
Abstract
Background
Investigators have proposed that various physical head and neck characteristics, such as neck strength and head and neck size, are associated with protection from mild traumatic brain injury (mTBI/concussion).
Objectives
To systematically review the literature and investigate potential relationships between physical head and neck characteristics and mTBI risk in athletic and military populations.
Methods
A comprehensive search of seven databases was conducted: MEDLINE, EMBASE, CINAHL, Scopus, SPORTDiscus, Cochrane Library, and Web of Science. Potential studies were systematically screened and reviewed. Studies on military and athletic cohorts were included if they assessed the relationship between physical head-neck characteristics and mTBI risk or proxy risk measures such as head impact kinematics.
Results
The systematic search yielded a total of 11,723 original records. From these, 22 studies met our inclusion criteria (10 longitudinal, 12 cross-sectional). Relevant to our PECO (Population, Exposure, Comparator, and Outcomes) question, exposures included mTBI incidence and head impact kinematics (acceleration, velocity, displacement) for impacts during sport play and training and in controlled laboratory conditions. Outcome characteristics included head and neck size (circumference, mass, length, ratios between these measures), neck strength and endurance, and rate of force development of neck muscles.
Discussion
We found mixed evidence for head and neck characteristics acting as risk factors for and protective factors against mTBI and increased susceptibility to head impacts. Head-neck strength and size variables were at times associated with protection against mTBI incidence and reduced impact kinematics (14/22 studies found one or more head-neck variable to be associated with protection); however, some studies did not find these relationships (8/22 studies found no significant associations or relationships). Interestingly, two studies found stronger and larger athletes were more at risk of sustaining high impacts during sport. Strength and size metrics may have some predictive power, but impact mitigation seems to be influenced by many other variables, such as behaviour, sex, and impact anticipation. A meta-analysis could not be performed due to heterogeneity in study design and reporting.
Conclusion
There is mixed evidence in the literature for the protective capacity of head and neck characteristics. We suggest field-based mTBI research in the future should include more dynamic anthropometric metrics, such as neck stiffness and response to perturbation. In addition, laboratory-based mTBI studies should aim to standardise design and reporting to help further uncover these complicated relationships.
Similar content being viewed by others

This article provides a comprehensive review of the relationship between physical head and neck characteristics and mild traumatic brain injury (mTBI) risk |
There was mixed evidence in the literature for the protective capacities of head and neck characteristics against mTBI |
While strength and size metrics of the head and neck may have some predictive power, head impact mitigation and mTBI incidence seem to be influenced by many other variables, such as behaviour, sex, and impact anticipation |
1 Introduction
Concussion, commonly referred to as mild traumatic brain injury (mTBI), is a prevalent injury in sport and military settings. mTBI is caused by biomechanical forces acting on the brain, either from a direct blow to the head or elsewhere on the body. The primary cause of mTBI is inertial forces, namely linear and rotational acceleration of the brain upon impact [1]. Those afflicted with mTBI experience transient loss of normal brain function. Typically, athletes recover to pre-injury function within 2–14 days [2]. However, for 10–30% of those affected, symptoms can persist for months [3]. Experience of long-term somatic, psychological, emotional, and cognitive symptoms after mTBI is known as post-concussion syndrome (PCS) [4].
Several physical characteristics of the head and neck have been researched with regard to the potential role they play in mTBI incidence. Perhaps most saliently, neck strength is hypothesised as a protective factor against mTBI, especially in a sporting context. It is thought that tensing of cervical musculature increases effective movable mass, allowing those with stronger necks to more effectively distribute potentially injurious forces from impacts as compared to those with weaker necks [5]. Rate of force development of neck muscles has also been measured by some groups [6, 7], with the idea that being able to quickly reach a high level of muscle activity is important for resisting deformation after head impacts [7]. Low neck endurance has also been proposed as a risk factor for mTBI, as it is speculated that the neck dysfunction associated with reduced levels of neck endurance may in turn reduce one’s ability to react, resist forces, and stabilise the head during impact [8]. Neck size and strength differences between sexes have been hypothesised as major underlying factors that account for the higher incidence of mTBI in females [9]. The posited relationship between head and neck characteristics and mTBI has seen groups investigate how these characteristics relate to mTBI incidence. Collins et al. [10] found a significant relationship between neck strength and size in prevention of mTBI in high school athletes, showing one-pound increments in neck strength decrease the odds of mTBI by 5%. Baker et al. [8] investigated cervical muscle endurance and did not find increases to endurance times to be significantly associated with mTBI in university athletes. Other head/neck characteristics have been related to mTBI through the head-response to impacts and perturbations, and observing how these characteristics affect the injury mechanism. Alsalaheen et al. [11] performed a perturbation experiment on recreationally active adults and discovered that men and women employed different stabilisation strategies. They hypothesise that women may rely on greater neuromuscular activation to account for lower size and strength compared to males. Dezman et al. [12] found that imbalance in neck musculature symmetry in the sagittal plane led to higher head accelerations in football/soccer heading. Mihalik et al. [5] found there was no effect of cervical strength on head acceleration in youth ice hockey head impacts. Schmidt et al. [7] investigated head impact biomechanics in American football and found that athletes with higher cervical stiffness had reduced odds of sustaining higher magnitude head impacts as compared with athletes with lower cervical stiffness, and that cervical strength and size had no significant effect in mitigation of head impact severity. Importantly, some of these characteristics are modifiable and therefore head/neck training programs may offer protection against sports-related and military mTBI.
Research into these head/neck characteristics broadly falls into two categories: studies performed in controlled laboratory settings and those in live field-based sporting situations. The former is useful as it allows experimenters to keep variables consistent across subjects, but applicability to the real world is not as obvious as in the latter. In laboratory-based settings, impacts are understandably kept to sub-concussive levels. Mechanisms of imparting these impacts on participants include football/soccer heading [12,13,14,15,16,17,18], perturbation through a weight dropped via a pulley system [6, 7, 9, 11, 19] or by an impact sled [20, 21]. Field-based settings have the advantage of being able to ethically observe the effect of head/neck characteristics on impacts over the mTBI threshold, as well as on mTBI incidence itself. These studies often record head/neck outcomes pre-season and then track mTBI incidence [8, 10, 22] or head impact kinematics (HIK) [5, 7, 23] over one or more seasons. Schmidt et al. [7] recorded both laboratory- and field-based data, which may provide insight into how measurements and outcomes relate between these two settings.
