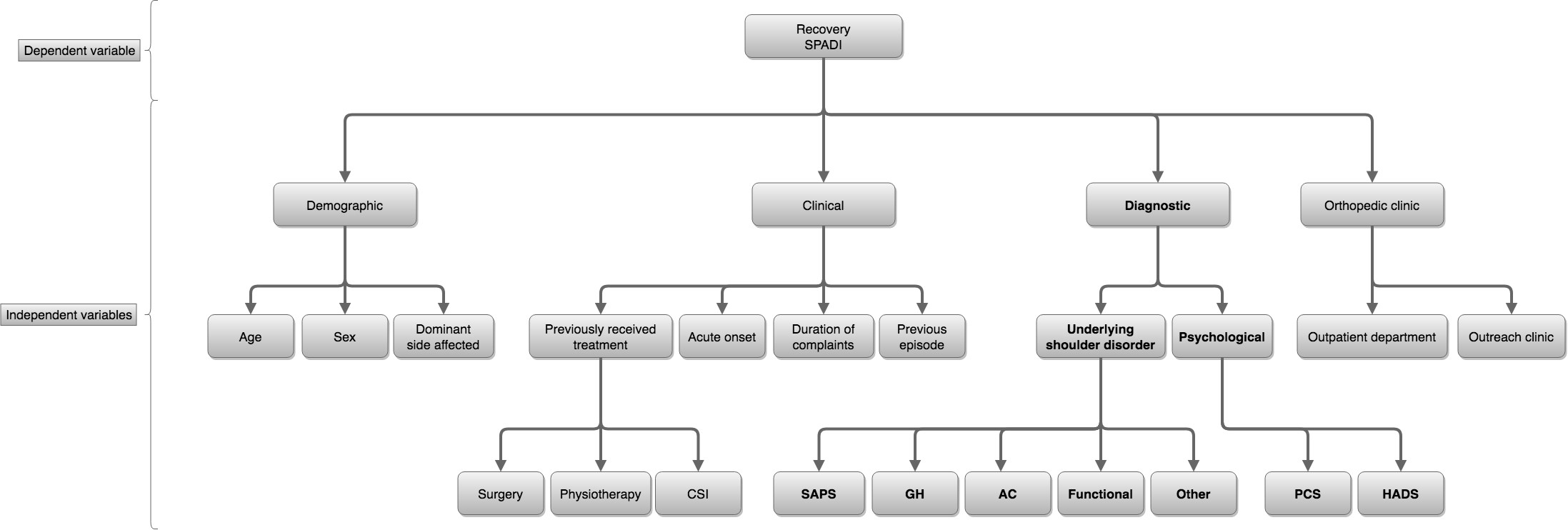
1. Demographic factors: age, sex, and dominant side affected;
2. Clinical factors: acute onset, duration of complaints, previous episodes, and previous treatment (corticosteroid injection, physiotherapy, or surgery)
3. Shoulder diagnosis: subacromial pain syndrome (SAPS), glenohumeral disorder, acromioclavicular (AC) disorder, functional disorder, and other pathology (e.g. biceps pathology, cervicobrachialgia);
4. Orthopaedic clinics: outpatient and outreach clinic.
2.5Sample size
On an annual basis, approximately 2000 new patients with shoulder complaints are seen in both clinics. During a four-month period, one research team member (GS) was available two days a week to recruit a consecutive sample of patients and to supervise the informed consent procedure. This allowed the researcher to assess eligibility of approximately 260 patients. Assuming that 75% of the patients were eligible and that the vast majority would participate because the investigator asked them personally and completing the questionnaires has a low burden, we expected to include 200 patients. This number is large enough to include all psychological diagnoses and underlying shoulder disorders in one model, correcting for other prognostic factors such as age, sex, and duration of complaints.
