
Abstract
Considerable research has documented risk factors of physical aggression in adolescence. However, less is known of sex differences in these associations. The current study addressed this important area by examining sex differences in concurrent associations of physical aggression with mental health concerns, trauma exposure, and substance use. The study sample consisted of 3686 boys (mean age 15.9 years) and 3881 girls (mean age 16.0 years) from Young-HUNT3, a population-based study of adolescents in Norway. Logistic regression was used to analyze the association of physical aggression, measured as involvement in physical fighting, with possible risk factors: attention problems, anxiety and depression, loneliness, self-esteem problems, trauma exposure, PTSD symptoms, and substance use. Twenty-one percent (n = 773) of boys and three percent (n = 133) of girls reported participating in physical fights. The results indicated that all risk factors were associated with physical aggression in the total sample as well as in boys and girls separately. Interaction effects with sex emerged for attention problems, anxiety and depression, loneliness, traumatic events, alcohol intoxication, and narcotics use, with larger odds ratios for girls than for boys. Attention problems, traumatic events, and alcohol intoxication showed unique associations with physical aggression for both boys and girls, in addition to PTSD symptoms for boys. In sum, boys’ and girls’ engagement in physical aggression was associated mainly with the same risk factors, but several of the factors increased the relative risk more for girls than for boys. The findings can inform interventions targeting physical aggression in adolescence.
Highlights
-
Sex differences were explored in concurrent associations between physical aggression and mental health concerns, trauma exposure, and substance use.
-
Twenty-one percent of boys and three percent of girls reported participation in physical fights.
-
Physical aggression was associated mainly with the same risk factors for boys and girls, but several of the factors increased the relative risk of physical aggression more for girls than for boys.
-
The findings can be used to improve clinical and societal interventions targeting physical aggression.
Similar content being viewed by others

Interpersonal violence is identified as the fourth leading cause of death among 15- to 19-year-old adolescents worldwide (Mokdad et al., 2016). The prevalence of physical aggression peaks in early childhood and decreases by adolescence, following the course of social, cognitive, and emotional development (Cote et al., 2006; Tremblay, 2000, 2014). However, some children and adolescents continue to engage in physically aggressive behavior, which can lead to vast consequences for victims and perpetrators (Kassing et al., 2019; Macmillan, 2001; Odgers et al., 2008).
In the area of aggression research, one of the most consistent findings is that boys are more physically aggressive than girls (Cleverley et al., 2012; Lansford et al., 2012). Sex differences in physically aggressive behavior can be detected as early as 17 months of age (Baillargeon et al., 2007), and are shown to persist throughout childhood and adolescence (Archer, 2004; Card et al., 2008). In a cross-sectional study of physical aggression in adolescence across 63 countries, the results indicated that 12- to 15-year-old boys were more than twice as likely (OR = 2.68) to report physical fighting compared to girls (Nivette et al., 2019). Similarly, in a national survey with adolescents in the United States (grades 9 to 12), 30% of boys and 17% of girls reported participating in physical fighting (Kann et al., 2018). Possibly due to the difference in rates, aggression has been studied more in boys than in girls, and many studies have used only boy samples (Froyland & von Soest, 2020; Nagin & Tremblay, 1999; Underwood et al., 2001). There is considerable literature on the risk factors of aggression (Farrington et al., 2017; Valois et al., 2002), but much less research has been dedicated to understanding sex differences in risk factors of physical aggression during adolescence. Here we use data from a large, population-based study with a sufficient sample size to explore sex differences in associations between risk factors related to psychological distress and risk behavior and physical aggression in adolescence.
