
Abstract
The extent to which the heterogeneity of gait and balance problems in PD may be explained by genetic variation is unknown. Variants in the glucocerebrosidase (GBA) gene are the strongest known genetic risk factor for PD and are associated with greater motor and cognitive severity. However, the impact of GBA variants on comprehensive measures of gait and balance and their relationship to cognition remains unknown. We aimed to determine differences in gait and balance impairments in those with and without GBA variants (mutation carriers and E326K polymorphism) and explore direct and indirect effects of GBA status on gait, balance, and cognition. 332 participants, 43 of whom had GBA variants, were recruited. Participants completed a comprehensive, objective assessment of gait and standing balance using body-worn inertial sensors. Group differences in gait and balance between PD with and without GBA variants were assessed with linear regression, adjusting for age, gender, clinical testing site, disease duration, and apolipoprotein E (APOE) ɛ4 status. Structural equation modeling (SEM) explored direct relationships between GBA status and gait and balance and indirect relationships between GBA status and gait and balance via cognition. The GBA variant group had more impaired gait (pace and variability) and balance (sway area/jerk and sway velocity), than the non-GBA variant group. SEM demonstrated cognition as a mediator of GBA status on gait and balance. The close relationships among GBA, gait/balance, and cognition suggest potential for novel therapeutics to target the GBA pathway and/or cognition to improve mobility in PD GBA variants.
Similar content being viewed by others
Introduction
Gait and balance difficulties are cardinal features of Parkinson’s disease (PD), yet these mobility deficits vary greatly across patients. The extent to which the heterogeneity of gait and balance problems in PD may be explained by genetic variation is unknown. The strongest known genetic risk factor for PD is variation within the glucocerebrosidase (GBA) gene, which includes the E326K polymorphism and over 200 “pathogenic” mutations responsible for Gaucher disease, although not all variants are reported in PD1. Together these variants are present in 7–10% of sporadic PD cases2. It is hypothesized that GBA mutations result in reduced GCase enzyme activity, which leads to compromised cellular functioning, including increased levels of α-synuclein and Lewy body formation3,4.
GBA variants are associated with more rapid symptom progression5,6, including younger disease onset, faster disease progression, and greater motor severity7,8. Furthermore, PD patients who carry GBA variants have demonstrated a faster decline in the postural instability and gait difficulty (PIGD) phenotype, as well as poorer dual-task gait speed performance5,9,10,11. However, it is critical to understand the specific gait and balance impairments in people with GBA-related PD to provide tailored targets for therapeutics and rehabilitation. To date, there have been no comprehensive comparisons of objective gait and balance measures between PD patients with and without GBA variants.
In addition to gait and balance deficits, GBA variants are associated with increased severity of non-motor symptoms, including impaired cognitive function6,12. A higher incidence of cognitive impairment and dementia is evident in patients with GBA variants; in particular, these patients have greater impairment in executive function and visuospatial cognitive domains6,12. Furthermore, GBA mutations are an independent risk factor for the development of cognitive impairment in PD as well as increased risk of developing dementia with Lewy bodies (DLB)13,14. Gait and balance require cognitive input across a number of domains, and those with poorer cognition demonstrate greater deficits in gait and balance measures. Furthermore, a longitudinal relationship has been demonstrated with measures of gait able to predict cognitive decline over three years15,16,17,18,19. Due to the known relationship between cognition with gait and balance measures, impairments in gait and balance may be exacerbated in those with GBA variants due to the nature of cognitive deficits in this cohort. If poor cognitive function impacts gait and balance function, therapies targeting cognitive function may provide novel treatment routes for this cohort.
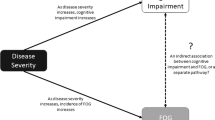
The primary aim of this paper was to assess differences in comprehensive, objective measures of gait and balance in people with PD with and without GBA variants. A secondary aim was to explore the direct and indirect relationships between GBA, cognition, and gait and balance. We hypothesized that people with PD and GBA variants would demonstrate poorer gait and balance than those without variants. Further, we hypothesized that GBA variants would lead to gait and balance impairments, both directly and indirectly via cognition; this hypothesis is outlined in Fig. 1.

Two pathways are likely to contribute; ① PD with the GBA variant (GBA+) have poorer cognitive function as previously established5 and ② GBA+ have poorer gait and balance, ③ poorer cognitive function impacts gait and balance function as previously established15,17,18. We hypothesize that ④ in GBA+ poorer cognitive function indirectly exacerbates gait and balance impairments via cognition.