2.6Data analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows version 26 (Armonk, NY, USA). Numerical variables are presented as mean with standard deviation (SD), while number of patients (%) are reported for categorical variables. Differences in numerical characteristics between clinics or among response subgroups (full-, partial or non-responders) were compared using the independent-samples
A linear mixed model analysis with an unstructured covariance structure for repeated measures was performed to assess the effects of the psychological diagnoses and underlying shoulder disorders on total SPADI score at 3 and 6 months with correction for baseline differences. The fixed part of the model contains these diagnoses and disorders, time (0, 3, and 6 months) and interaction between these factors with time. In addition, other prognostic variables (age, sex, dominant side affected, duration of complaints, and orthopaedic centre) were included to correct for their potential confounding effect. A likelihoodbased approach was used for missing outcome data, assuming missingness to be at random (MAR). Prognostic factors with too many missing values and/or a low prevalence (
Finally, two sensitivity analyses through a linear mixed model were performed. First to analyze the effect of distinguishing the pathoanatomical disorders by clustering the four different disorders (SAPS, glenohumeral disorder, AC disorder, and another disorder) into one group and comparing them with functional disorders. We anticipated that not all participants would return their questionnaires. That is why this study has three subgroups of respondents: (i) full-responders, who returned all questionnaires; (ii) partial-responders, who only responded at 3 or 6 months; and (iii) non-responders, who did not respond after baseline. Therefore, this study also analyzed the effect of missing values by including only full-responders.
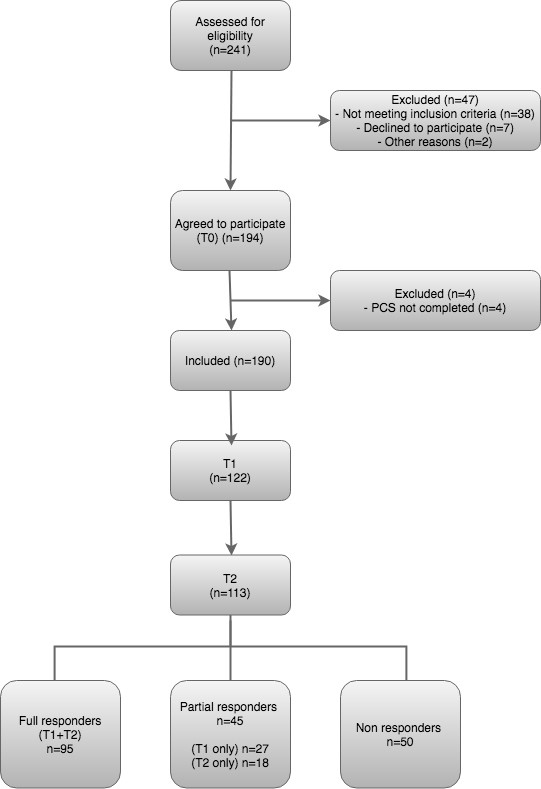
Figure 2.
Flowchart of patients throughout the study.
Two-sided
3.Results
A total of 241 patients were assessed for eligibility. Thirty-eight patients were excluded for not meeting the inclusion criteria, seven declined to participate, and two were excluded due to other reasons, resulting in 194 included patients who provided baseline data. Finally, four patients were additionally excluded because they did not complete the PCS at baseline. This measurement was required because the study aim concerns the effect of PCS and HADS on SPADI, and for this reason only patients with complete baseline measurements of the PCS and HADS were included in the analysis. This resulted in a study population of 190 patients; 98 (52%) were included at the outreach clinic and 92 (48%) at the outpatient clinic. Of them, 122 (64%) provided outcome data at three months and 113 (59%) at six months. Based on these numbers, there were 95 full-responders (50%) 45 partial-responders (24%) and 50 non-responders (26%). This flow of patients is illustrated in Fig. 2. Differences in baseline characteristics between the two orthopaedic clinics and the three response subgroups are presented in supplementary data Table S1.