Aggressive behavior is associated with various forms of psychopathology, with strong relations identified for emotion dysregulation and impulsivity (Connor et al., 2019). Mental health problems tend to increase in adolescence, and many disorders and related concerns affect girls and boys to different extents. For example, while ADHD is more prevalent in boys than in girls, internalizing problems are more prevalent in girls than in boys (Arnett et al., 2015; Hagquist, 2010). Positive associations of ADHD and depression with aggression have been well documented (Dutton & Karakanta, 2013; Fontaine et al., 2008; Reed et al., 2017). However, anxiety has been shown to both increase the risk of and protect against aggression (Hatfield & Dula, 2014; Murray et al., 2018), and loneliness and low self-esteem have been associated with aggression in some studies (D’zurilla et al., 2003; Donnellan et al., 2005; Schinka et al., 2013), but not in others (Stickley et al., 2014; Walker & Gudjonsson, 2006). Despite the general lack of focus on sex differences in adolescence, a small number of studies have examined and identified sex differences in associations between aggression and psychiatric symptoms in adolescence. Results have indicated a stronger association between ADHD and aggression for boys than for girls (Ruchkin et al., 2008) and a stronger association between depression, anxiety, and loneliness, and aggression for girls than for boys (Benarous et al., 2015; Storch et al., 2004).
Exposure to traumatic events and symptoms of Post-Traumatic Stress Disorder (PTSD) can also increase the risk of physical aggression (Arata et al., 2007; Marsee, 2008). Although girls are more likely to be exposed to traumatic events than boys (Baglivio et al., 2014; Duke et al., 2010), the consequences of exposure can vary by sex (Aebi et al., 2017; Leban & Gibson, 2020). In a study examining associations between multiple adverse childhood experiences and physical aggression in adolescence, a cumulative effect was indicated, implying that one additional adverse childhood event (ACE) increased the risk for physical fighting by 65% for boys and 60% for girls (Duke et al., 2010). Another study showed that traumatic events were associated with delinquency for boys and substance use for girls (Leban & Gibson, 2020). The effects of ACEs on physical fighting in adolescence can be direct and indirect, mediated through PTSD symptoms (Aebi et al., 2017; Marsee, 2008; Ruchkin et al., 2007). Of relevance to our study, Aebi et al. (2017) reported, in a sample of 15-year-old adolescents, that PTSD symptoms were associated with an increased risk of physical aggression for boys and girls, while a mediating effect of PTSD symptoms on the association between trauma exposure and physical aggression was detected only for boys. In another study, trauma-related psychological distress predicted physical aggression equally in boys and girls in early adolescence (Thompson & Farrell, 2019).
Substance use, and drinking alcohol in particular, is also known to be associated with aggressive behavior in adolescence (Bachman & Peralta, 2002; Tomlinson et al., 2016). In a US national survey, boys and girls (grades 9 to 12) reported comparable rates of participation in binge drinking and marijuana use (Kann et al., 2018). An association between narcotics use and aggression in adolescence has been found (Bachman & Peralta, 2002; Swahn & Donovan, 2004), but no sex difference was found in these studies. For alcohol use, a dose-response relation between alcohol use and risk of aggression has been found (Kivimäki et al., 2014; Robertson et al., 2020; Wells et al., 2008), and in a college student sample, the association was found to be stronger for boys than girls (Quinn et al., 2013).
In summary, much more research on physical aggression has been conducted on boys than on girls, leaving girls’ physical aggression less well understood. Studies have also tended to focus on younger samples or samples with limited age range, with only one sex, or with limited sample size, not allowing direct sex comparisons. This study adds to the gap in the literature by examining potential sex differences in multiple risk factors in a large non-clinical population sample of boys and girls in the age range of early to late adolescence. Adolescence is an important developmental period for the study of risk factors of aggression, as many adolescents engage in risky behavior due to increased peer influence and decreased parental supervision (Galambos et al., 2003; Racz & McMahon, 2011). Also, the prevalence rates of potential risk factors for aggression, such as various types of psychological distress, increase during adolescence, and differentially affect boys and girls (Hagquist, 2010; Merikangas et al., 2010). However, for several of the commonly cited mental health risk factors, empirical support has been inconsistent, and exploring them in boys and girls separately could provide important information on risk factors of physical aggression in adolescence. Thus, the objective of this study was to examine concurrent associations between physical aggression and various mental health problems, trauma exposure, and substance use in adolescence, and to study whether these associations differ between boys and girls. Based on previous findings, we expected to find that all the risk factors were associated with physical aggression for both sexes, but based on inconsistencies in previous findings regarding sex differences, we did not have a hypothesis regarding sex differences in strength of association.