In the current literature, the role of head and neck size, neck strength (maximum strength, rate of strength development, and endurance), and neck stiffness in prevention of mTBI is inconclusive. This systematic review aims to determine the relationships between these characteristics of the head and neck with mTBI incidence and injury risk. Understanding these relationships will help elucidate major risk factors and help to inform decision making for training and prevention of mTBI.
2 Methods
This systematic review was registered with Open Science Framework (OSF) Registries on 24 November 2021 (https://osf.io/f6gv8). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed when conducting and reporting this review [24]. The PRISMA guidelines contain a checklist and flow-chart that indicate the items to include within a systematic literature review and the phases in which to conduct the review.
2.1 Search Strategy and Eligibility Criteria
A systematic search of the literature was conducted using seven databases from their date of inception up until 8 November 2021. The databases used were MEDLINE, EMBASE, CINAHL, Scopus, SPORTDiscus, Cochrane Library and Web of Science. Our review question was defined within the PECO (Population, Exposure, Comparator, and Outcomes) framework. Keywords to describe the population (athletes and military), exposure (mTBI or proxy measures of mTBI risk), and outcome (head and neck characteristics) were used in the search strategy (see Table 1). The review was not aimed at specific comparisons between concussions and interventions; so as not to limit the papers that were captured, comparator keywords were not used in the search strategy. The lower cut-off of 13 years of age allowed for studies on teenagers to be included. As 65 years is a common age of retirement, the upper cut-off ensures a full occupational cohort was captured. The final search term was formed by concatenation of the terms as such: [population terms] AND [exposure terms] AND [outcome terms]. Keywords targeted the title and abstract section of potential records in the databases. Corresponding subject headings were also included when they existed in each database (i.e., subject heading “Brain Concussion/” in Medline). We also performed a manual search of the included studies’ reference lists.
Articles were included that: (1) took a biomechanical, performance, anthropometric, clinical, or other physical recording of the head and/or neck, (2) determined the likelihood of exposure to mTBI, either through direct incidence or proxy measures of mTBI risk (increased head acceleration during perturbation/impact, reduced ability for dynamic stabilisation, etc.), (3) observed an adult military population in active duty or training, or a 13- to 65-year-old sporting population, of any sport, at any level of competition, (4) presented original data, and (5) were published in English in a peer-reviewed scientific journal. Articles were excluded if they: (1) observed mTBI occurrence in civilian vehicle accidents (as opposed to military blast-related vehicle accidents), (2) observed mTBI occurrence as a result of a fall, (3) observed populations of children (0–12 years old) and older adults (65 + years), or where results from 13- to 65-year-old participants were not reported separately to children and older adults, (4) only reported physical measures that are not directly focused on the head and/or neck (postural sway, balance, etc.), (5) only reported measures of brain and genetic structure at the micro-level (gene studies, brain protein biomarkers, imaging studies, etc.), (6) only reported on neurocognitive performance measures, (7) studied an animal population, (8) used simulations or models instead of human participants, (9) were unavailable as full-text documents, and (10) were reviews, conference abstracts, case reports, commentaries, or letters to the editor. When there was uncertainty about whether a record met the inclusion criteria, it was kept for further assessment in the full text screening stage. No studies were excluded based on quality assessment.
2.2 Quality Assessment
Studies that met the inclusion criteria were reviewed by one author (NJC), and a second author (TLAD, PS) then independently reviewed each study that met the inclusion criteria using the Mixed Methods Appraisal Tool (MMAT) [25]. The screening and quantitative non-randomized criteria were applied to each of the included studies. Conflicts between author ratings were discussed with an independent third author until an agreement was reached.
2.3 Data Extraction
Data were extracted into a spreadsheet by one author (NJC) and reviewed by all authors independently. Data extracted included study details (author, year, setting), participant characteristics (number, age, sex, sport code and level of play for athletes, branch of military for military studies), aims, methodology, exposures, outcomes, and general findings.
2.4 Data Synthesis and Analysis
A meta-analysis was planned, but during data extraction it became clear there was a large amount of heterogeneity within the included studies. As such, a statistically supported meta-analysis could not be performed. Results are therefore reported in tabular and narrative format.
3 Results
3.1 Study Selection and Quality Assessment
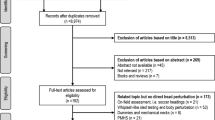
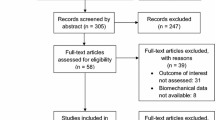
The results of the search are shown in Fig. 1. Inclusion and exclusion criteria were used on title and abstract for 11,723 records. Out of 155 articles screened in the full text stage, 22 fully met our inclusion criteria. Reasons for exclusion at this stage are given in the PRISMA flowchart (Fig. 1).

PRISMA flowchart showing the stages and number of records in the systematic review
Table 2 reports the methodological quality assessment of the included studies. All studies fulfilled both screening questions of the MMAT (“Are there clear research questions?” and “Do the collected data allow addressing the research questions?”). Twenty of the 22 included studies met all criteria of the MMAT. The average score was 4.9/5. One study [21] did not meet the criteria on item 3.3 (“Are there complete outcome data?”) and another study [14] did not meet the criteria on item 3.4 (“Are the confounders accounted for in the design and analysis?”).
Table 3 summarises the 22 articles that met inclusion criteria. The articles are separated into two distinct groups: (1) field-based concussion and/or HIK studies, and (2) laboratory-based perturbation studies. The key difference between the groups is that Group 1 recorded data from real-world, live sporting settings, while Group 2 used controlled settings in which study participation was the only task. The study by Schmidt et al. [7] is the only study that falls into both groups. The results of our included articles are presented in these groups.
3.2 Group 1: Field-Based Concussion and/or Head Impact Kinematics Studies (n = 8)
Studies in Group 1 used field-based measurements of concussion and/or head kinematics and correlated them with head and neck characteristics [5, 7, 8, 10, 22, 23, 26, 28]. The relationship between each variable and mTBI is reported in Table 3.