Results
Characteristics of participants
A total of 332 participants with idiopathic PD were recruited to the study from the three clinical testing sites. Participant demographic and clinical characteristics are described in Table 1. Of these, 43 participants (13%) carried a pathogenic GBA mutation (n = 21) or the E326K polymorphism (n = 22; see Supplementary Table 1 for specific variants observed1). No unclassified nonsense or frameshift mutations were observed in the cohort, and the only other nonsynonymous substitution seen was the T369M polymorphism. While T369M is a risk factor for PD20, data from our group suggest that it is not associated with more severe motor or cognitive deficits among PD patients21. Therefore, the T369M carriers (n = 9) identified in this study were not included in the GBA variant group but were not excluded from analysis. Overall, those with GBA variants were more likely to have a higher H&Y score (p = 0.028) than those without GBA variants, but there was no difference for MDS-UPDRS III or disease duration. Those with GBA variants were more likely to have MCI or PDD (p < 0.001) than those without GBA variants, but there were no other clinical or demographic differences. Within the GBA group, those with the E326K polymorphism were older than mutation carriers (mutation: 62.2 ± 9.6 years; E326K polymorphism: 69.5 ± 8.3 years, p = 0.01), but there were no other demographic or clinical differences observed between the GBA subgroups (Supplementary Table 2).
Comparison of gait and balance measures in PD with and without GBA variants
Participants with GBA variants had slower gait pace (β −0.38, p = 0.008) and increased gait variability (β 0.53, p = 0.002) compared to those without, but there was no difference in gait rhythm or trunk movement during gait between groups, after adjusting for covariates (age, gender, disease duration, apolipoprotein E (APOE) ɛ4 status, and clinical testing site). Gait and balance outcomes for those with and without GBA variants are compared in Table 2. None of the gait domains differed between those with the GBA mutations compared to E326K polymorphism (Supplementary Table 2). Individual gait and balance measures that informed domains are shown in Supplementary Table 3.
Participants with GBA variants demonstrated greater postural sway area/jerk (β 0.50, p = 0.011) and greater sway velocity (β 0.28, p = 0.041) than those without variants, when comparing domains of balance, after adjusting for covariates. None of the balance domains differed between GBA variant subgroups; participants with GBA mutations had similar balance to participants with the E326K polymorphism (Supplementary Table 2). Individual measures that informed balance domains are shown in Supplementary Table 3.
Additional analysis identified that when controlling for cognitive group, the pace & turning domain and the sway velocity domains were no longer significantly different between groups. However, gait variability and sway area & Jerk remained significantly different (Supplementary Table 4).
Cognition function in PD with and without GBA variants
Participants with GBA variants had a significantly poorer MoCA score (β −0.66, p = 0.004), worse attention/executive function (TMT B-A; β 0.39, p = 0.023), worse visuospatial function (JoLO; β −0.41, p = 0.012), poorer immediate recall (HVLT-R total recall; β −0.51, p = 0.002) and poorer semantic fluency (Animals; β −0.40, p = 0.049) compared to those without the GBA variant, when adjusting for age, gender, years of education, disease duration, data collection clinical testing site, and APOE ɛ4 status. Differences in cognitive performance between groups with versus without GBA variants are shown in Table 3. There was no difference in cognitive performance between the GBA variant groups (Supplementary Table 2).
Direct and indirect associations of GBA variants with gait, balance, and cognition
Significant, direct relationships between GBA and cognition (relationship 1) and between cognition and gait (relationship 3) were found for all 4 domains of gait and balance (see Fig. 1). The SEM for the four significant domains of gait and balance are shown in Fig. 2. Standardized regression weights demonstrate the relative strength of associations between the variables in the model. All models were a good-excellent fit as specified by the criteria above. All significant differences in cognitive performance between groups were retained in the latent variable except for the JoLO, which did not meet the loading variable requirement.

SEM for A pace and turning, B gait variability, C sway area and Jerk and D sway Velocity. Solid arrows indicate direct pathways, dashed arrows indicate indirect pathways. * symbolizes significant standardized β value, TE total effect. Cognition is a latent variable including attention/executive function, global cognition, memory, and language.
The pace/turning domain of gait showed no direct relationship with GBA (β −0.09), but there was a significant indirect relationship between GBA status and pace/turning via cognition (β −0.21; Fig. 2A). The variability domain of gait showed a significant, direct relationship between GBA and gait variability (β 0.46) as well as a significant, indirect relationship between GBA and gait variability via cognition (β 0.09; Fig. 2B).