Method
Study Population and Design
The sample comprised 7567 adolescents (3686 boys and 3881 girls), who participated in a population-based survey in Norway. All residents in the age range of 13 to 19 years old (n = 10,464) in the county of Nord-Trøndelag were invited to participate in the adolescent part (Young-HUNT3) of The Trøndelag Health Study (HUNT3) from 2006 to 2008 (Holmen et al., 2014; Krokstad et al., 2013). The Trøndelag Health Study (HUNT) is a collaboration between HUNT Research Centre, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology (NTNU), Trøndelag County Council, Central Norway Regional Health Authority, and the Norwegian Institute of Public Health. A comprehensive questionnaire was administered in a school setting (original questionnaire in English language is available here: https://www.ntnu.edu/hunt/data/que). Adolescents outside the school system or not in school on the day the questionnaire was administered were invited to participate through mail. The response rate for the self-report questionnaire was 78% (n = 8200). Participants who did not provide an answer to the question about physical fighting—the primary dependent variable in this study—were excluded from data analyses (n = 633). Participation in the Young-HUNT study was voluntary, and written consent was required. Specifically, for participants below 16 years of age, parents had to provide written consent. A Data Protection Impact Assessment (DPIA) has been conducted and approved by The Norwegian University of Science and Technology (NTNU). Ethics approval was given by the Regional Committee for Medical and Health Research Ethics (REK) in Norway (2017/1208/REK-midt).
Measures
Dependent variable
Physical aggression was assessed with one item measuring participation in physical fighting. Participants were asked if they had been in a physical fight using a 4-point response scale including Never, Sometimes, Often, or Very often. Although the time frame for participating in physical fights was not specified, this item was embedded in a questionnaire about family, social, and health-related issues, queried for the period of the past 12 months. Of the 7567 participants, 47 participants (0.6%) endorsed Very Often, 86 participants (1.1%) endorsed Often, 773 participants (10.2%) endorsed Sometimes, and 6661 participants (88.0%) endorsed Never. Due to the highly skewed distribution, the physical aggression variable was dichotomized as No aggression for all participants who responded Never and Physical aggression for all participants who endorsed any other response category (i.e., Sometimes, Often, or Very often). The item was part of the 14-item School Adjustment Questionnaire, assessing behavior at school or in relation to school, designed by the Norwegian Institute of Public Health. Factor analysis of the 14-item questionnaire has revealed three factors “Academic problems” (highest loading item: I have problems concentrating in class), “Conduct problems” (highest loading item: I am reprimanded by my teacher), and “Dissatisfaction with school” (highest loading item: I look forward to going to school) (Storksen et al., 2006). Several studies have used the total or subscale scores of the School Adjustment Questionnaire from the HUNT study in research of adolescent mental and physical health (Blaauw et al., 2015; Skrove et al., 2015; Storksen et al., 2006; Strandheim et al., 2009). Our rationale for conducting a separate analysis with the physical aggression item (rather than the conduct problems subscale) was that, if present, physical aggression constitutes a distinct and significant problem in adolescence that requires a focused investigation.
Independent variables
Symptoms of anxiety and depression were assessed using a previously validated 5-item scale (SCL-5) (Strand et al., 2003; Tambs & Moum, 1993) derived from the 25-item Hopkins Checklist for Anxiety and Depression (SCL-25). Participants were asked to indicate on a 4-point scale, from Never to Very often, how much they had been bothered during the last 14 days by the following symptoms: Been constantly afraid and anxious, Felt tense or uneasy, Felt hopelessness when you think of the future, Felt dejected or sad, and Worried too much about various things. A mean of the items was computed, with higher scores indicating more symptoms of anxiety and depression. Cronbach’s alpha for the internalizing problem scale was 0.83.