3.2.1 Exposures
Baker et al. [8] followed 130 university varsity athletes (ice hockey, football/soccer, and basketball) throughout their respective seasons. They reported 12 participants (six male) sustained a mTBI in their study (9.2% of study population). Collins et al. [10] followed 6662 high school athletes (lacrosse, football/soccer, and basketball) throughout the 2010 and 2011 academic years. They reported 179 participants (72 male) sustained a mTBI (2.7% of study population). Esopenko et al. [22] followed 324 National Collegiate Athletic Association (NCAA) Division I athletes over their whole college career in 16 sports. They reported 13 participants (nine male) sustained a mTBI (4% of study population). The other five studies in this group related HIK resulting from training and/or game-related head impacts to head-neck characteristics [5, 7, 23, 26, 28].
3.2.2 Measurement of Head Impact Kinematics
All five of the HIK studies in Group 1 reported peak linear head acceleration [5, 7, 23, 26, 28], three reported peak rotational head acceleration [5, 23, 28], Fitzpatrick et al. [26] reported peak rotational head velocity, and Mihalik et al. [5] and Schmidt et al. [7] also reported Head Impact Technology severity profile (HITsp), which is a weighted composite score that takes into account rotational and linear acceleration as well as impact location and duration [7]. Three articles [5, 7, 28] only included impacts over 10 G, while Kelshaw et al. [23] had a threshold of 20 G. Fitzpatrick et al. [26] did not report an impact threshold. Kelshaw et al. [23] and Williams et al. [28] both used video to confirm impacts, and Williams et al. [28] additionally used waveform-analysis to rule out head acceleration data from non-impact events (biting, shouting, and insertion or removal of instrumented mouthguard).
3.2.3 Measurement of Neck Strength
Neck strength in flexion, extension, and right and left lateral flexion was reported by Collins et al. [10] (in pounds), Fitzpatrick et al. [26] (in Newtons), Kelshaw et al. [23] (unitless and normalised with participant body mass), Schmidt et al. [7] (as peak torque and rate of torque development), and Williams et al. [28] (in Newtons). Fitzpatrick et al. [26] also measured left and right rotational neck strength. Baker et al. [8] were alone in investigating neck endurance as measured by the deep neck flexor endurance test (DNFET). Three of the studies analysed their results based on groups. Kelshaw et al. [23] and Mihalik et al. [5] investigated head kinematic outcomes based on grouping into neck strength tertiles for each direction of neck strength measured, while Schmidt et al. [7] investigated their head kinematic results based on high and low performers (two groups, median-split) for each head/neck outcome.
3.2.4 Additional Outcome Measures
Head and neck anthropometrics reported in the six studies included head circumference [7, 10, 23, 28], neck circumference [7, 10, 22, 28], proportional neck circumference [22], neck length [10, 23], and head-neck segment length [7]. Schmidt et al. [7] also investigated neck muscle size as well as neck stiffness assessed through perturbation, which are both mentioned in more detail in Sect. 3.3.1.
3.2.5 Exposure-Outcome Relationships
Of the Group 1 studies that report mTBI incidence [8, 10, 22], only one found significant differences in head-neck outcomes for athletes who did versus did not sustain an mTBI [10]. Collins et al. [10] found neck girth, neck:head girth ratio, and all measures of neck strength were significantly lower in athletes who sustained an mTBI than those who did not. Esopenko et al. [22] found no significant differences in raw or proportional neck circumference measures in athletes who sustained an mTBI compared to those who did not. Baker et al. [8] found that athletes who sustained an mTBI had lower average neck endurance than those who did not; however, the difference was not significant between groups.
For the Group 1 studies that reported HIK [5, 7, 23, 26, 28], four found no significant impact mitigation effect associated with stronger neck muscles [5, 7, 23, 28]. In fact, two found that athletes with stronger necks were at times more likely to sustain more severe head impacts than those with weaker necks [5, 7]. Initially, Fitzpatrick et al. [26] similarly found no association between neck strength and a reduction in HIK. However, upon analysing their data directionally (i.e., mean HIK for impacts on the front of the head correlated with neck extension strength), they found that neck strength significantly and negatively associated with linear acceleration but not rotational velocity in this way. Two studies included head-neck size variables in their analyses with HIK, and neither found significant impact mitigation effects associated with any measured size variables [7, 28]. Schmidt et al. [7] found that players with stiffer necks had reduced odds of sustaining severe and moderate head impacts compared to players with less neck stiffness, as measured by HITsp.
3.3 Group 2: Laboratory-Based Perturbation Studies (n = 15)
Studies in Group 2 used controlled, laboratory-based methods of perturbation of the head and correlated head kinematic response with head and neck characteristics. Methods used to perturb the head were a load attached via pulley system [6, 7, 9, 11, 19], football/soccer heading [12,13,14,15,16,17,18, 27], or an impact sled [20, 21]. The relationship between each variable and mTBI is reported in Table 3.
3.3.1 Load-Drop Studies (n = 5)
Five studies utilized head load applicators that employed headgear attached to a load via a pulley system and imparted a force on the head when the load was dropped [6, 7, 9, 11, 19].
Measurement of head kinematics To capture motion during perturbations, four studies used camera-based motion capture systems, 3D [11, 19], 2D [9] or infrared [6]. Schmidt et al. [7] used an electromagnetic motion capture system. Motion during perturbation was reported in terms of peak angular acceleration [9, 19], peak angular velocity [6, 11], peak linear velocity [6], and angular displacement [7, 9, 11].
Types of perturbation Loading conditions differed between studies; three studies varied force based on participant body mass [6, 7, 11] while the other two did not vary the load between participants [9, 19]. All five papers assessed forced neck extension, while four also examined forced flexion [6, 7, 9, 19]. Eckner et al. [6] also assessed right lateral flexion and left axial rotation, and Debison-Larabie et al. [19] left and right lateral flexion. A “pre-load” was used in two studies, where a load smaller than the dropped load was supported by the participant before the perturbation trial occurred [7, 11]. Alsalaheen et al. [11] also performed perturbations without pre-load. All five studies subjected participants to perturbation while relaxing neck musculature. Two studies asked participants to brace for the impact by pre-activating (tensing) neck musculature [6, 9]. Four studies had a condition where participants were given an indication (i.e., a countdown) of when the weight would be dropped [7, 9, 11, 19]. Eckner et al. [6] did not report whether participants had knowledge of weight drop timing.
Measurement of neck strength Neck strength was measured during maximum voluntary isometric contraction (MVIC) for neck flexion [6, 9, 11], extension [6, 7, 9], lateral flexion [6, 7], and right axial rotation [6]. Two studies also reported rate of neck force development [6, 7] for the same directions as their neck MVIC measures.
