Article Text

Abstract
Background The assumption that more rapid treatment improves survival of advanced non-small cell lung cancer (NSCLC) has not yet been proven. We studied the relation between time-to-treatment and survival in advanced stage NSCLC patients in a large multicentric nationwide retrospective cohort. Additionally, we identified factors associated with delay.
Method We selected 10 306 patients, diagnosed and treated between 2014 and 2019 for clinical stage III and IV NSCLC, from the Netherlands Cancer Registry that includes nationwide data from 109 Dutch hospitals. Associations between survival and time-to-treatment were tested with Cox proportional hazard regression analyses. Time-to-treatment was adjusted for multiple covariates including diagnostic procedures and type of therapy. Factors associated with delay were identified by multilevel logistic regression.
Results Risk of death significantly decreased with longer time-to-treatment for stage III patients receiving only radiotherapy (adjusted HR, aHR >21 days: 0.59 (95% CI 0.48 to 0.73)) or any type of systemic therapy (aHR >49 days: 0.72 (95% CI 0.56 to 0.91)) and stage IV patients receiving chemotherapy and/or immunotherapy (aHR >21 days: 0.81 (95% CI 0.73 to 0.88)). No significant association was found for stage III patients treated with chemoradiotherapy and stage IV patients treated with targeted therapy. More complex diagnostic procedures often delay treatment.
Conclusion Although in general it is important to start treatment as early as possible, our study finds no evidence that a more rapid start of treatment improves outcomes in advanced stage NSCLC patients. The benefit of urgent treatment is probably confounded by unmeasured patient and tumour characteristics and, clinical urgency dictating timelines of treatment. Time-to-treatment and its impact should be continuously evaluated as therapeutic strategies continue to evolve and improve.
- Non-Small Cell Lung Cancer
- Clinical Epidemiology
- Lung Cancer
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Previous literature indicates a complex association between time-to-treatment and survival for advanced non-small cell lung cancer. We studied this relation in a Western country with equal access to healthcare and identified factors associated with longer waiting times.
What this study adds
The ‘sicker-quicker’ effect is most likely caused by unmeasured confounders relating to patient and tumour characteristics rather than factors related to the hospital infrastructure. Also effectiveness of therapy and presence of an actionable mutation seem to surround this paradox.
How this study might affect research, practice or policy
An ongoing evaluation of time-to-treatment and its impact on outcomes will be needed as therapeutic strategies continue to evolve and improve.
Introduction
Non-small cell lung cancer (NSCLC) accounts for approximately 85% of all lung cancer diagnosis and has an overall 5-year survival rate of only 24%.1 2 Most patients have locally advanced or metastatic disease at the time of presentation, which is likely to be a result of the long time before symptom onset.3 In recent years, the arrival of immunotherapy, targeted therapy and combined chemoimmunotherapy improved prognosis of advanced NSCLC.4–6 Molecular diagnostics have become part of the clinical routine to identify patients who may benefit from targeted therapy or immunotherapy.7 Although these tests can improve patient outcomes, the diagnostic turnaround time may result in prolonged time-to-treatment.8 Delays in the diagnostic work-up are conceived as a medical risk due to the aggressiveness of advanced NSCLC.9 10
In the Netherlands, guidelines and several medical institutions have published timelines to establish standards for timely care of patients with known or suspected (lung) cancer varying from 30 to 49 days.11–14 Variations in these recommendations mark a national heterogeneity that is reflected by a Dutch retrospective cohort study.15 In this study, substantial differences in time-to-treatment on hospital-level were reported for advanced NSCLC with medians ranging from 17 to 68 days.15
The assumption is that prompt diagnosis and treatment lead to better patient outcomes. However, not all evidence supports this: previous literature frequently found shorter time-intervals to be associated with poorer survival for advanced NSCLC.16–21 The evidence for benefit of shorter time intervals seems stronger for surgical early-stage NSCLC patients.22 The paradoxical findings for advanced stages indicate a complex association between time-to-treatment and survival. We suspect that this association is not only influenced by patient and tumour characteristics but also determined by hospital infrastructure such as the turnaround time of diagnostic tests.23 Therefore, the objective of this study was twofold: First we examined the association between time-to-treatment and overall survival (OS) in a large nationwide retrospective cohort. Second, we identified factors associated with a longer time-to-treatment.