Loneliness was assessed with one item: Do you feel lonely? with a 5-point response scale with the alternatives: Very often, Often, Sometimes, Seldom, and Very seldom or never.
Self-esteem was assessed using a 4-item shortened version of the 10-item Rosenberg Self-Esteem Scale (Rosenberg, 1965). The original scale is shown to have good psychometric qualities (Alessandri et al., 2015). Participants were asked to rate on a 4-point response scale, from Strongly agree to Strongly disagree the following items: I take a positive attitude towards myself (reverse-scored), I certainly feel useless at times, I feel I do not have much to be proud of, and I feel that I’m a person of worth, at least on an equal plane with others (reverse-scored). A mean of the items was computed, with higher scores indicating lower self-esteem. Cronbach’s alpha for the self-esteem scale was 0.77.
Attention problems were assessed by two items: Have difficulties concentrating during class and Can’t manage to be calm/sit still during class, rated on a 4-point scale from Never to Very often. The items were part of the 14-item School Adjustment Questionnaire, and previously validated as a meaningful factor (Skrove et al., 2015; Strandheim et al., 2009). A mean of the items was computed, with higher scores indicating more attention difficulties. Cronbach’s alpha for attention problems was 0.62.
Exposure to traumatic events was assessed by an 11-item scale based on The University of California at Los Angeles Post-traumatic Stress Disorder Reaction Index (UCLA PTSD Reaction Index) (Steinberg et al., 2004). Participants were asked if they had any of the following 11 events happen to them during their lifetime: That someone in your family has been seriously ill, Death of a loved one, A catastrophe, A serious accident, Been violently hurt, Been put in sexually uncomfortable/abusive situations by someone about your age, Been put in sexually uncomfortable situations by an adult, Been threatened or physically harassed by other students at school for a long time, Received painful or frightening treatment at the hospital while being treated for an illness or an injury, and Experienced something else that was very frightening, dangerous or violent. The three response categories were: No, Yes, last year and Yes, in my life. The variable was dichotomized into No, not experienced and Yes, experienced in a lifetime (Yes, last year or Yes, in my life). A total number of types of traumatic events experienced in a lifetime was computed with a possible range from 0 to 11 events. Cronbach’s alpha for the trauma exposure scale was 0.67. Participants who responded Yes to ever experiencing any traumatic events were further asked: Do you still think much about what happened with Yes and No response categories. The question referred to traumatic experience in general, not a specific event. If the participant responded Yes, they were further asked the following three questions with Yes and No response categories: Do you have frightening thoughts, see images or hear sounds from the actual experience even when you don’t want to?, When something reminds you about what happened do you become distant, afraid or sad?, and Do you try to avoid talking about it, thinking about it or feel any feelings about what happened? A sum score of the symptoms of PTSD, corresponding to these last three questions, was created with a possible range from 0 to 3 symptoms. Cronbach’s alpha for the PTSD symptom scale was 0.64.
Substance use was assessed by items on alcohol intoxication and narcotic exposure. Participants were asked if they ever had drunk so much alcohol that they had felt intoxicated, with the response categories: No, never, Yes, once, Yes, 2-3 times, Yes, 4-10 times, and Yes, more than 10 times. Responses were categorized into: Never been drunk, Been drunk 1-10 times and Been drunk more than 10 times (Skrove et al., 2013; Strandheim et al., 2009). Participants were asked if they ever had tried hash, marijuana, or other drugs, with the response categories Yes and No. In Norway, the legal age for buying beer and wine is 18 years old, and it is 20 years old for spirits. The use of narcotics is illegal.
Demographic variables
Information on sex and date of birth was collected from the Norwegian National Population Registry. Participants’ ages were calculated by subtracting date of birth from date of questionnaire completion. Family socioeconomic status (SES) was assessed with one item asking how well off the participants thought their family was compared to others, with the response categories: About the same as others, Better financial situation, and Worse financial situation. The variable was dichotomized into About the same or better financial situation and Worse financial situation.