Additional outcome measures Other head and neck characteristics reported were neck stiffness [7, 9], head-neck segment length [7, 9], head-neck mass [9], head circumference [7], neck circumference/girth [6, 7, 9, 11], head:neck circumference ratio [19], neck volume [19], physiological cross-sectional area (PCSA) of the sternocleidomastoid [6, 7, 11], upper trapezius, and semispinalis capitis [7].
Exposure-outcome relationships Three groups compared males with females in their analyses [9, 11, 19]. Compared to females, males in these studies had significantly higher levels of neck strength, neck girth, sternocleidomastoid PCSA, neck volume, head:neck girth ratio, head-neck mass, but not head-neck length. Tierney et al. [9] found females experienced significantly greater levels of angular head acceleration and displacement than males, suggesting a beneficial effect in stabilisation of the stronger and larger head-neck segment in males. Similarly, Debison-Larabie et al. [19] found males experienced less angular head acceleration during perturbation than females, but only in flexion and left lateral flexion directions (no significant differences in acceleration were found between males and females for forced extension or right lateral flexion). Alsalaheen et al. [11], however, found no significant differences between males and females in angular head velocity or displacement during perturbation. The study by Eckner et al. [6] included youth athletes below 13 years old in their analyses, whereby neck strength and size had significant main effects for rotational and linear velocity after perturbation. When adjusting for sex and age in the models these effects remained significant. The same trend was seen for the older athletes (comparing college age and older males and females), but the authors did not report statistical analysis for this sub-group as it was not the aim of their study. Schmidt et al. [7, 9, 11] did not analyse the effects of head-neck strength and size variables on response to perturbation as this was not the aim of their study.
3.3.2 Football/Soccer Heading Studies (n = 8)
All eight of the studies in group 2 used controlled football/soccer heading trials to perturb the head [12,13,14,15,16,17,18, 27].
Measurement of head impact kinematics Six of the eight studies recorded HIK using accelerometers [13,14,15,16, 18, 27], with Caccese et al. [15] also utilising gyroscope data. Camera-based motion capture systems were used by four groups, 3D systems by three [12, 15, 27], and a 2D system by Teymouri et al. [17]. Teymouri et al. [17] also used a pressure gauge attached to participants’ foreheads to measure impact force of the ball on the head during trials. Six studies reported peak linear head acceleration during headers [13,14,15,16, 18, 27].Footnote 1 Two reported peak rotational head acceleration [12, 15]. Bretzin et al. [14] reported peak rotational velocity.Footnote 2 Tierney et al. [18] also reported Head Injury Criteria. Teymouri et al. [17] reported head speed and momentum before and after heading.
Types of headers Becker et al. [13] used five heading conditions in their study: standing, running, jumping, and post-fatigue running and jumping. Four of the studies used only the standing header condition [15, 16, 18, 27], with Müller and Zentgraf [27] allowing for one sidestep to complete the header. Teymouri et al. [17] used a less controlled method, instructing participants to defend a free kick from within the penalty box with a header (mean speed of 18.0 ± 2.4 m/s). They reported standing, jumping, and jumping forward headers. Two studies did not report the motion of the participant during the header [12, 14]. Four studies used ball machines to serve the ball to participants, Tierney et al. [18] used a speed setting of 9.8 m/s (22 mph), Müller and Zentgraf [27] used speeds of 9.4 m/s and 10.8 m/s (only male participants received balls at 10.8 m/s), while Bretzin et al. [14] and Caccese et al. [15] both used 11.2 m/s (25 mph) with Bretzin additionally using 17.9 m/s (40 mph). Three studies used another human to serve the ball to the participant. Dezman et al. [12] had an investigator serve the ball to participants at a mean speed of 4.3 ± 0.7 m/s. Gutierrez et al. [16] had a trained football/soccer player perform a throw-in to the participant and did not report ball speed. Becker et al. [13] were the only group to use a stationary ball. Six studies had participants head the ball forwards, either towards a target [15, 18, 27], back to the server [12, 16], or horizontally as hard as possible [13]. Gutierrez et al. [16] also had participants head the ball left and right. Participants in the study by Teymouri et al. [17] were instructed to head the ball away from the goal. Bretzin et al. [14] did not report on the direction of headers.
Measurement of neck strength Bretzin et al. [14] reported neck strength in six directions: flexion, extension, left and right lateral flexion, left and right rotation. Gutierrez et al. [16] and Müller and Zentgraf [27] reported neck strength in four directions: flexion, extension, left and right lateral flexion. Müller and Zentgraf [27] also reported lateral neck strength symmetry and functional neck strength and endurance (for the flexor and extensor muscle chains, these functional measurements had participants activating their neck and other muscles in functionally relevant positions for sport). Three groups reported neck flexion and extension strength [12, 13, 18]. Teymouri et al. [17] reported only neck flexion. Caccese et al. [15] were the only group not to report a measure of neck strength.
Additional outcome measures Five studies also included measures of head-neck size and mass. Bretzin et al. [14] and Tierney et al. [18] reported head-neck segment length and mass, and neck girth. Caccese et al. [15] reported head width, length, depth and girth. Müller and Zentgraf [27] recorded neck length and circumference and reported neck volume. Teymouri et al. [17] reported head girth as well as correlation coefficients for their head-neck anthropometric measures with force exerted from the ball onto the head.
Exposure-outcome relationships The majority of included football/soccer heading studies found that athletes with stronger necks and larger head-neck segments in some way demonstrated reduced HIK during heading. Gutierrez et al. [16] found moderate and consistent negative correlations between neck strength and head acceleration during heading in all directions. The males in the study by Bretzin et al. [14] had stronger necks than females (only significantly different for flexion and left lateral flexion) and experienced lower levels of linear head acceleration and rotational head velocity compared to females for both heading speeds (only the differences in rotational head velocity reached significance). They also found neck girth had negative correlations with rotational velocity and linear accelerations at low ball speeds, but only with linear acceleration at high ball speeds. Females in the study by Tierney et al. [18] had significantly lower head-neck segment mass and length, neck girth, and neck strength than males, and showed significantly greater linear head acceleration in headgear conditions but not in the control condition without headgear. Teymouri et al. [17] found that athletes with larger head circumference experienced less force from the ball during heading than those with smaller head circumference. Initially, Dezman et al. [12] found that neck flexion/extension strength were not correlated with linear or rotational head acceleration. However, they demonstrated that neck strength imbalance (flexion–extension difference) did significantly negatively correlate with angular (but not linear) head acceleration. Two heading studies included a strengthening intervention [13, 27]. Müller and Zentgraf [27] found significant beneficial effect from the intervention on neck strength and functional neck strength and endurance. Participants showed a significant decrease in peak linear head accelerations during heading between pre- and post-intervention measurements for low (9.4 m/s) but not high (10.8 m/s) ball velocity. The strengthening intervention performed by Becker et al. [13] did not produce significant strength changes between intervention and control groups (flexion strength increased for all groups, extension strength did not). Subsequently, training-induced alterations in peak linear head acceleration during football/soccer heading were not significant for any of the five heading conditions. The study by Caccese et al. [15] included youth athletes below 13 years old in their analyses, whereby a significant difference was seen between males and females in head circumference and linear and rotational head acceleration during heading (males had larger heads and experienced lower levels of HIK than females). However, multivariate sex by age analyses did not show these same interaction effects.