Table 1
Baseline characteristics of the patients included in the analysis (
| Variables | ||
|---|---|---|
| Demographic | ||
| Females, | 87 | (45.8) |
| Age, mean (SD) | 57.0 | (13.2) |
| Dominant side affected, | 108 | (58.1) |
| Primary outcome | ||
| SPADI, mean (SD) | 60.2 | (21.3) |
| Psychological disorder | ||
| PCS, mean (SD) | 19.1 | (11.4) |
| Catastrophizing, cut-off | 36 | (18.9) |
| HADS, mean (SD) | 10.2 | (7.0) |
| Anxiety, cut-off | 53 | (27.9) |
| Depression, cut-off | 42 | (22.1) |
|
Shoulder disorder, | ||
| SAPS | 123 | (64.7) |
| Glenohumeral disorder | 29 | (15.3) |
| AC disorder | 32 | (16.8) |
| Functional disorder | 23 | (12.1) |
| Other disorder | 21 | (11.1) |
| Clinical | ||
| Duration of shoulder pain, | ||
| 0–6 months | 91 | (52.0) |
| | 84 | (48.0) |
| Missing | 15 | (7.9) |
| Acute onset, | 56 | (82.4) |
| Missing, | 122 | (64.2) |
| Previous episode | 30 | (23.1) |
| Missing | 60 | (31.6) |
| Previous treatment, | ||
| Physiotherapy | 101 | (63.5) |
| Missing | 31 | (16.3) |
| Corticosteroid injection | 52 | (37.4) |
| Missing | 51 | (26.8) |
| Surgery | 7 | (3.7) |
| Initial applied management, | ||
| Advice only | 11 | (5.8) |
| Painkillers | 49 | (25.8) |
| Corticosteroid injections | 69 | (36.3) |
| Physical exercise | 124 | (65.3) |
| Additional imaging | 15 | (7.9) |
| Surgery | 3 | (1.6) |
| Barbotage therapy for calcification | 8 | (4.2) |
| Referral to other medical specialist | 2 | (1.1) |
SPADI: Shoulder Pain and Disability Index total score (score 0–100); PCS: Pain Catastrophizing Scale (score 0–52); HADS: Hospital Anxiety and Depression Scale (score 0–42); SAPS: subacromial pain syndrome; AC: acromioclavicular;
Baseline characteristics of the patients included in the analysis are shown in Table 1. The mean (
3.1Longitudinal effects on recovery
The potential prognostic factors complaint onset (64%,
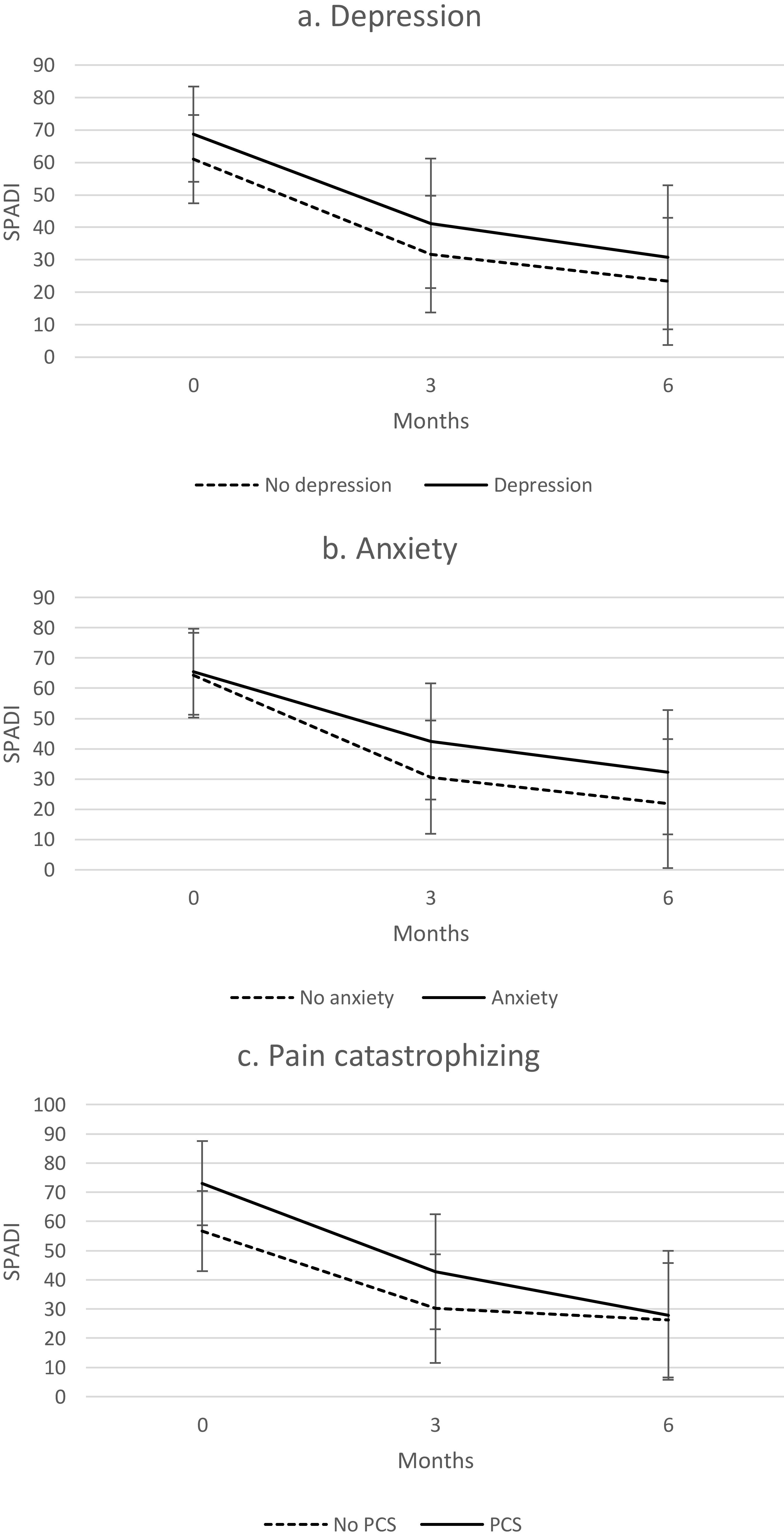
At six months, a non-significant greater improvement in total SPADI score was seen in patients with a depression compared to those without (mean difference in change from baseline (B)
Also for the underlying shoulder disorders, non-significant differences were observed at three and six months. All observed means at baseline, three, and six months, as well as the mean change from baseline, are shown in Table 2, where the longitudinal trends for the three psychological disorders are also presented in Fig. 3.