Analyses
Descriptive data are first presented for the whole study population (Table 1) and then presented according to reporting on the dependent variable, physical fighting (Table 2). Counts and percentages are presented for categorical variables and means and SDs for continuous variables. Sex differences were assessed with Student’s t test for continuous variables and Pearson’s chi square test for categorical variables.
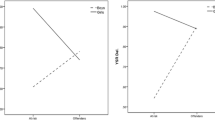
Logistic regression was used to calculate odds ratios (ORs) and 95% confidence intervals (CI) for the associations between each of the independent variables and the dependent variable, physical fighting. Separate analyses were conducted for the total sample, boys only, and girls only. For the total sample, the independent variables were examined one at a time, controlling for age, sex, and family SES (Table 3, Total Sample—Model 1). Next, an interaction term between sex and each of the independent variables was added and examined individually to examine possible sex differences (Table 3, Total Sample—Model 1 with Interactions). Logistic regression provides effect measures on a multiplicative scale. Interactions on a multiplicative scale imply that the combined effect is larger, or smaller, than the product of the individual effects, while interactions on an additive scale imply that the combined effect of two exposures is larger, or smaller, than the sum of the individual effects (Knol et al., 2011). Margin plots illustrating the probability of physical fighting were derived from the analyses including interactions and only plotted for the variables showing statistically significant sex interactions (Fig. 1). In the analyses conducted separately by sex, the independent variables were first examined independently, only adjusted for age and family SES (Table 3, Boys/Girls—Model 1). Next, in order to examine potential unique effects of the independent variables, the variables were examined together in a fully adjusted model (Table 3, Boys/Girls—Model 2). We report Nagelkerke R2 for the logistic regression model.

Margins plot illustrating probability of physical fighting by risk factors for boys and girls. Note. Derived from logistic regression with sex interaction terms, for physical fighting as dependent variable and attention problems (a), anxiety and depression problems (b), loneliness (c), traumatic events (d), alcohol intoxication (e), and tried narcotics (f) as independent variables examined individually, controlling for age and family SES
Missing values were handled by available case analysis. This means that in each analysis, cases with available data for that particular analysis were included. Handling missing data using available case analysis was considered appropriate given the low proportions of missing values in our study. We report estimates with 95% confidence intervals (CI) where relevant, and we regard two-sided p values under 0.05 to indicate statistical significance. While our criterion for statistical significance was two-sided p values < 0.05, due to multiple hypotheses, p values greater than 0.01 should be interpreted with caution.
All statistical analyses were conducted using Stata for Windows, version 16 (Stata Corp, College Station, TX, USA).
Results
Characteristics of the Study Sample
Characteristics of the study sample are presented in Table 1. The mean age for boys was 15.9 years (SD 1.73) and for girls 16.0 years (SD 1.76). Twenty-one percent (n = 773) of boys and 3.4% (n = 133) of girls reported engaging in physical fights. Sex differences were found for six of the nine independent variables: anxiety and depression, loneliness, self-esteem problems, PTSD symptoms, alcohol intoxication, and tried narcotics (Table 1). Girls had higher mean levels of anxiety and depression, self-esteem problems, loneliness, and PTSD symptoms than boys, while boys had higher percentages for alcohol intoxication over 10 times and having tried narcotics than girls.
Characteristics for the study sample, grouped by physical aggression and no physical aggression, are presented in Table 2. Sex differences were indicated for all the independent variables in the physical aggression group, except for having tried narcotics (Table 2). Physically aggressive girls, compared to physically aggressive boys, had higher mean levels of attention problems, anxiety and depression, self-esteem problems, loneliness, traumatic events, and PTSD symptoms, and a higher percentage of the girls than boys had been drunk between 1 and 10 times, and more than 10 times.