3.3.3 Impact Sled Studies (n = 2)
The final two studies in this group used an impact sled to impart force on the heads of military cohorts [20, 21].
Measurement of head kinematics Morris and Popper [21] measured head kinematics using infrared sensors and accelerometers. Mawn et al. [20] did not report how they measured head kinematics. Mawn et al. [20] reported linear x (forwards-backwards) and z (up-down) accelerations and angular y (in the sagittal plane) accelerations. Morris and Popper [21] reported head acceleration in terms of “mean corrected mouth deflection”, which is a unitless value calculated by dividing head displacement by neck length.
Types of sled run Mawn et al. [20] examined acceleration in the -Gx direction (forced flexion, or “eyeballs out”), which was approximately 10 G (10.1 ± 0.2 G). Morris and Popper [21] used a 6.5 G acceleration in the -Gx direction and a 4 G acceleration in the + Gy direction (right lateral flexion, or “eyeballs right”).
Head-neck outcome measures For physical head and neck characteristics, Mawn et al. [20] reported neck length, circumference, and estimated head mass, as well as ratios between these variables ( “stockiness quotient” or neck circumference:neck length ratio, head mass:stockiness quotient ratio, and head mass:neck circumference ratio), while Morris and Popper [21] reported neck extension strength during a static condition and during the sled-run (as headrest force resultant).
Exposure-outcome relationships Both impact sled studies found links between head-neck characteristics and resultant head motion during impact. Mawn et al. [20] performed linear regressions using the abovementioned head-neck size variables and found these variables had a distinct influence on linear and angular head acceleration. They found a strong relationship between anthropometry and linear z-axis (up-down) acceleration, and moderate relationships between anthropometry and linear x-axis (forwards-backwards) and angular y-axis (sagittal plane) accelerations. Morris and Popper [21] initially found static neck strength not to predict head motion as measured by mean corrected mouth deflection. However, they reported that headrest force resultant and static neck strength measurements did not correlate well. When using headrest force resultant as the independent variable instead of static neck strength, they were able to establish strong correlations with head motion for males and females.
4 Discussion
This systematic review provides a comprehensive overview of the relationship between physical head and neck characteristics and mTBI risk. Mixed evidence was found regarding the protective capacities of head-neck strength and size variables against mTBI and head impacts. Fourteen of the 22 included studies established at least one significant association between a head-neck strength or size variable and mTBI risk reduction, while eight of the 22 studies found no significant results.
4.1 Comparison Between Field- and Laboratory-Based Studies
Concerning how impact mitigation translates between less severe laboratory-based impacts to in-game impacts of 10 G + , the study by Schmidt et al. [7] can potentially provide insight given that they assessed both measures. Although they found no impact mitigation effect from neck strength or size, they found that increased neck stiffness and reduced displacement during a low-level (3.5% body mass dropped from 15 cm) laboratory-based perturbation both reduced the odds of sustaining higher magnitude head impacts during play compared to players who demonstrated lower stiffness and larger head displacement. Their results indicate that ability to mitigate low-level impacts may translate to high-level impacts, which justifies our inclusion of proxy mTBI risk measures in the review. Schmidt et al. [7] were not concerned with how head-neck characteristics affected head acceleration during the controlled perturbations, but other groups examined this directly. Tierney et al. [9] found that lower levels of head and neck size and neck strength in females were associated with reduced stiffness and higher head acceleration and angular displacement as compared to males. From their results, for low G impacts there is a link between head-neck strength and size to increased stiffness and reduced head acceleration and head displacement. This finding may indicate that a similar relationship might exist at high G impacts. While Schmidt et al. [7] found that increased stiffness provided a mitigative effect in high G impacts, they did not see the same effect for head-neck size or strength. This result could stem from sex differences in dynamic response, as Tierney et al. [9] compared males and females while Schmidt et al. [7] only included male participants.
4.2 Neck Strength in Field-Based Studies
Many of the studies included in this systematic review showed varying levels of evidence that neck strength provides some protective effect against mTBI incidence and impact severity. Perhaps the most meaningful evidence is from the study by Collins et al. [10]. Their study had a large sample size relative to other studies included (N = 6662). All measures of strength (extension, flexion, left and right lateral flexion) were significantly higher in athletes who did not sustain a mTBI compared to the injured cohort. They state that for every pound (0.45 kg) increase in overall neck strength (averaged across the four directions), the odds of sustaining a mTBI was reduced by 5%. Neck strength did not seem to have the same protective effect when field-based impacts were examined over 10 G and 20 G, with two investigations finding that players with stronger necks were more likely to sustain more severe head impacts as measured by HITsp [5, 7]. In addition, Schmidt et al. [7] controlled for player type and separated participants into skill or line groups based on player position. Linemen are typically larger and stronger than skill players and have substantially different roles to skill players. Due to this role difference, linemen have greater exposure to head impacts than skill players. They found that linemen with stronger necks had increased odds of receiving moderate (66–106 G) and severe (> 106 G) head impacts compared with mild (10–66 G) head impacts. They suggested that players with stronger necks may perceive less risk from impact situations and have more sporting ability than those with weaker necks, and so are more willing to engage in high-energy collisions. They also posited that anticipation and being the striking player may play a role, as the same relationship was not found in skill players, who are not as responsible for initiation of contact as expected by linemen. Another finding was that skill players who could activate neck musculature faster had increased odds of sustaining severe impacts. The investigators suggested that by acting faster to mitigate HIK, the forces imparted on the head act over a shorter amount of time and so are more severe. Baker et al. [8] investigated pre-season neck endurance as opposed to MVIC, measured by the deep neck flexor endurance test (DNFET, laying supine and holding a small neck flexion for as long as possible). While athletes in their study who sustained a concussion had lower pre-season DNFET scores, no significant group differences could be found. Interestingly though, they did find a moderate correlation of DNFET improvement with mTBI recovery, which has some potential clinical utility.