Table 2
Observed means, mean changes from baseline and estimated mean difference in change from baseline for total SPADI score at 3 and 6 months for the three psychological and five underlying shoulder disorders
| Observed means | Estimated mean difference | ||||||
| Disorder | |||||||
| Present | Absent | ||||||
| Variables | Mean (SD) | Mean (SD) | B (95% CI) | ||||
| Psychological disorder | |||||||
| Depression | |||||||
| Baseline | 68.7 | (18.8) | 57.8 | (21.4) | |||
| Change at 3 months | (17.8) | (23.5) | 1.8 | ( | 0.752 | ||
| Change at 6 months | (23.2) | (27.7) | ( | 0.964 | |||
| Anxiety | |||||||
| Baseline | 66.3 | (19.3) | 57.8 | (21.7) | |||
| Change at 3 months | (21.5) | (22.5) | 10.6 | ( | 0.056 | ||
| Change at 6 months | (24.3) | (27.5) | 9.1 | ( | 0.215 | ||
| Pain catastrophizing | |||||||
| Baseline | 75.1 | (18.1) | 56.6 | (20.5) | |||
| Change at 3 months | (24.4) | (22.4) | ( | 0.533 | |||
| Change at 6 months | (25.8) | (27.0) | ( | 0.045 | |||
| Shoulder disorder | |||||||
| SAPS | |||||||
| Baseline | 62.0 | (20.0) | 56.9 | (23.3) | |||
| Change at 3 months | (24.2) | (18.9) | ( | 0.284 | |||
| Change at 6 months | (29.1) | (20.6) | ( | 0.33 | |||
| Glenohumeral disorder | |||||||
| Baseline | 65.2 | (16.9) | 59.3 | (21.9) | |||
| Change at 3 months | (23.9) | (22.3) | 0.8 | ( | 0.93 | ||
| Change at 6 months | (18.4) | (28.0) | ( | 0.30 | |||
| AC disorder | |||||||
| Baseline | 64.8 | (22.3) | 59.3 | (21.1) | |||
| Change at 3 months | (30.6) | (20.3) | ( | 0.30 | |||
| Change at 6 months | (27.4) | (26.7) | ( | 0.32 | |||
| Functional disorder | |||||||
| Baseline | 48.7 | (22.9) | 61.9 | (20.6) | |||
| Change at 3 months | (15.1) | (23.3) | ( | 0.21 | |||
| Change at 6 months | (19.5) | (27.7) | ( | 0.30 | |||
| Other disorder | |||||||
| Baseline | 54.8 | (25.5) | 60.9 | (20.7) | |||
| Change at 3 months | (15.5) | (23.3) | ( | 0.62 | |||
| Change at 6 months | (22.8) | (26.6) | 1.8 | ( | 0.88 | ||
SAPS: subacromial pain syndrome; AC: acromioclavicular.
Figure 3.
Total SPADI score estimated marginal means with 95% confidence intervals for a) Depression, b) Anxiety and c) Pain catastrophizing.
The two sensitivity analyses showed no effect of clustering the four pathoanatomical disorder groups (SAPS, glenohumeral disorder, AC disorder, and another disorder) into one group, and of including only full-responders in the analysis, i.e. similar results were found.