Material and methods
Source
Information regarding clinical stage III and IV NSCLC patients from 2014 to 2019 was retrieved from The Netherlands Cancer Registry (NCR), after approval by the Privacy Review Board. In accordance with the regulations of the Central Committee on Research involving Human Subjects, this observational retrospective cohort study does not require approval from an ethic committee in the Netherlands. The NCR collects data on all cancer patients diagnosed in the Netherlands, based on notification of newly diagnosed malignancies by the national automated pathological archive and hospital discharge diagnoses. The data had been collected in 109 hospitals and includes information on patient and tumour characteristics, diagnostics and treatment and is extracted routinely from the medical records by specially trained NCR personnel. Tumour staging was recorded according the seventh and eight edition of the TNM (T=tumor, N=node, M=metastasis) classification.24 Information on vital status and date of death is updated annually using a computerised link with the national civil registry. Information on performance status is registered since 2015, and information on comorbidities, lung function tests and smoking status is not available.
Patient selection
From 2014 to 2019, the NCR recorded 58 312 patients diagnosed with clinical stage III or IV NSCLC. The following cases were considered eligible: age >18 years and patients who received tumour-directed treatment (stage III: chemoradiotherapy, radiotherapy or systemic therapy; stage IV: systemic therapy). We excluded patients with a time-to-treatment of <0 days or >180 days (<1%) and missing information on time-to-treatment. Negative time intervals were for example seen in patients who have visited pulmonologists in multiple hospitals. A maximum cut-off value of 180 days was used as larger time intervals were mostly caused by patients’ preferences. Because the Dutch Lung Cancer Guidelines allow other lead times for patients with an indication for mediastinoscopy (49 days), these patients were excluded.14 Additionally, we excluded patients who entered the clinical pathway differently (eg, via the emergency department instead of an outpatient appointment) because these patients represent a group with symptomatic disease leading to different choices and possibilities in the diagnostic pathway. These patients often suffer from other primary health problems or show acute lung cancer-related symptoms. This may affect the relation between time-to-treatment and survival differently from those patients who enter the diagnostic pathway via an outpatient visit with a pulmonologist. After exclusion, 10 306 patients were included for analysis (figure 1). All patients were followed from the index to death or February 2020.
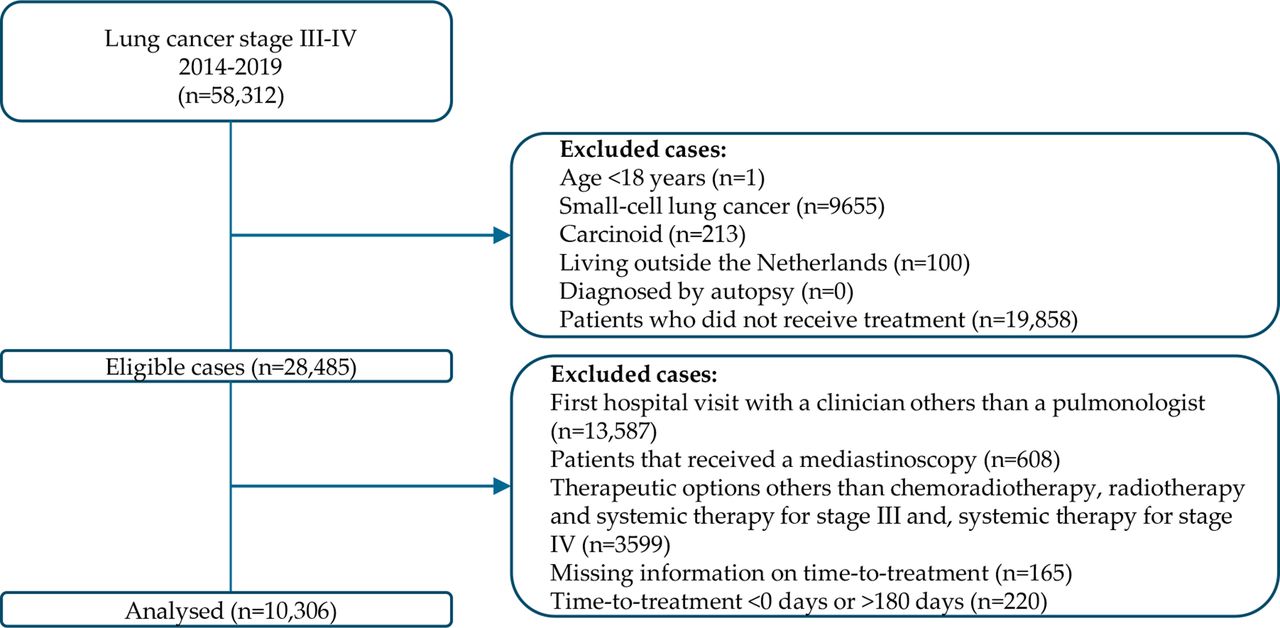
Study flow chart.