4.3 Neck Strength in Laboratory-Based Studies
Evidence for the protective capacity of neck strength is also mixed when considering lower, controlled impacts in a laboratory setting. Eckner et al. [6] found significant main effects for neck strength on both linear and rotational head velocity. Although their study included children, the effect remained when adjusting for age as a covariate in the model. They also found rate of force development to be a significant predictor of linear and rotational head velocity mitigation in all directions except right lateral flexion. Tierney et al. [9] also found larger values of neck strength significantly reduced angular head acceleration and displacement from the perturbation when comparing between sexes. Both of these studies assessed forced neck flexion and extension. Alsalaheen et al. [11] also compared results between the sexes but only evaluated forced neck extension. Despite the men in their study having stronger necks, no significant differences were seen between males and females for angular velocity or displacement. Bretzin et al. [14] also found a relationship between neck muscle strength and HIK during football/soccer heading. They found that three of the six (flexion, left lateral flexion and left rotation) directions of neck strength they measured correlated significantly with linear acceleration at a low ball-speed, and four of six (flexion, left and right lateral flexion, and left rotation) at a high ball-speed. They did not report if players were standing, running or jumping, or where they were aiming the ball, but did control ball-speed. Gutierrez et al. [16], on the other hand, did not control ball-speed (using a throw-in from another football/soccer player to closely mimic real-life situations), but did report on player motion (standing only) and had players aim left, right or forward. They found neck strength moderately and consistently negatively correlated with linear head accelerations, for all directions of strength they measured (flexion, extension, left and right lateral flexion) and all football/soccer heading directions. Dezman et al. [12], while not finding a protective effect from neck strength magnitude alone, did find that athletes with more symmetrical flexion and extension strength experienced lower angular head acceleration during football/soccer heading than those with greater strength imbalance. Teymouri et al. [17] found no significant correlation between neck flexion strength and force exerted by the ball on the head. Tierney et al. [18] found no correlation between neck strength and head acceleration during heading in a control condition without headgear but did find significant negative correlations between these variables for two headgear conditions. The neck-strengthening program used by Becker et al. [13] did not significantly increase strength for the two intervention groups as compared to a control group. Subsequently, football/soccer heading HIK were also not reduced for the intervention groups or the control group. The intervention group in Müller and Zentgraf [27] had significantly increased neck strength (but not lateral strength symmetry) post-intervention as compared with controls. Compared to pre-intervention measurements, post-intervention mean peak linear head acceleration during heading was reduced by 1.5 G in the low-speed condition and 1.4 G in the high-speed condition; however, only the low-speed condition results reached significance. Morris and Popper [21] found neck strength did not predict head deflection in their impact sled study. However, they did find strong negative correlations between head deflection and headrest force, which is the force exerted on the headrest by a participant the instant before impact. They suggested that motivation plays a key role in the level of force participants are willing to exert. During static neck strength testing, participants are not as motivated to exert maximal neck force as they are during impact sled runs (to protect themselves from the impact). This finding is significant for all studies that assess neck strength included in the current review, as strength was always tested statically in non-motivated conditions. As Morris and Popper [21] found, neck MVIC strength measures taken in the laboratory may not reflect neck force exerted during motivated situations like gameplay and training impacts or other forms of head perturbation. This could contribute to the lack of protective relationship existing between static neck strength and head impact mitigation in Schmidt et al. [7], while such a relationship was found between head impact mitigation in the laboratory and field (when compared to those with lower stiffness, players with higher levels of stiffness in laboratory perturbations had lower odds of sustaining more severe field-based impacts). While the participants had their heads perturbed by a weight drop, they may have been more motivated to maximally activate neck musculature to dissipate the force than in the static neck strength testing condition.
4.4 Head-Neck Size Variables in Field-Based Studies
Another characteristic of interest in some of the included studies is the size of the head and neck. Some researchers propose that neck size can be used as a quick and simple proxy measure of other neck features, such as strength [22]. Studies included in this review did find correlations between head-neck size and mass measurements and neck strength [14, 23]. In addition, increased size of the head-neck segment would reduce head accelerations, whereby for the same force a body with larger mass experiences less acceleration than a body with smaller mass. Indeed, mathematical models have shown a correlation between less head mass and increased accelerations [29]. Collins et al. [10] evaluated neck length and head and neck circumference, as well as the ratio of these anatomical features. Viewing their overall results, neck circumference and neck/head circumference were significantly smaller for the mTBI group. However, when compared within sex, neck circumference difference was not significantly different between groups for either males or females, and neck/head circumference ratio only remained significantly different between the groups for males. Esopenko et al. [22] found neck circumference not to be related to either mTBI sustained during college or to mTBI history. Kelshaw et al. [23] reported head and neck circumference and neck length but did not relate these to HIK in their study, instead relating them to neck strength measurements. A moderately positive correlation was found between neck circumference and extension strength, but no other relationships were statistically significant. Schmidt et al. [7] found that players above the median in neck muscle PCSA were at increased odds of moderate and severe head impacts compared to those below the median PCSA. Again, this could be because players in the upper half of the PCSA distribution feel safer entering high-energy collisions, or due to expectations of these players to participate in collisions.