4.Discussion
This study presents evidence that the psychological disorders depression, anxiety, and pain catastrophizing, as well as underlying shoulder disorders, are not significantly associated with recovery of shoulder pain at six months. Although we found a clinically relevant greater improvement in total SPADI score at 6 months in those patients with pain catastrophizing than those without (SPADI difference in change from baseline
The present study observed that both depression and anxiety were present in approximately one-fourth of the study population with shoulder pain, which is consistent with results from a systematic review [10]. Prevalence of pain catastrophizing in shoulder patients presenting in orthopaedic clinics has yet not been reported, however, it is known that 25% of patients with chronic pain suffer from pain catastrophizing [23]. This is marginally higher than in the present study where 19% was found. The observed prevalence of these psychological disorders indicates that our study population seems representative of the population of patients with shoulder pain seen at an orthopaedic clinic.
The results of the present study indicating that depression, anxiety and pain catastrophizing are not significantly associated with recovery of shoulder pain are in line with two systematic reviews [12, 13], which is in contrast to studies investigating patients with low back pain and knee pain [27]. Reasons behind these contrasting findings may lie in the populations studied. In many patients with shoulder pain, a specific patho-anatomical diagnosis can be established, where for example in patients with low back pain, the diagnosis remains non-specific in most patients. Besides the availability of specific treatments for these specific shoulder disorders, this uncertainty about the diagnosis might contribute to anxious and depressive feelings, while in patients with pain catastrophizing this can maintain the overly negative orientation to painful stimuli.
It is noteworthy that in the present study patients with pain catastrophizing showed greater improvement than those without, although at six months, both subgroups showed similar total SPADI scores. It is known that pain catastrophizing is associated with shoulder pain at baseline [10], but the tendency towards a greater improvement at six months has not been described in the literature. A possible explanation for this phenomenon could lie in the information provided by the orthopaedic surgeon, which reassures the patient and offers perspective on recovery. The findings that expectations of recovery predict treatment outcome and baseline optimism moderates the relation between pain catastrophizing and shoulder disability following physiotherapy treatment [13], substantiates this idea.
Heterogeneity of applied outcome measures may be another reason why conflicting associations between recovery and psychological factors are found in the different study populations. To measure depression and anxiety, we used the HADS questionnaire, while a variety of other outcome measures was used in other studies, e.g. SF-12 Mental Component Summary, one item of EQ-5D, Centre for Epidemiological Studies Depression Scale, and a psychologist interview based on the DSM-III-R. Differences in construct validity of these outcome measures can lead to differences in specificity to detect depression and anxiety [12, 13].
The strengths of this study are that it is the first to describe the association between both psychological factors and underlying shoulder disorders with recovery of shoulder pain, the prospective design, and the possibility of adjusting for several potential confounding factors. We used the SPADI to measure recovery, which has good reliability and validity [17]. Likewise, the HADS and PCS have been shown to be valid indicators of possible depression and anxiety, and pain catastrophizing, respectively, in clinical practice [20, 21, 22, 23]. To avoid the burden of filling in too many questions, we chose to include only the psychological factors of depression, anxiety and pain catastrophizing in this present study. This can be seen as a limitation, however, we aimed at preventing selection bias. By limiting the time taken to participate in the study, we hoped that all the consecutive patients asked would actually participate. Since only 3% of the assessed patients (
On the other hand, it is known that other psychological factors might influence recovery, e.g. fear-avoidance beliefs and self-efficacy [13]. The choice for selecting depression, anxiety and pain catastrophizing was based on the fact that, so far, no evidence could be found that they can predict recovery, while for the other psychological factors, there seems to be an association [13]. Not including these other psychological factors can be regarded as a limitation. Another limitation is that we excluded five potential prognostic factors for analysis due to a high number of missing values (complaint onset, previous episode, previous corticosteroid injection and physiotherapy) and previous surgery due to a low prevalence. To assess the effect of missing outcome data, we conducted a sensitivity analysis by including only full-responders, which showed no differences in effect. Especially in the patients who were included at the outpatient department it was observed that more values were missing. The explanation for this is that we used the data from the EMR without making agreements about uniform reporting. At the outreach clinic a fixed format for history taking and physical examination is used, while at the outpatient department notes are made in the EMR as they see fit. The procedure at the outreach clinic ensures that missing data will be limited.
We included a heterogenic patient group in terms of diagnosis and previous interventions carried out in primary care, which had an impact on the numbers in the subgroups. These subgroups are too small to do additional analyses, so the results need to be read for the entire shoulder pain population.