Study variables
Our main variable of interest was time-to-treatment, calculated in days from first outpatient visit with a pulmonologist for suspected lung cancer till start of treatment.14
We have discussed all variables of the NCR dataset thoroughly with medical experts involved in lung cancer care (eg, pulmonologist, radiologists). For multivariable analysis, we selected those variables that could affect OS and timing of treatment: age was grouped in 18–60, 61–70, 71–80 and 80+ years. History of cancer was registered if the patient was diagnosed with another type of cancer 5 years before NSCLC. Socioeconomic status was provided by the Netherlands Institute for Social Research at an aggregated level for each postal code and determined from the average income, proportions with low income, low educational level, and unemployment, and categorised as low (1–4), intermediate (5–7) and high (8–10). Year of diagnosis was grouped in 2014, 2015–2016 and 2017+. Since the impact of age, socioeconomic status and year of diagnosis was not linear, these factors were included as categorical variables in the model. We based categorisation of year of diagnosis on the development of (new) therapeutic strategies and agents (ie, introduction of immunotherapy in 2015 for stage IV) and the introduction of the eight version of the TNM classification in 2017. The well-being of the patient was indicated by the Eastern Cooperative Oncology Group Performance Status (ECOG PS) and the Karnofsky scale (10–100). Karnofsky scores were converted to ECOG PS and grouped in 0, 1, 2, 3–4 and unknown.25 The histology of the tumour was grouped by type according to the third edition of the International Classification of Disease for Oncology: adenocarcinoma, squamous cell carcinoma, large cell carcinoma and clinical diagnosis wherever pathological confirmation was not possible. Distant metastasis were categorised in M1a and M1b/M1c. Treatment with chemoradiotherapy included concurrent and sequential, whereas concurrent was defined as chemotherapy and radiotherapy starting within 30 days from each other and sequential as chemotherapy and radiotherapy starting between 30 and 90 days from each other.26 Systemic therapy comprised of chemotherapy, immunotherapy, targeted and combined chemoimmunotherapy while radiotherapy covered stereotactic body radiation therapy and radiation focused on primary tumour and, on metastasis.
Analysis
Statistical analyses were conducted in SAS, V.9.4 (SAS Institute). Descriptive statistics were presented as proportions of patients per stage and therapeutic strategy (table 1). Stratification according to stage was consistently applied in further statistical analysis where the significance level was set at a p<0.05. The data were also stratified for type of therapy in the survival analysis. Primary outcomes were OS in relation to time-to-treatment and, factors associated with longer time-to-treatment. OS was calculated as the time in days between start of treatment until day of death or 1 February 2020.
Patients’ demographic and clinical characteristics by stage and type of therapy for advanced NSCLC who were diagnosed and treated between 2014–2019 in the Netherlands
First, we studied the association between time-to-treatment and OS using a multivariable Cox proportional hazards (PH) model. Time-to-treatment was tested for data-driven quartiles (first: 0–21 days, second: 22–35 days, third: 36–49 days, fourth: >49 days) as there is a lot of (inter)national variation between recommended time-to-treatment intervals, and this provided an equal distribution of patients across the different intervals. This way ensured sufficient power in all categories. The first quartile served as reference. Prior to analysis, the PH assumption was examined to determine whether the HR for any parameter was constant over time. Non-proportionality was detected by a graphical approach and proportionality tests. Other covariates were selected for their prognostic association with survival by use of backward and forward stepwise selection and parameters with p>0.05 were removed from the model. The covariates included in each model are cited in tables 2 and 3 may differ between the models. The dataset was stratified according to type of therapy to account for effect modification. In addition, the model of stage IV disease was extended for subtype of systemic therapy due to prognostic differences. We combined immunotherpy and chemotherapy as immunotherapy was only offered as second line therapy during the first years of the study period. The study was underpowered to perform additional analyses for stage III receiving systemic therapy. The association was determined by adjusted HRs (aHRs), 95% CI and p values. AHRs >1.0 with p<0.05 represented an increased hazard of death. We used the Kaplan-Meier method and log-rank tests to determine how OS varied with stage and type of therapy across the quartiles.