4.5 Head-Neck Size Variables in Laboratory-Based Studies
In controlled perturbation conditions, head and neck size metrics proved to reduce or partially reduce head deflection severity in some studies [6, 9, 19, 20], but not in others [11]. Alsalaheen et al. [11] found significant differences in neck circumference and SCM PSCA between males and females (males had larger necks), but no difference in angular velocity or displacement. However, it was found that females had a significantly larger neuromuscular response (mean baseline and peak EMG across all perturbation conditions), which may indicate that the males were able to rely on their larger size (and strength) to mitigate impact forces, while females had to use a larger percentage of activation. This is despite the fact that this perturbation protocol was normalised to participant weight. Similarly, Tierney et al. [9] also found that females had faster and larger neuromuscular responses than males. However, in contrast to findings from Alsalaheen et al. [11], Tierney et al. [9] observed significantly greater peak acceleration and head displacement in females compared to males. Tierney et al. [18] found neck circumference and head-neck mass and length to be significantly negatively correlated with resultant head acceleration during headers in both their headgear conditions, but only head-neck mass in their non-headgear condition. Headgear appeared to have different effects on HIK between sexes. Males experienced lower head accelerations when wearing headgear, while females experienced higher head accelerations. The authors attribute this finding to a feeling of safety the headgear might provide and participants feeling as if they must strike the ball harder while wearing headgear. They suggested that the lower head-neck stability (head-neck mass, neck girth, neck flexion and extension strength) in females compared to males in their study may account for why this was not seen in males. Teymouri et al. [17] found head circumference to significantly negatively correlate with the amount of force measured on the head during headers. What this result tells us about injury risk prevention is unclear, however, as it has been reported that injuries during headers depend more on head acceleration than the applied force [30]. Bretzin et al. [14] found neck girth to be significantly and negatively associated with HIK, more so as ball speed increased. Despite measuring head-neck length and mass, they did not report if these correlated with HIK.
4.6 Differences Between Females and Males
Several of the studies included in the present review performed a group analysis between males and females. The general trend in such studies is stronger and larger necks in males as compared to females. This trend, at times, has been taken as evidence that having a stronger and larger neck is responsible for any measured benefits in head impact mitigation. However, as previously discussed, Alsalaheen et al. [11] did find that males and females utilised different neuromuscular strategies under the same load. Tierney et al. [9] also found head acceleration and angular displacement of males to be significantly lower than that of females in their controlled perturbation experiment. When males had knowledge of the incoming perturbation, their angular acceleration was 25% less than without this knowledge. No significant difference was found between the known and unknown conditions in females. While Williams et al. [28] found no significant difference in peak linear head acceleration between males and females, they did see a marked difference in response to impacts, where over 50% of impacts sustained by females resulted in uncontrolled whiplash while only one such event occurred in their male cohort. They attributed this to decreased stability in the female cervical spine as compared to males. As men and women use different strategies to stabilise the head [11], physical size and strength differences alone may not be the only factors at play. In future studies, comparisons should be performed within groups in addition to between them to minimise the influence of any different neuromuscular strategies employed by the sexes on findings.
4.7 Reviews From Other Perspectives
It is worth noting that the role of the head and neck in mTBI risk has been examined by several other reviews through other perspectives. The review by Elliott et al. [31] evaluated the relationship between neck strength and head and neck injuries in sport, and whether neck exercise interventions reduce these injuries. Their review shares similar aims with this review but is broader in its inclusion of head and neck injuries other than solely mTBI, addresses strengthening interventions specifically, and is narrower in its focus on only athletic populations. Other reviews on this topic have either not been systematic [32,33,34,35,36,37,38,39,40,41] or have had a more narrow scope than this review by limiting their search to either specific experimental paradigms [42, 43] or specific physical neck characteristics [44]. To our knowledge, this review is the first systematic review to holistically assess physical characteristics of the head and neck and how they relate to mTBI risk in a broad range of settings. We also included military cohorts in our review, which further differentiates it from the existing literature. In our search terms, we listed popular sports which are known to have high rates of mTBI. However, studies on sports other than those included in our search terms were also captured in our search with the inclusion of “athlete” and “sport” keywords and subject headings, as well as by our manual search efforts of reference lists.
It should be noted that only papers written in English were screened, which is a limitation of this review. Participant age was restricted to 13–65 years, which excluded papers that observed participants outside of this age threshold. Occupational (excluding military service) and vehicular mTBI studies were not included in the search strategy. Additionally, only three of the included studies directly assessed mTBI incidence [8, 10, 22]. The other 19 included studies used indirect measures of mTBI risk, which may limit applicability of any conclusions drawn.
5 Conclusion
From the studies included in the current review and the broader literature, there appears to be evidence of some interaction between physical characteristics of the head-neck segment and mTBI risk, in terms of incidence and biomechanical response to impact. However, these characteristics alone appear to not be sufficient to wholly predict mTBI risk. Other factors, such as neuromuscular response, behaviour, sex, and anticipation of impact also contribute to head impact mitigation. Further large-scale robust prospective investigations are required to determine the exact role that physical head-neck characteristics play in mTBI prevention and impact mitigation.
References
Meaney DF, Smith DH. Biomechanics of concussion. Clin Sports Med. 2011;30(1):19–31.
Iverson GL. Outcome from mild traumatic brain injury. Curr Opin Psychiatry. 2005;18(3):301–17.
Atif H, Hicks SD. A review of MicroRNA biomarkers in traumatic brain injury. J Exp Neurosci. 2019;13:1179069519832286.
Vanderploeg RD, Belanger HG, Curtiss G. Mild traumatic brain injury and posttraumatic stress disorder and their associations with health symptoms. Arch Phys Med Rehabil. 2009;90(7):1084–93.
Mihalik JP, et al. Does cervical muscle strength in youth ice hockey players affect head impact biomechanics? Clin J Sport Med. 2011;21(5):416–21.
Eckner JT, et al. Effect of neck muscle strength and anticipatory cervical muscle activation on the kinematic response of the head to impulsive loads. Am J Sports Med. 2014;42(3):566–76.
Schmidt JD, et al. The influence of cervical muscle characteristics on head impact biomechanics in football. Am J Sports Med. 2014;42(9):2056–66.
Baker M, et al. Exploring the role of cervical spine endurance as a predictor of concussion risk and recovery following sports related concussion. Musculoskelet Sci Pract. 2019;42:193–7.
Tierney RT, et al. Gender differences in head-neck segment dynamic stabilization during head acceleration. Med Sci Sports Exerc. 2005;37(2):272–9.
Collins CL, et al. Neck strength: a protective factor reducing risk for concussion in high school sports. J Prim Prev. 2014;35(5):309–19.
Alsalaheen B, et al. Women and men use different strategies to stabilize the head in response to impulsive loads: implications for concussion injury risk. J Orthop Sports Phys Ther. 2019;49(11):779–86.
Dezman ZD, Ledet EH, Kerr HA. Neck strength imbalance correlates with increased head acceleration in soccer heading. Sports Health. 2013;5(4):320–6.
Becker S, et al. Effects of a 6-week strength training of the neck flexors and extensors on the head acceleration during headers in soccer. J Sports Sci Med. 2019;18(4):729–37.