Treatment expectations or preferences are important because they can affect patient satisfaction, adherence to treatment plans, and patient outcomes [28]. Treatment expectations and preferences were not assessed, as this was not an intervention study. Initial treatment was based on shared decision making, and patients chose their own exercise therapist if applicable. Therefore, we believe that the chance that patients have started an unappreciated treatment is small. During follow-up, we did not assess which treatments were used, because our aim was not to predict specific treatment outcomes. Whether psychological factors play a role in selecting patients for surgery, cannot be determined with the current study. Finally, although we used a likelihood-based approach for incomplete responses, there might be an attrition bias.
Knowledge about prognostic modifiable risk factors could be useful to inform and direct treatment decisions in patients with shoulder pain. Currently, treatment strategies focus not on psychological factors [6, 7], and the current study indicates that there is still no evidence to suggest that doing so provides a better prognosis. This does not alter the fact that treatment can be adjusted to individual psychological factors if these appear to be relevant for the prognosis. A holistic approach with an adequate explanation of the disorder and treatment strategy is essential for patients. On the one hand this will promote compliance, and on the other hand it will increase the acceptance of complaints. Due to lack of time, however, this is a challenge in daily practice.
Since again no association has been shown between psychological factors and recovery from shoulder pain, does not mean that we should stop research this field. We may need to use other outcome measures. Different musculoskeletal pain conditions often share common underlying mechanisms and a similar clinical course on average. Moreover, similar prognostic factors may predict outcomes [9, 29, 30]. In patients with low back pain in general practice, treatment tailored at psychological factors led to better outcomes [8]. In this low back pain study, instead of a separate outcome measure for each psychological factor, a multidimensional biopsychosocial outcome measure was used, the STarT Back Screening Tool. Recently, a modified, generic version of this tool was developed for patients with the five most common musculoskeletal pain presentations in general practice: shoulder, neck, back, knee or multisite pain, the STarT MSK tool [31]. This tool includes ten different biopsychosocial constructs, among which pain intensity, pain duration, depression, fear of movement and pain self-efficacy. Future research is recommended to include a multidimensional biopsychosocial outcome measure, for example by using the STarT MSK tool.
5.Conclusion
In this study, we could not prove that depression, anxiety, and pain catastrophizing, as well as underlying shoulder disorders, were associated with recovery of shoulder pain at six months in patients visiting an orthopaedic department. For future prospective research, we advise to include a multidimensional biopsychosocial outcome measure instead of outcome measures per disorder.
Acknowledgments
We would like to thank the staff of MCC Omnes, Meditta Medical Center and the orthopaedic department of Zyderland MC for their assistance in this research.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The authors report no funding.
References
[1] | Luime JJ, Koes BW, Hendriksen IJ, et al. Prevalence and incidence of shoulder pain in the general population; a systematic review. Scand J Rheumatol. (2004) ; 33: (2): 73-81. |
[2] | van der Windt DA, Koes BW, Boeke AJ, Devillé W, De Jong BA, Bouter LM. Shoulder disorders in general practice: Prognostic indicators of outcome. Br J Gen Pract. (1996) ; 46: (410): 519-23. |