Multivariable Cox regression clinical stage III and IV NSCLC; (aHR (95% CI)) for mortality associated with time-to-treatment
Multivariable Cox regression clinical stage IV NSCLC (subtypes of systemic therapy); (aHR (95% CI)) for mortality associated with time-to-treatment
Next, we identified factors associated with a delay in time-to-treatment by multivariable analysis using multilevel logistic regression. The first quartile served as reference (ie, 0–21 days). As the data had a hierarchical structure, meaning that patients are nested within hospitals, a multilevel model was used including the hospital of diagnosis as random-effect parameter.27 The analysis included age, gender, year of diagnosis, diagnostic staging procedures and type of therapy as fixed effects, while hospital of diagnosis was included as a random effect. The statistical significance of the fixed parameters was evaluated in forward and backward analysis. Parameters with a p>0.05 were eliminated from the model. Model fit was assessed by Bayesian Information Criterion. The intraclass correlation coefficient (ICC) was calculated to quantify the fraction of the total variability in the outcome attributable to the clustering effect.27
Results
Patient population
This retrospective cohort (figure 1) included 10 306 patients, 57% of which were male (table 1). Median age was 68 years in stage III and 67 years in stage IV patients, and 74% of the total population was >60 years. Forty-nine per cent was diagnosed with stage III and 51% with stage IV. For stage IV disease, distant metastases were most commonly staged as M1b (38%). This category involves patients with stage M1b according to the seventh and eighth TNM edition, meaning patients with multiple and solitary distant metastases. Of the included stage III patients, 55% received chemoradiotherapy, 27% radiotherapy and 18% systemic therapy. Other demographic and clinical characteristics are listed in table 1.
Time-to-treatment
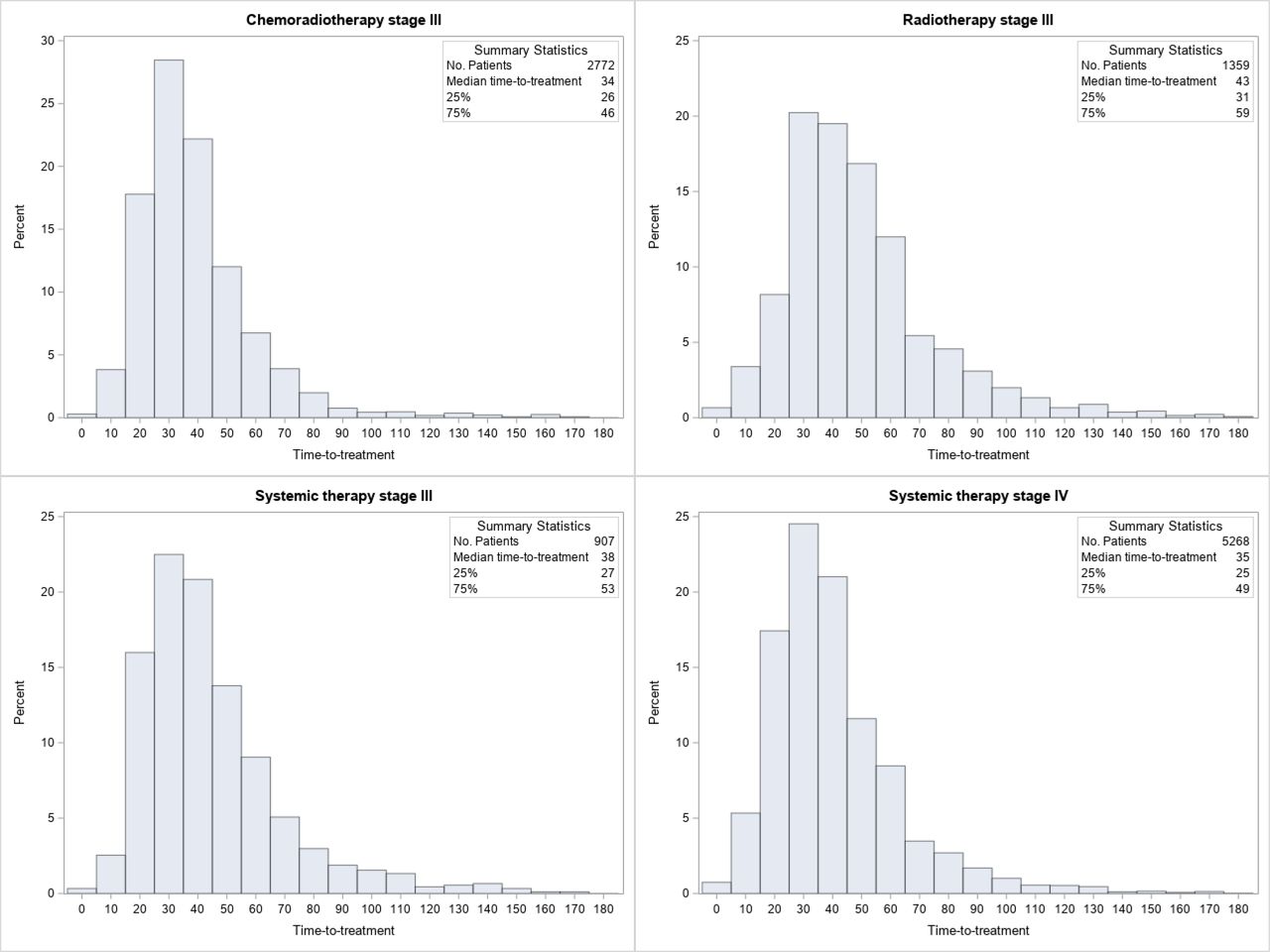
For 53% of stage III patients and 48% of stage IV patients treatment was initiated beyond 35 days. The median time-to-treatment was 37 days (IQR: 27–51) for stage III and 35 days (IQR: 25–49) for stage IV. For stage III, median intervals per type of therapy were 34 days (IQR: 26–46) for chemoradiotherapy, 43 days (IQR: 31–59) for radiotherapy and 38 days (IQR: 27–53) for systemic therapy. Figure 2 presents the distribution of time-to-treatment per stage and type of therapy.