For the sway area/jerk domain of balance, SEM demonstrated a significant direct relationship between GBA and sway area/jerk (β 0.38) and a significant indirect relationship between GBA and sway area/jerk via cognition (β 0.12; Fig. 2C). For the sway velocity domain, there was no direct relationship between GBA and sway velocity (β 0.17) but there was a significant indirect relationship between GBA and sway velocity via cognition (β 0.10; Fig. 2D).
Discussion
This study compared comprehensive gait, balance, and cognitive measures in people with and without GBA variants in a well-characterized, multi-site PD cohort. In addition, we used SEM to examine the causal relationships among gait/balance and cognition in GBA-related PD to determine the extent to which cognitive impairment impacts gait and balance deficits. In our cohort, those with GBA variants demonstrated greater impairments in the pace/turning and variability domains of gait and the sway area/jerk and sway velocity domains of balance. Furthermore, our SEM indicated both direct associations between GBA status and gait variability and postural sway area/jerk as well as widespread, indirect associations for GBA on gait and balance via cognition as a mediator. Although future validation work in independent cohorts is needed, our findings suggest novel avenues for treating mobility impairments in PD.
Previous work demonstrates that GBA carriers have greater motor symptom severity and are more likely to present with the PIGD motor phenotype5,9. We identified impairments in specific domains of gait (pace/turning and variability) and balance (sway area/jerk and velocity) in GBA carriers compared to those without. In contrast, other domains of gait (rhythm and trunk movement) and balance (sway frequency) did not differ significantly between GBA groups. This finding is consistent with the idea of multiple mechanisms underlying the control of different gait and balance domains, as evidenced by inconsistent effects of dopaminergic replacement therapy22,23. Our findings support previous evidence indicating the impacts of GBA variants on mobility and extend prior work by identifying specific gait and balance domains that are more affected in those with GBA variants, even when accounting for disease duration.
GBA carriers with PD have greater accumulation of α-synuclein due to the reduced expression of the GCase enzyme2,13. As poorer gait and balance have been noted in mouse models overexpressing α-synuclein24, this may indicate that α-synuclein accumulation in non-dopaminergic pathways underlies the gait and balance deficits shown in GBA carriers25. Importantly, reduced GCase activity occurs not only in GBA-related PD, but also idiopathic PD26, suggesting a novel treatment target for mobility deficits in PD.
Gait and balance dysfunction are associated with cognitive dysfunction in the elderly, with specific associations for cognitive domains related to distinct measures of gait and balance18,27. We, therefore, hypothesized that cognition would impact gait and balance in our PD cohort and that the impact of cognitive impairment would be exacerbated in GBA carriers. Our SEM confirmed that cognitive impairment was significantly associated with specific gait and balance deficits15,17 and that GBA status was significantly associated with poorer cognition6.
Cognitive status mediated an indirect relationship for all gait and balance domains that were worse in those with GBA variants compared to those without. No direct effect of GBA was found for the pace/turning domains of gait or the sway velocity domain of balance, but an indirect effect via cognition was found for both. In contrast, gait variability and sway area showed both a direct effect of GBA as well as an indirect effect via cognition. This indicates that cognition, in addition to other GBA-related factors, likely contributes to gait and balance impairments in people with PD.
Our results support the notion that GBA variants impact gait and balance deficits in various ways. First, measures such as gait speed and turning speed are associated with cognition in aging and PD populations15,16, indicating potential dysfunction in cortical areas associated with cognition. Second, measures such as gait variability and sway area may be impacted by the effects of GBA variants on other regions or circuits that are less dependent on cognitive control, such as subcortical areas18. Further work is needed to inform this hypothesis, including replication in an independent cohort, imaging studies, and longitudinal analysis to determine the trajectory of mobility and cognitive impairments in GBA variants.
The impact of GBA variants occurs on a continuum, where severe pathogenic mutations are known to impact motor and cognitive signs to a greater extent than mild mutations28,29. The severity of specific variants in our cohort is summarized in Supplementary Table 1, with roughly equal numbers of mild and severe mutations. However, we found no differences in gait, balance, or cognitive characteristics between those with mild versus severe mutations (Supplementary Table 5). These findings are surprising considering the known continuum of mutation severity on symptoms. Heterogeneity may have impacted our findings due to the small numbers in our cohort, and further work should explore the impact of mutation severity on gait, balance, and cognition.