[3] | Ottenheijm RP, Cals JW, Winkens B, Weijers RE, de Bie RA, Dinant GJ. Ultrasound imaging to tailor the treatment of acute shoulder pain: A randomised controlled trial in general practice. BMJ Open. (2016) ; 6: (11): e011048. |
[4] | Kuijpers T, van Tulder MW, van der Heijden GJ, Bouter LM, van der Windt DA. Costs of shoulder pain in primary care consulters: A prospective cohort study in The Netherlands. BMC Musculoskelet Disord. (2006) ; 7: : 83. |
[5] | Virta L, Joranger P, Brox JI, Eriksson R. Costs of shoulder pain and resource use in primary health care: A cost-of-illness study in Sweden. BMC Musculoskeletal Disorders. (2012) ; 13: (1): 17. |
[6] | NICE. Shoulder pain (Clinical Knowledge Summaries) [internet] (2017) [cited 2022 Jan 17]. Available from: https://www.nice.org.uk/accessibility. |
[7] | American Academy of Orthopaedic Surgeons. Management of Rotator Cuff Injuries – Evidence-Based Clinical Practice Guideline. (2019) [cited 2022, Jan 17]. Available from: https://aaos.org/globalassets/quality-and-practice-resources/rotator-cuff/management-of-rotator-cuff-injuries-2.pdf. |
[8] | Whitehurst DG, Bryan S, Lewis M, Hill J, Hay EM. Exploring the cost-utility of stratified primary care management for low back pain compared with current best practice within risk-defined subgroups. Ann Rheum Dis. (2012) ; 71: (11): 1796-802. |
[9] | Henschkem N, Ostelo RWJG, Terwee CB, van der Windt DAWM. Identifying generic predictors of outcome in patients presenting to primary care with nonspinal musculoskeletal pain. Arthritis Care & Research. (2012) ; 64: (8). |
[10] | Wong WK, Li MY, Yung PS, Leong HT. The effect of psychological factors on pain, function and quality of life in patients with rotator cuff tendinopathy: A systematic review. Musculoskelet Sci Pract. (2020) ; 47: : 102173. |
[11] | Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol Bull. (2007) ; 133: (4): 581-624. |
[12] | Mallows A, Debenham J, Walker T, Littlewood C. Association of psychological variables and outcome in tendinopathy: A systematic review. Br J Sports Med. (2017) ; 51: (9): 743-8. |
[13] | De Baets L, Matheve T, Meeus M, Struyf F, Timmermans A. The influence of cognitions, emotions and behavioral factors on treatment outcomes in musculoskeletal shoulder pain: A systematic review. Clin Rehabil. (2019) ; 33: (6): 980-91. |
[14] | Reeves B. The natural history of the frozen shoulder syndrome. Scand J Rheumatol. (1975) ; 4: (4): 193-6. |
[15] | Federation of medical specialists. Guidelines database [internet] (2013) [cited 2022 Jan 17]. Available from: https://richtlijnendatabase.nl. |
[16] | van Engelen EISM, Jungen MJH. Uitgebreide toelichting van het meetinstrument: Shoulder Pain and Disability Index (SPADI) (2014) [cited 2022, Jan 17]. Available from: https://meetinstrumentenzorg.nl/wp-content/uploads/instrumenten/SPADI-form.pdf. |
[17] | Thoomes-de Graaf M, Scholten-Peeters GGM, van Duijn E, Karel Y, Koes BW, Verhagen AP. The dutch shoulder pain and disability index (SPADI): A reliability and validation study. Quality of Life Research. (2015) ; 26: (6): 1515-9. |
[18] | Breckenridge JD, McAuley JH. Shoulder pain and disability index (SPADI). Journal of Physiotherapy. (2011) ; 57: (3): 197. |
[19] | Thoomes-de Graaf M, Scholten-Peeters W, Duijn E, et al. The responsiveness and interpretability of the shoulder pain and disability index. J Orthop Sports Phys Ther. (2017) ; 47: (4): 278-86. |
[20] | Djukanovic I, Carlsson J, Årestedt K. Is the hospital anxiety and depression scale (HADS) a valid measure in a general population 65–80 years old? A psychometric evaluation study. Health Qual Life Outcomes. (2017) ; 15: (1): 193. |
[21] | Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale. An updated literature review. J Psychosom Res. (2002) ; 52: (2): 69-77. |
[22] | Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: Development and validation. Psychological Assessment. (1995) ; 7: (4): 524-32. |