Distribution of time-to-treatment per stage and type of therapy.
Time-to-treatment and survival
The median OS was 22 months for stage III and 10 months for stage IV. The 1-year, 3-year and 5-year OS rate was 71%, 37% and 25% for stage III and, 44%, 16% and 9% for stage IV, respectively. Stage III patients treated with chemoradiotherapy (1-year, 3-year and 5-year survival rates 76%, 41% and 29%, respectively) and stage IV patients treated with targeted therapy (61%, 31% and 14%, respectively) presented with better OS compared with other therapeutic strategies (figures 3 and 4). Figure 5 illustrates Kaplan-Meier plots of time-to-treatment by stage and type of therapy. For stage III patients receiving only radiotherapy or systemic therapy and stage IV patients treated with chemotherapy and/or immunotherapy, significant differences were found between the time-to-treatment intervals (log-rank p<0.0001, p=0.003 and p<0.0001, respectively). The multivariable adjusted survival analysis showed no significant association between time-to-treatment and OS in stage III patients treated with chemoradiotherapy. In stage III patients receiving radiotherapy or systemic therapy, longer waiting times were significantly associated with a lower risk of death (radiotherapy aHR 22–35 days: 0.65, 95% CI 0.51 to 0.82; aHR 36–49 days: 0.55, 95% CI 0.44 to 0.69; aHR >49 days: 0.59, 95% CI 0.47 to 0.73; systemic therapy aHR >49 days: 0.72, 95% CI 0.56 to 0.91, table 3). In stage IV patients, time-to-treatment beyond 22 days was associated with a lower risk of death (aHR 22–35 days: 0.89, 95% CI 0.82 to 0.98; aHR 36–49 days: 0.84, 95% CI 0.77 to 0.93; aHR >49 days: 0.77, 95% CI 0.70 to 0.85). Stratified analysis for subtypes of systemic therapy showed no significant association between time-to-treatment and survival for patients treated with targeted therapy. For patients treated with chemotherapy and/or immunotherapy, time intervals beyond 22 days were associated with a lower risk of death (aHR 22–35 days: 0.87, 95% CI 0.79 to 0.97; aHR 36–49 days: 0.80, 95% CI 0.72 to 0.89; aHR >49 days: 0.72, 95% CI 0.64 to 0.81). Tables 2 and 3 show the aHRs of time-to-treatment stratified per type of therapy. Online supplemental files 1 and 2 provide insight in the dominance of covariates that were selected for multivariable analysis.
Supplemental material

Kaplan-Meier plot stage III therapeutic strategies (chemoradiotherapy, radiotherapy, systemic therapy).