Our findings are consistent with the idea that GBA status is associated with specific gait and balance deficits both directly and indirectly, via cognitive impairments. Although our work needs to be replicated in future cohorts, it supports a precision-medicine approach for both rehabilitative and pharmacological interventions30. In the future, rapid and cost-effective methods will emerge to identify people with PD who have GBA variants, which could enable referral to physical therapy to address balance and gait impairments even before their earliest presentation31. Exercise programs targeting cognitive function as well as balance and gait at an early disease stage may improve mobility and prolong the time to first fall30. Furthermore, targeted medications to increase GCase enzyme activity may improve cognition and mobility13,32. A recent study assessing efficacy for ambroxol therapy to increase GCase activity demonstrated that the treatment was safe, well-tolerated, and able to penetrate the blood-brain barrier33, but the impact on mobility is yet to be assessed. Furthermore, treadmill training in mice expressing human α-synuclein improved gait (specifically, speed and stride length) and balance, demonstrating the importance of exercise, in addition to dopaminergic medications, to target mobility impairments24.
This study has several limitations. First, our cohort of GBA carriers was relatively small compared to those without GBA. Recruitment of GBA carriers is challenging, as they account for only 7–10% of patients with PD. We also pooled patients with pathogenic mutations and the E326K polymorphism for this analysis. Our results and other studies5,6 demonstrate similarities in motor and cognitive functions in these groups, providing justification for this grouping. Second, it is possible that some people with PD in our cohort were unable to complete gait and balance assessments; for example, if they were unable to stand unsupported for 30 seconds. Therefore, PD participants with GBA variants included in this study may not capture the most severely affected participants, which may bias results. Third, we did not control for multiple comparisons in our analysis. This decision was made due to the exploratory nature of our study, the first of its kind in this rare genetic cohort with well characterized gait, balance, and cognition. We sought to limit the impact of multiple comparisons by using independent domains of gait and balance rather than individual characteristics34, however, our exploratory results should be treated with caution until they are replicated in independent cohorts. Fourth, we used disease duration rather than disease severity in our statistical modeling as we sought to determine how cognition impacts gait and balance impairment, irrespective of disease severity. Fifth, our cohort was also enriched for PD APOE ε4 carriers. This may have impacted our findings, but separate analyses demonstrated that differences in gait and balance characteristics between those with and without the GBA variant remained even when APOE ε4 carriers were removed. Finally, our analysis was cross-sectional, but longitudinal studies of gait and balance in GBA cohorts could inform our understanding of the physiological mechanisms for how GBA variants affect gait and balance.
This study demonstrated that among people with PD, specific domains of gait (pace/turning and variability) and balance (sway area/jerk and velocity) were more affected in those carrying GBA variants compared to those without. In addition, cognitive impairments impacted the relationships between GBA and gait and balance. These findings have implications for personalized medicine to improve mobility among people with PD.
Methods
Participants
Participants with PD were recruited from the Pacific Udall Center (PUC) Clinical Core, comprised of three clinical testing sites: Oregon Health and Science University/Portland VA Medical Center, Portland, OR; University of Washington/VA Puget Sound Health Care System, Seattle, WA; and Stanford University, Palo Alto, CA. All subjects provided informed written consent approved by the joint Institutional Review Boards at Oregon Health & Science University, the VA Portland Health Care System, University of Washington, VA Puget Sound Health Care System, and Stanford University, (Stanford University, IRB- 37967). Participants were included in the study if they: (i) met the United Kingdom Parkinson’s Disease Society Brain Bank (UKBB) clinical diagnostic criteria for PD, with the modification that having more than one affected relative was not an exclusion criterion35, (ii) had no history of other neurological disorders that affected cognition, e.g., large-vessel stroke or severe traumatic brain injury, and iii) were able to stand unsupported for a minimum of 30 seconds. Participants who were taking medication were tested ‘on’ PD medication for all assessments. Because the overall goal of this study was to examine balance and gait measures in genetic subgroups of PD, the study cohort was enriched in both GBA variants and APOE ε4 carriers by selectively inviting every eligible GBA and APOE ε4 carrier in the PUC Clinical Core to participate in the study. APOE ε4 carriers have a greater risk of cognitive decline and dementia36 and therefore this genetic type has been controlled for in statistical analyses.
Demographic and clinical characteristics
Age, gender, height, and years of education were recorded for all participants. PD motor severity was assessed using the Movement Disorders Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS III)37 and the modified Hoehn and Yahr scale (H&Y)38. Daily dopamine replacement therapy dose was calculated using the levodopa equivalent daily dose score (LEDD)39. Each participant was assigned a diagnosis of no cognitive impairment (NCI), mild cognitive impairment (MCI), or Parkinson’s disease dementia (PDD). The diagnosis was established at biweekly diagnostic consensus conference between all clinical testing sites in accordance with specific criteria40.