[23] | Sullivan MJL. The Pain Catastrophizing Scale User Manual. (2009) : 1-36. |
[24] | Roach KE, Budiman-Mak E, Songsiridej N, Lertratanakul Y. Development of a shoulder pain and disability index. Arthritis Care Res. (1991) ; 4: (4): 143-9. |
[25] | Fernandes L, Storheim K, Lochting I, Grotle M. Cross-cultural adaptation and validation of the Norwegian pain catastrophizing scale in patients with low back pain. BMC Musculoskeletal Disorders. (2012) ; 13: (1): 111. |
[26] | Bell ML, Fairclough DL, Fiero MH, Butow PN. Handling missing items in the Hospital Anxiety and Depression Scale (HADS): A simulation study. BMC Res Notes. (2016) ; 9: (1): 479. |
[27] | Pinheiro MB, Ferreira ML, Refshauge K, et al. Symptoms of depression as a prognostic factor for low back pain: A systematic review. Spine J. (2016) ; 16: (1): 105-16. |
[28] | Doyle C, Lennox L, Bell D. A systematic review of evidence on the links between patient experience and clinical safety and effectiveness. BMJ Open. (2013) ; 3: : e001570. |
[29] | Mallen CD, Peat G, Thomas E, Dunn KM, Croft PR. Prognostic factors for musculoskeletal pain in primary care: A systematic review. Br J Gen Pract. (2007) ; 57: (541): 655-61. |
[30] | Mallen CD, Thomas E, Belcher J, Rathod T, Croft P, Peat G. Point-of-care prognosis for common musculoskeletal pain in older adults. JAMA Internal Medicine. (2013) ; 173: (12): 1119-25. |
[31] | Campbell P, Hill JC, Protheroe J, et al. Keele Aches and Pains Study protocol: Validity, acceptability, and feasibility of the Keele STarT MSK tool for subgrouping musculoskeletal patients in primary care. J Pain Res. (2016) ; 9: : 807-18. |
Appendices
Supplementary data
Supplementary Table 1
Orthopaedic clinics’ and response subgroups’ baseline characteristics
| Variables | Orthopaedic clinic ( | Response subgroups ( | |||
|---|---|---|---|---|---|
| Outreach ( | Outpatient ( | Full-responders ( | Partial-responders ( | Non-responders ( | |
| Demographic | |||||
| Females, | 47 (48.0%) | 40 (43.5%) | 47 (49.5%) | 21 (46.7%) | 19 (38.0%) |
| Age, years (SD) | 55.8 (12.1) | 58.3 (14.3) | 60.1 (11.6) | 58.4 (12.2) | 49.9 (14.5) |
| Dominant side affected, | 57 (59.4%) | 51 (56.7%) | 55 (59.1%) | 19 (43.2%) | 34 (69.4%) |
| Primary outcome | |||||
| SPADI, mean (SD) | 56.4 (20.3) | 64.6 (21.7) | 60.5 (20.7) | 60.2 (20.7) | 59.7 (23.5) |
| Psychological disorder | |||||
| PCS, mean (SD) | 16.4 (10.5) | 22.0 (11.5) | 17.7 (10.16) | 19.1 (12.7) | 21.9 (11.9) |
| HADS, mean (SD) | 10.2 (6.8) | 10.3 (7.2) | 9.7 (6.54) | 9.3 (6.1) | 12.0 (8.2) |
| Shoulder disorder, | |||||
| SAPS Glenohumeral disorder AC disorder Functional disorder Other disorder | 66 (67.3%) 18 (18.4%) 22 (22.4%) 14 (14.3%) 8 (8.2%) | 57 (62.0%) 11 (12.0%) 10 (10.9%) | 64 (67.4%) 15 (15.8%) 17 (17.9%) 10 (10.5%) 9 (9.5%) | 31 (68.9%) 7 (15.6%) 9 (20.0%) 6 (13.3%) 5 (11.1%) | 28 (56.0%) 7 (14.0%) 6 (12.0%) 7 (14.0%) 7 (14.0%) |
| Clinical | |||||
| Duration of shoulder pain, | |||||
| 0–6 months | 49 (53.3%) | 42 (50.6%) | 46 (51.7%) | 18 (42.9%) | 27 (61.4%) |
| | 43 (46.7%) | 41 (49.4%) | 43 (48.3%) | 24 (57.1%) | 17 (38.6%) |
| Missing | 6 | 9 | 6 | 3 | 6 |
| Acute onset, | 21 (21.4%) | 35 (38.0%) | 27 (79.4%) | 14 (82.4%) | 15 (88.2%) |
| Missing | 67 | 55 | 61 | 28 | 33 |
| Previous episode, | 22 (22.4%) | 8 (8.7%) | 15 (21.7%) | 9 (36.0%) | 6 (16.7%) |
| Missing | 9 | 51 | 26 | 20 | 14 |
| Previously received treatment, | |||||
| Physiotherapy | 65 (66.3%) | 36 (39.1%) | 29 (34.5%) | 17 (47.2%) | 27 (69.2%) |
| Missing | 1 | 30 | 11 | 9 | 11 |
| Corticosteroid injection | 25 (25.5%) | 27 (29.3) | 22 (33.3%) | 17 (48.6%) | 13 (34.2%) |
| Missing | 9 | 42 | 29 | 10 | 12 |
| Surgery | 0 (0.0%) | 7 (7.6%) | 2 (2.1%) | 3 (6.7%) | 2 (4.0%) |
SPADI: Shoulder Pain and Disability Index total score (score 0–100); PCS: Pain Catastrophizing Scale (score 0–52); HADS: Hospital Anxiety and Depression Scale (score 0–42); SAPS: subacromial pain syndrome; AC: acromioclavicular;