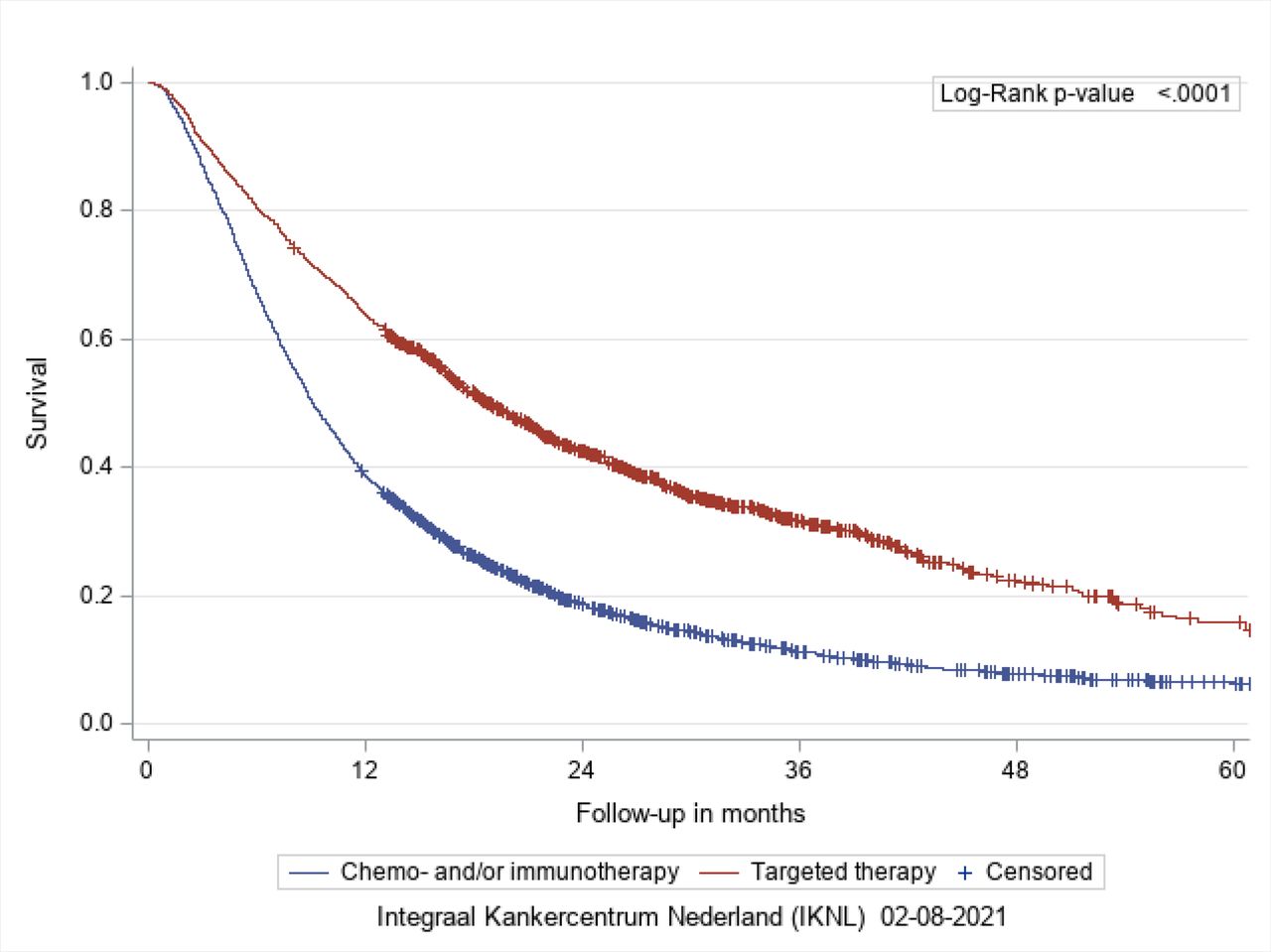
Kaplan-Meier plot stage IV systemic therapy (chemotherapy and/or immunotherapy, targeted therapy).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier plots time-to-treatment by stage and type of therapy.
Factors associated with a delay in time-to-treatment
Patient characteristics, such as age >80 years (stage III: OR 1.57, 95% CI: 1.23 to 2.02; stage IV: OR 1.79, 95% CI: 1.32 to 2.42), were a significant predictor with prolonged time-to-treatment (table 4). Also, diagnostic procedures like EBUS (stage III: OR 1.81, 95% CI: 1.58 to 2.07; stage IV: OR 1.69, 95% CI: 1.44 to 1.99), explorative surgery (stage III: OR 10.9, 95% CI: 4.02 to 29.7; stage IV: OR 8.16, 95% CI: 2.94 to 22.7) and transthoracic biopsy (stage III: OR 2.24, 95% CI: 1.72 to 2.90; stage IV: OR 2.08, 95% CI: 1.67 to 2.60) significantly increased the odds for delay. For stage III patients, treatment with radiotherapy (OR: 2.34, 95% CI: 1.99 to 2.74) or systemic therapy (OR: 1.58, 95% CI: 1.34 to 1.86) was less often initiated within the first and second quartile (≤35 days) compared with chemoradiotherapy.