Genotyping
The GBA group within this study included both low frequency mutations that cause Gaucher disease and the E326K polymorphism which occurs at a frequency >1% in the population. Hereafter, they will be referred to together as “GBA variants”. Genomic DNA was extracted from peripheral blood or saliva samples using standard procedures. The entire GBA coding region was screened in every participant using Sanger sequencing to capture all known pathogenic mutations (defined as those reported in patients with Gaucher disease1,41), the E326K polymorphism (rs2230288), and other potentially relevant variants. All sequencing was performed at a single laboratory at the PUC site in Seattle using methods previously described6.
By design, our cohort was enriched for APOE ε4 carriers. APOE ε4 status was determined by genotyping the APOE single nucleotide polymorphisms rs429358 and rs7412 (which define the ε2, ε3, and ε4 alleles), using TaqMan Assays as previously described42.
Gait and balance assessment
Participants performed a standardized instrumented gait and balance assessment wearing six inertial sensors (Opals by APDM Wearable Technology of ERT, Portland, OR). Inertial sensors were attached with elastic Velcro straps to the wrists and feet, as well as on the sternum and fifth lumbar vertebrae. To assess gait, participants were asked to walk at their normal pace back and forth on a straight 7 m walkway in a quiet hallway for 2 min. To assess balance, participants stood quietly, looking an image straight ahead for 60 seconds with their arms at their sides. At the start of the gait and balance trials, a template was used to achieve consistent foot placement (10 cm between left and right heel and 30° outward rotation of the feet).
Gait and balance measures
A total of 15 gait and 13 balance measures were analyzed from the inertial sensors. To reduce variables for statistical analysis but maintain a wide representation of measures, gait and balance measures were allocated to independent domains based on our previous model18. The 4 domains of gait were pace/turning, rhythm, variability, and trunk movement. The four domains of balance were sway area/jerk, sway velocity, sway frequency anteroposterior (AP), and sway frequency medio-lateral (ML).
Cognitive assessment
Study visits included a comprehensive assessment of cognition40. To assess different domains of cognition, the MoCA was selected to assess global cognition, the Trail Making Test (TMT) B-A and the letter number sequencing test (LNST) were selected to assess executive function, the Hopkins Verbal Learning Test-Revised (HVLT-R) Total recall and Delayed recall were selected to assess memory (immediate and delayed recall respectively). The Judgment of Line Orientation (JoLO) test assessed visuospatial function and language was assessed via semantic fluency (Animals).
Data analysis
Distributions of all metrics were inspected using boxplots, histograms, and normal quantile plots. Variables that were positively skewed were transformed (natural log 10) prior to further analysis to better meet modeling assumptions. Domain scores were calculated for the 8 gait and balance domains, with groupings based on a previous principal component analysis18. Domain scores were calculated by standardizing the component measures (using the value minus the mean, divided by the standard deviation), multiplying by −1 to reverse scaling if needed for consistency, and taking the average (no weighting was used). Demographic and clinical characteristics were compared between PD, with and without GBA variants, using Student’s t-tests with unequal variances and χ2 tests. To ensure GBA subtypes (GBA mutation and E326K polymorphism) could be grouped, differences between GBA variant subtypes for demographic, clinical, gait, balance, and cognitive data were compared using independent Student’s t-tests.
Comparing gait and balance in GBA and non-GBA related PD
We compared group mean differences in individual gait and balance domain scores between PD with and without GBA variants using generalized linear models (GLM) and applying a robust estimator with (1) an indicator variable for GBA variants and (2) covariate variables. Covariates included age, gender, clinical testing site, and APOE ɛ4 status (due to high percentage of APOE ɛ4 carriers within our sample). In addition, disease duration was included as a covariate as a proxy for disease severity, as measures such the MDS-UPDRS III and H&Y directly relate to our primary outcome measure of gait and balance. Additional analysis was performed controlling for cognitive group (NCI, MCI, or PDD) to decipher whether results were driven by GBA variant status or cognitive status.
This is study is unique in having well-characterized gait, balance, and cognition measures in a cohort enriched for rare GBA variants. Due to the exploratory nature of this work, a p-value <0.05 in the adjusted model was considered evidence of association for the next stage of analysis. Gait and balance domains significantly related to the GBA variant were taken forward to the SEM analysis.