Bretzin AC, et al. Sex Differences in anthropometrics and heading kinematics among division i soccer athletes. Sports Health Multidiscipl Approach. 2017;9(2):168–73.
Caccese JB, et al. Sex and age differences in head acceleration during purposeful soccer heading. Res Sports Med. 2018;26(1):64–74.
Gutierrez GM, Conte C, Lightbourne K. The relationship between impact force, neck strength, and neurocognitive performance in soccer heading in adolescent females. Pediatr Exerc Sci. 2014;26(1):33–40.
Teymouri M, et al. The relationship between biomechanical-anthropometrical parameters and the force exerted on the head when heading free kicks in soccer. Arch Trauma Res. 2012;1(1):44–8.
Tierney RT, et al. Sex differences in head acceleration during heading while wearing soccer headgear. J Athl Train. 2008;43(6):578–84.
Debison-Larabie C, Murphy BA, Holmes MWR. Difference between male and female ice hockey players in muscle activity, timing, and head kinematics during sudden head perturbations. J Appl Biomech. 2018;34(6):454–61.
Mawn SV, Lambert JJ, Catyb JL Jr. The relationship between head and neck anthropometry and kinematic response during impact acceleration. Aviat Space Environ Med. 1992;63(1):32–6.
Morris CE, Popper SE. Gender and effect of impact acceleration on neck motion. Aviat Space Environ Med. 1999;70(9):851–6.
Esopenko C, et al. Bigger necks are not enough: an examination of neck circumference in incoming college athletes. J Prim Prev. 2020;18:18.
Kelshaw P, et al. Isometric cervical muscle strength does not affect head impact kinematics in high school boys’ lacrosse. Int J Athlet Ther Train. 2018;23(6):234–8.
Moher D, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLOS Med. 2009;6(7):e1000097.
Pluye P, Hong QN. Combining the power of stories and the power of numbers: mixed methods research and mixed studies reviews. Annu Rev Public Health. 2014;35(1):29–45.
Fitzpatrick D, et al. Head impact forces in blind football are greater in competition than training and increased cervical strength may reduce impact magnitude. Int J Inj Contr Saf Promot. 2021;28(2):194–200.
Müller C, Zentgraf K. Neck and trunk strength training to mitigate head acceleration in youth soccer players. J Strength Condition Res. 2020;35:581.
Williams EMP et al. Sex differences in neck strength and head impact kinematics in university rugby union players. Eur J Sport Sci. 2021;1–10.
Schneider K, Zernicke RF. Computer simulation of head impact: estimation of head-injury risk during soccer heading. Int J Sport Biomech. 1988;4(4):358–71.
Mehnert MJ, Agesen T, Malanga GA. “Heading” and neck injuries in soccer: a review of biomechanics and potential long-term effects. Pain Physician. 2005;8(4):391–7.
Elliott J, et al. Injury reduction programs for reducing the incidence of sport-related head and neck injuries including concussion: a systematic review. Sports Med. 2021;51(11):2373–88.
Benson B, et al. What are the most effective risk-reduction strategies in sport concussion? Br J Sports Med. 2013;47:321–6.
Gilchrist I et al. Neck muscle strength training in the risk management of concussion in contact sports: critical appraisal of application to practice. J Athlet Enhance. 2015;04.
Hanson E, et al. Management and prevention of sport-related concussion. Clin Pediatr. 2014;53(13):1221–30.
Honda J, Chang SH, Kim K. The effects of vision training, neck musculature strength, and reaction time on concussions in an athletic population. J Exerc Rehabil. 2018;14(5):706–12.
Hrysomallis C. Neck Muscular Strength, Training, Performance and Sport Injury Risk: A Review. Sports Med. 2016;46(8):1111–24.
Morin M, Langevin P, Fait P. Cervical spine involvement in mild traumatic brain injury: a review. Sports Med. 2016;2016:1590161.
Rowson S, et al. Biomechanical perspectives on concussion in sport. Sports Med Arthrosc Rev. 2016;24(3):100–7.
Streifer M, et al. The potential role of the cervical spine in sports-related concussion: clinical perspectives and considerations for risk reduction. J Orthop Sports Phys Ther. 2019;49:1–22.
Waltzman D, Sarmiento K. What the research says about concussion risk factors and prevention strategies for youth sports: a scoping review of six commonly played sports. J Saf Res. 2019;68:157–72.
Wood TA, Morrison S, Sosnoff JJ. The role of neck musculature in traumatic brain injuries in older adults: implications from sports medicine. Front Med. 2019;6:53.
Le Flao E, et al. Assessing head/neck dynamic response to head perturbation: a systematic review. Sports Med. 2018;48(11):2641–58.
Peek K, Elliott JM, Orr R. Higher neck strength is associated with lower head acceleration during purposeful heading in soccer: a systematic review. J Sci Med Sport. 2020;23(5):453–62.
Enniss TM, et al. Primary prevention of contact sports-related concussions in amateur athletes: a systematic review from the Eastern Association for the Surgery of Trauma. Trauma Surg Acute Care Open. 2018;3(1):e000153–e000153.
Author information
Authors and Affiliations
Contributions
NJC, TLAD and PS conceived the review and designed the review methods with consultation of NB, TEH and NS. NJC ran the literature search and screened all records. NB, TLAD, TEH, NS and PS assisted with title/abstract and full-text screening. Data were extracted by NJC and reviewed by all authors independently. Quality assessment was performed by NJC, TLAD and PS. NJC wrote and edited the manuscript. NB, TLAD, TEH, NS and PS revised and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. Financial support for this review was provided by the Defence Innovation Network and a Macquarie University Research Excellence Scholarship (MQRES) awarded to Nicholas Cooney.
Conflicts of interest
Nathaniel Bates, Nicholas J. Cooney, Tim L. A. Doyle, Timothy E. Hewett, Nathan Schilaty, and Paul Sowman declare that they have no conflicts of interest.
Data availability
All data generated or analysed during this study are included in this published article or the studies it cites.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cooney, N.J., Sowman, P., Schilaty, N. et al. Head and Neck Characteristics as Risk Factors For and Protective Factors Against Mild Traumatic Brain Injury in Military and Sporting Populations: A Systematic Review. Sports Med 52, 2221–2245 (2022). https://doi.org/10.1007/s40279-022-01683-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-022-01683-2