Multivariable analysis by multilevel logistic regression; factors associated with a delay in time-to-treatment
We also found factors that were significantly associated with shorter time intervals in both stages. For stage III patients, a performance status >2 (OR: 0.62, 95% CI: 0.41 to 0.93) significantly decreased the odds for delay. For stage IV, a missing performance status (OR: 0.79, 95% CI: 0.68 to 0.94), distant metastasis staged as M1b or M1c (OR: 0.80, 95% CI: 0.71 to 0.91) and targeted therapy (OR: 0.78, 95% CI: 0.68 to 0.89) were significantly associated with shorter intervals. Other factors are detailed in table 4. The ICC indicates that 4%–8% of the total variation in the probability of longer waiting times is accounted for by the hospital characteristics. This leaves 92%–96% to be accounted for measured or unmeasured factors others than the hospital, such as patient and tumour characteristics.
Discussion
Present observational findings demonstrate a complex association between time-to-treatment and survival for advanced NSCLC. A longer time-to-treatment was significantly associated with a lower risk of death for stage III patients treated with radiotherapy or systemic therapy and for stage IV patients treated with chemotherapy and/or immunotherapy. No significant association with survival was found for stage III patients treated with chemoradiotherapy and stage IV patients treated with targeted therapy. With this study, we distinguish ourselves from others by identifying factors associated with longer time-to-treatment intervals using a multilevel approach and performing stratified analysis for stage and type of therapy.
Although we have corrected for multiple confounders, the cause of the paradoxical association remains unsolved. We believe that this complex association is probably confounded by unmeasured patient and tumour-specific factors rather than hospital related factors. Especially, as the multilevel logistic regression analyses showed a low interhospital variability, which may relate to the well-organised healthcare and compulsory basic level of healthcare insurance in the Netherlands. Clinical urgency seems to dictate timelines of treatment as advanced stage patients presenting with severe signs and symptoms receive treatment more promptly compared with fitter patients. Also, effectiveness of therapy, inherent to OS prognosis, appears to surround the paradoxical effect. Although our study finds no evidence that urgent treatment is associated with improved outcomes in advanced NSCLC, we still would like to stress the general importance of early diagnosis and treatment. Especially as cancer stage remains the most important predictor of lung cancer survival28 and delays to diagnosis and treatment can cause significant emotional distress to patients and their care-givers.29 Diagnostic procedures appeared to be responsible for longer waiting times. However, these factors might have resulted in the selection of more complicated diagnostic procedures for patients fit for treatment.
A recent systematic review reported that timely care was associated with worse prognosis in advanced NSCLC.21 This finding is in line with our results. We believe that this paradox partly relates to a sicker quicker phenomenon; More aggressive tumours are likely to cause symptoms that would draw attention to the underlying cancer and may prompt to fast diagnosis and treatment,30 but would also spread more rapidly and result in poorer prognosis.31 32 For example, a performance status >2 in stage III patients significantly decreased the risk for treatment delay (OR 2.24, 95% CI: 1.72 to 2.90). Presence of superior vena cava obstruction may be an important indicator for prompt palliative radiotherapy in stage III NSCLC patients.33 For stage III chemotherapy, no paradox was found as this therapy is applied to fitter patients and therefore minimises the sicker-quicker effect. Unfortunately, we could not get this information from the dataset, and we were not able to explain the exact cause since the paradox remained after correcting for factors as performance status and age. Potential unmeasured confounders surrounding the ‘sicker-quicker effect’ could be symptom level at presentation, therapy intent (potentially curative vs purely palliative), comorbidities, tumour biology and tumour mass.34 35 However, it is extremely difficult to identify and account for these (unmeasured) confounders as retrospective analysis rather catches trends than quantifies the impact at an individual level. We believe that registration studies should collect more details on patient and tumour characteristics with regard to disease progression, prognosis and comorbidities. Added, future research should focus on subgroup analysis, with respect to stage, type of therapy, therapy intent, histology, comorbidities and presence of a targetable mutation, to limit heterogeneity and quantify the impact at a more individualised level.
Discovery of new molecular alterations and development of targeted therapy demonstrated major improvements over conventional chemotherapy when applied to the appropriately selected advanced patients.36 37 Presence of an actionable mutation seems to affect the association between time-to-treatment and survival since we found different outcomes across subtypes of systemic therapy. This likely relates to effectiveness of therapy as the OS prognosis remains poor for patients receiving conventional chemotherapy, making time-to-treatment less relevant.38 39 Another potential confounder is behaviour of tumours with a targetable mutation as a longer volume doubling time was found in NSCLC patients with a positive epidermal growth factor receptor (EGFR) mutation compared with a negative mutational status (median: 676 days vs 139 days).40 We suspect tumours with a positive mutational status to have a slowly progressive and less aggressive character. For these patients, clinicians seem to have time for optimal pretreatment assessments. While the field of targeted and immunotherapy continues to evolve and improve, time-to-treatment and its impact may also become more relevant. An ongoing evaluation of time-to-treatment and its impact on outcomes will be needed parallel to these developments.