Exploring the direct and indirect relationships between GBA, cognition, and gait and balance
To explore the direct and indirect effects of cognition on gait and balance, we first sought to identify differences in cognition between those with and without GBA variants. Differences were assessed using a GLM with a robust estimator with the indicator variable for GBA variants and adjusting for age, gender, disease duration, clinical testing site, APOE ɛ4 status, and years of education. A p-value below 0.05 in the adjusted model was considered evidence of association with those related to the GBA variant taken forward to the SEM analysis.
To explore the relationship between GBA variants, cognition, and gait and balance impairments, SEM was used to estimate direct and indirect relationships presented in Fig. 1. We sought to explore direct relationships between GBA and cognition (Relationship 1, Fig. 1), between GBA and gait/balance (Relationship 2, Fig. 1) and between cognition and gait/balance (Relationship 3, Fig. 1). We then sought to explore the indirect relationship between GBA and gait/balance via cognition (Relationship 4, Fig. 1).
Models were examined only for the balance and gait domains that were significantly different between genetic groups as determined in the first stage of analysis. Each model included GBA group and a single domain of gait or balance, with cognition entered as a latent variable (using standardized scores for each cognitive test). Cognitive tests that differed between GBA and non-GBA groups at a significance threshold of p < 0.05 were entered onto the latent variable. Second, latent variable loadings were examined to determine if any cognitive tests had a poor variable loading (variable loading <0.60) as these were then removed from the model. Maximum likelihood methods were used to estimate parameters using all available data. The goodness of fit were assessed using 1) X2 test for the model versus a saturated model did not reject the null at p < 0.05, 2) comparative fit index (CFI) > 0.90, 3) root mean squared error of approximation (RMSEA) at <0.08, 4) Akaike’s information criterion and Bayesian information criterion lower than for other formulations with the same variables43,44. SPSS version 24 and Stata version 15 were used for data analysis.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Beutler, E., Gelbart, T. & Scott, C. R. Hematologically important mutations: Gaucher disease. Blood Cells Mol. Dis. 35, 355–364 (2005).
Sardi, S. P., Cheng, S. H. & Shihabuddin, L. S. Gaucher-related synucleinopathies: The examination of sporadic neurodegeneration from a rare (disease) angle. Prog. Neurobiol. 125, 47–62 (2015).
Shihabuddin, L. S., Brundin, P., Greenamyre, J. T., Stephenson, D. & Sardi, S. P. New frontiers in Parkinson’s disease: From genetics to the clinic. J. Neurosci. 38, 9375–9382 (2018).
Sardi, S. P. et al. CNS expression of glucocerebrosidase corrects alpha-synuclein pathology and memory in a mouse model of Gaucher-related synucleinopathy. Proc. Natl Acad. Sci. USA 108, 12101–12106 (2011).
Davis, M. Y. et al. Association of GBA mutations and the E326K polymorphism with motor and cognitive progression in Parkinson disease. JAMA Neurol. 73, 1217–1224 (2016).
Mata, I. F. et al. GBA Variants are associated with a distinct pattern of cognitive deficits in Parkinson’s disease. Mov. Disord. 31, 95–102 (2016).
Winder-Rhodes, S. E. et al. Glucocerebrosidase mutations influence the natural history of Parkinson’s disease in a community-based incident cohort. Brain 136, 392–399 (2013).
Brockmann, K. et al. GBA-associated Parkinson’s disease: Reduced survival and more rapid progression in a prospective longitudinal study. Mov. Disord. 30, 407–411 (2015).
Malek, N. et al. Features of GBA-associated Parkinson's disease at presentation in the UK Tracking Parkinson's study. J. Neurol. Neurosurg. Psychiatry 89, 702–709 (2018).
Srulijes, K. et al. Dual-task performance in GBA Parkinson’s disease. Parkinsons Dis. 2017, 8582740 (2017).
Stoker, T. B. et al. Impact of GBA1 variants on long-term clinical progression and mortality in incident Parkinson’s disease. J. Neurol., Neurosurg. Psychiatry https://doi.org/10.1136/jnnp-2020-322857 (2020).
Neumann, J. et al. Glucocerebrosidase mutations in clinical and pathologically proven Parkinson’s disease. Brain 132, 1783–1794 (2009).
Blandini, F. et al. Glucocerebrosidase mutations and synucleinopathies: Toward a model of precision medicine. Mov. Disord. 34, 9–21 (2019).