Molecular diagnostics have become standard in clinical routine to identify patients who may benefit from targeted therapy or immunotherapy.7 However, previous Dutch studies showed that the molecular testing rate increased significantly from 73% in 2013 to 81% in 2017.41 42 Though, about 15% of the patients did not receive targeted therapy despite presence of a targetable mutation.43 This suggests a suboptimal diagnostic pathway in the past years that might have affected patient outcomes and potentially acts as a confounder in relation with time-to-treatment.
The strengths of our study mainly relate to the nationwide coverage of the database. We have created a platform that can be used in future research to restudy the impact of time-to-treatment on advanced NSCLC. Due to the large sample size, we were able to stratify analysis without being underpowered. Added, the availability of a broad range of patient variables in the NCR database enabled us to account for various potential confounders. Also, we selected a recent patient cohort to ensure that our data reflects the current clinical situation. Thereby, all patients included had equal access to oncology care as health insurance is obligated in the Netherlands. Next, we evaluated the complete timeframe as we used first outpatient visit for the suspicion of lung cancer as starting point of the interval. Last, we have tried to correct for immortal time bias by calculating the OS for every patient from start of treatment. However, measuring survival from the start of treatment does not account for the group of patients that deteriorated before having treatment. One way to do this is to stratify analysis by histology, stage and comorbidity as this limits confounding by not including a heterogeneous group of stages or treatments.44 Yet, we have prioritised stratification for stage and type of therapy as we lack power for histology. Alternatively, we adjusted for histology in our multivariable analysis. Future research should focus on subgroup analysis and the relationship between diagnostic delays and deterioration of performance status over time.
This study also has some limitations. For instance, detailed information on comorbidities, smoking information, lung function test and psychosocial status are not available in the NCR, therefore limiting the possibility to explore the impact of these variables. Especially psychosocial status is of particular importance in pretreatment assessment when considering patients’ perspective.29 Delay in time between diagnostic workup and start of treatment is undesirable as this potentially causes significant emotional distress and impaired health-related quality of life. Also, information on performance status and transthoracic biopsy is missing for a subgroup of patients as the NCR started this registration since 2015 and 2017, respectively. As these subgroups consisted of relatively high numbers of patients, we classified the status as unknown rather than exclude them from analysis. Excluding patients with missing data from the analysis provided similar results. Last, our findings were obtained in a country with universal public healthcare and can therefore only be generalised to countries with a similar healthcare status.
Conclusion
Our study finds no evidence that a more rapid start of treatment improves outcomes in advanced NSCLC. A paradoxical effect was seen for stage III patients treated with radiotherapy or systemic therapy and stage IV patients receiving chemotherapy and/or immunotherapy: survival was better in patients with longer time-to-treatment. The benefit of urgent treatment is probably confounded by unmeasured patient and tumour characteristics, and clinical urgency dictating timelines of treatment. Patients presenting with severe signs and symptoms seem to receive treatment more promptly compared with fitter patients. Despite our findings, clinical timeliness should still be approached carefully for each patient to ensure accurate and timely care. Future research should focus on subgroup analysis, with respect to stage, type of therapy, therapy intent, histology, comorbidities and presence of a targetable mutation, to quantify the impact at a more individualised level. As therapeutic strategies for advanced NSCLC continue to evolve and improve, also time-to-treatment and its impact may become more relevant. Therefore, an ongoing evaluation will be needed.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank the registration team of the Netherlands Comprehensive Cancer Organisation (IKNL) for the collection of data as well as IKNL staff for scientific advice. Special thanks to Ronald Damhuis and Matteo Cellamare for their advice on the statistical analyses.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conceptualisation: MP, OCJS, MMvdH, MJA and SEK. Methodology: MP, OCJS, MJA and SEK. Formal analysis and Interpretation: MJA and SEK. Writing-original draft preparation: OCJS, MT, MJA and SEK. Writing-review and editing: MP, OCJS, MMvdH, MJA, MT and SEK. Supervision: MP, OCJS, MMvdH and MT. Project administration: SEK. Guarantor: OCJS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Outside the submitted work MJA has received a research grant from Amgen (paid to the institution).
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.