Tsuang, D. et al. GBA mutations increase risk for Lewy body disease with and without Alzheimer disease pathology. Neurology 79, 1944–1950 (2012).
Morris, R., Lord, S., Bunce, J., Burn, D. & Rochester, L. Gait and cognition: Mapping the global and discrete relationships in ageing and neurodegenerative disease. Neurosci. Biobehav Rev. 64, 326–345 (2016).
Yogev-Seligmann, G., Hausdorff, J. M. & Giladi, N. The role of executive function and attention in gait. Mov. Disord. 23, 329–342 (2008).
Kelly, V. E. et al. Association of cognitive domains with postural instability/gait disturbance in Parkinson’s disease. Parkinsonism Relat. Disord. 21, 692–697 (2015).
Morris, R. et al. Cognitive associations with comprehensive gait and balance measures in Parkinson’s disease. Parkinsonism Relat. Disord. 69, 104–110 (2019).
Morris, R. et al. Gait rather than cognition predicts decline in specific cognitive domains in early Parkinson’s disease. J. Gerontology: Ser. A. 72, 1656–1662 (2017).
Mallett, V. et al. GBA p.T369M substitution in Parkinson disease: Polymorphism or association? A meta-analysis. Neurol. Genet. 2, e104 (2016).
Julius, A. et al. Association of the GBA T369M polymorphism with motor and cognitive symptoms in Parkinson’s disease. [abstract]. Mov. Disord. 32(suppl 2), (2017). https://www.mdsabstracts.org/abstract/association-of-the-gba-t369m-polymorphism-with-motor-and-cognitive-symptoms-in-parkinsons-disease/.
Curtze, C., Nutt, J. G., Carlson-Kuhta, P., Mancini, M. & Horak, F. B. Levodopa is a double-edged sword for balance and gait in people with Parkinson’s disease. Mov. Disord. 30, 1361–1370 (2015).
Wilson, J. et al. Gait progression over 6 years in Parkinson’s disease: Effects of age, medication, and pathology. Front. Aging Neurosci. 12, 577435–577435 (2020).
Minakaki, G. et al. Treadmill exercise intervention improves gait and postural control in alpha-synuclein mouse models without inducing cerebral autophagy. Behav. Brain Res. 363, 199–215 (2019).
Behl, T. et al. Cross-talks among GBA mutations, glucocerebrosidase, and α-synuclein in GBA-associated Parkinson’s disease and their targeted therapeutic approaches: a comprehensive review. Transl. Neurodegeneration 10, 4 (2021).
Murphy, K. E. et al. Reduced glucocerebrosidase is associated with increased α-synuclein in sporadic Parkinson’s disease. Brain 137, 834–848 (2014).
Lord, S. Independent domains of gait in older adults and associated motor and nonmotor attributes: Validation of a factor analysis approach. J. Gerontology: Ser. A. 68, 820–827 (2012).
Thaler, A. et al. Parkinson’s disease phenotype is influenced by the severity of the mutations in the GBA gene. Parkinsonism Relat. Disord. 55, 45–49 (2018).
Menozzi, E. & Schapira, A. H. V. Exploring the genotype-phenotype correlation in GBA-Parkinson disease: Clinical aspects, biomarkers, and potential modifiers. Front. Neurol 12, 694764 (2021).
Giladi, N., Mirelman, A., Thaler, A. & Orr-Urtreger, A. A personalized approach to Parkinson’s disease patients based on founder mutation analysis. Front. Neurol. 7, 71 (2016).
Straniero, L. et al. A rapid and low-cost test for screening the most common Parkinson’s disease-related GBA variants. Parkinsonism Relat. Disord. 80, 138–141 (2020).
Silveira, C. R. A. et al. Ambroxol as a novel disease-modifying treatment for Parkinson’s disease dementia: Protocol for a single-centre, randomized, double-blind, placebo-controlled trial. BMC Neurol. 19, 20 (2019).
Mullin, S. et al. Ambroxol for the treatment of patients with Parkinson disease with and without glucocerebrosidase gene mutations: A nonrandomized, noncontrolled trial. JAMA Neurol. 77, 427–434 (2020).
Lord, S., Galna, B. & Rochester, L. Moving forward on gait measurement: Toward a more refined approach. Mov. Disord. 28, 1534–1543 (2013).
Gibb, W. R. & Lees, A. J. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson’s disease. J. Neurol., Neurosurg. Psychiatry 51, 745 (1988).
Jo, S. et al. The role of APOE in cognitive trajectories and motor decline in Parkinson's disease. Sci Rep. 11, 7819 (2021).
Goetz, C. G. et al. Movement Disorder Society‐sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS‐UPDRS): Scale presentation and clinimetric testing results. Mov. Disord.: Off. J. Mov. Disord. Soc. 23, 2129–2170 (2008).
Hoehn, M. M. & Yahr, M. D. Parkinsonism: Onset, progression, and mortality. Neurology 57 (Suppl. 3), S11–S26 (2001).
Tomlinson, C. L. et al. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov. Disord. 25, 2649–2653 (2010).
Cholerton, B. A. et al. Pacific Northwest Udall Center of excellence clinical consortium: Study design and baseline cohort characteristics. J. Parkinsons Dis. 3, 205–214 (2013).
Hruska, K. S., LaMarca, M. E., Scott, C. R. & Sidransky, E. Gaucher disease: Mutation and polymorphism spectrum in the glucocerebrosidase gene (GBA). Hum. Mutat. 29, 567–583 (2008).
Mata, I. F. et al. APOE, MAPT, and SNCA genes and cognitive performance in Parkinson disease. JAMA Neurol. 71, 1405–1412 (2014).
Hu, L. T. & Bentler, P. M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling: A Multidiscip. J. 6, 1–55 (1999).
Acock, A. Discovering Structural Equation Modeling Using Stata Revised edn (Stata Press, 2013).
Acknowledgements
This work was supported by grants from the National Institutes of Health (NIH) (Pacific Udall Center; P50 NS062684) and the Department of Veterans Affairs (101 CX001702), and by infrastructure provided by the Veterans Affairs Northwest Parkinson’s Disease Research, Education, and Clinical Center. This publication was made possible with support from the Oregon Clinical and Translational Research Institute (OCTRI), grant number UL1TR002369 from the National Center for Advancing Translational Sciences (NCATS), a component of the NIH, and NIH Roadmap for Medical Research.
Author information
Authors and Affiliations
Contributions
R.M.—data acquisition, statistical data analysis, drafting of the paper. D.N.M.—data acquisition, critical revision of the paper. K.R.—statistical data analysis, critical revision of the paper. V.E.K.—data acquisition, critical revision of the paper. K.S.—data acquisition, critical revision of the paper. A.H.—data acquisition, critical revision of the paper. K.A.C.—data acquisition, critical revision of the paper. S.C.H.—data acquisition, critical revision of the paper. C.P.Z.—study concept and design, data acquisition, critical revision of the paper. K.P.—study concept and design, data acquisition, critical revision of the paper. I.M.—study concept and design, data acquisition, critical revision of the paper. K.L.E.—study concept and design, data acquisition, critical revision of the paper. J.L.—statistical data analysis, critical revision of the paper. B.C.—study concept and design, data acquisition, critical revision of the paper. T.J.M.—study concept and design, data acquisition, critical revision of the paper. J.F.Q.—study concept and design, data acquisition, critical revision of the paper. F.H.—study concept and design, data acquisition, drafting of the paper, critical revision of the paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing non-financial interests but the following competing financial interests; V.E.K. has received grant support from the report’s grants from NIH, Department of Veterans Affairs, and University of Washington and is an external advisor for projects by Sage Bionetworks. B.C. is supported by grants from the NIH. C.P.Z. is supported by grants from the NIH, Department of Veterans Affairs, and the American Parkinson Disease Association. K.P. has received grants from the NIH, clinical trial funded by Sanofi, and consulting for Allergan. K.L.E. has received grants from the NIH. T.J.M. has received grants from the NIH and Farmer Family Foundation. J.F.Q. receives compensation for conducting clinical trials for Roche, Sanofi, Abbvie, and member of DSMB for Retrophin pharmaceuticals. F.H. has a significant financial interest in APDM, a division of Clario Int, a company that may have a commercial interest in the results of this research and technology. This potential institutional and individual conflict has been reviewed and managed by OHSU. R.M., D.N.M., K.R., K.S., A.H., K.A.C., S.C.H., I.M., and J.L. have nothing to declare.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Morris, R., Martini, D.N., Ramsey, K. et al. Cognition as a mediator for gait and balance impairments in GBA-related Parkinson’s disease. npj Parkinsons Dis. 8, 78 (2022). https://doi.org/10.1038/s41531-022-00344-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41531-022-00344-5
This article is cited by
-
Impact of GBA variants on longitudinal freezing of gait progression in early Parkinson’s disease
Journal of Neurology (2023)