Mental Health and Physical Aggression
Results from the logistic regression analyses are presented in Table 3. All included mental health variables: attention problems, anxiety and depression, self-esteem problems, and loneliness, were associated with physical aggression in the total sample and then separately for boys and girls (Table 3, Total sample/Boys/Girls—Model 1). ORs derived from these analyses reflect the odds of engaging in physical fighting per one unit increase on the independent variable. Interaction effects with sex were indicated for all the variables except for self-esteem problems (Table 3, Total Sample—Model 1 with Interactions). Separate analyses for boys and girls indicated larger ORs for girls (Table 3, Boys/Girls—Model 1), implying stronger associations for girls than for boys. For a one unit increase on the attention problem scale, the odds of physical fighting increased by 228% for girls (OR = 3.28 [CI 2.59–4.14]) and 134% for boys (OR = 2.34 [2.08–2.64]); for a one unit increase on the anxiety and depression scale, the odds increased by 158% for girls (OR = 2.58 [2.02–3.29]) and 85% for boys (OR = 1.85 [1.56–2.20]); and for a one unit increase on the loneliness scale, the odds of physical fighting increased by 56% for girls (OR = 1.56 [1.34–1.82]) and 27% for boys (OR = 1.27 [1.17–1.37]). The margin plots illustrate the probability of physical fighting by attention problems (Fig. 1a), anxiety and depression (Fig. 1b), and loneliness (Fig. 1c) for each sex. Although the analyses separated by sex indicate higher ORs for girls than for boys, the margin plots, based on the sex interaction analyses, show that the probability of physical fighting increases more for boys than for girls, per unit increase on each independent variable. For example, an increase on the attention scale from 2 to 3 increased the probability of physical fighting by 0.16 (from 0.20 to 0.36) for boys and 0.05 (from 0.03 to 0.08) for girls. Whereas odds reflect the ratio between the occurrence of an event to the non-occurrence of the event, probabilities reflect the occurrence of an event relative to the total number of events. Here, the probabilities are larger, and the margin plot curves are steeper for boys due to the higher prevalence of physical fighting for boys. In other words, while these mental health variables increased the relative risk of physical fighting more for girls than boys, the effect on overall probability of engaging in physical fighting was greater for boys. In the fully adjusted model for both sexes, only attention problems remained statistically significant, while the associations with the other mental health variables became non-significant (Table 3, Boys/Girls—Model 2).
Trauma and Physical Aggression
Experience of traumatic events and PTSD symptoms were associated with physical aggression in the total sample and in the separate analyses for each sex (Table 3, Total sample/Boys/Girls—Model 1). Interaction effects with sex were indicated for exposure to traumatic events but not for PTSD symptoms (Table 3, Total Sample—Model 1 with Interactions). Separate analyses by sex indicated larger ORs for girls for exposure to traumatic events (Table 3, Boys/Girls Model 1), implying a higher relative effect for girls than for boys. For every additional experience of type of traumatic event, the odds of physical fighting increased by 51% for girls (OR = 1.51 [1.39–1.65]) and 34% for boys (OR = 1.34 [1.28–1.40]). The margin plot (Fig. 1d) based on the sex interaction analyses illustrates the probability of physical fighting by experience of traumatic events for each sex. Although the ORs are higher for girls than for boys in the separate analyses by sex, the plot shows that the probability of physical fighting increased more for boys experiencing one additional type of traumatic event than for girls. For example, an increase from 5 to 6 traumatic events increased the probability of physical fighting by 0.06 (from 0.36 to 0.42) for boys and 0.04 (from 0.07 to 0.11) for girls. This is due to the higher prevalence of physical fighting in boys. Traumatic events remained statistically significant in the fully adjusted model for boys and girls, while the association with PTSD symptoms remained statistically significant only for boys (Table 3, Boys/Girls—Model 2).
Substance Use and Physical Aggression
Alcohol intoxication in adolescence, both intoxication between 1–10 times and above 10 times, and having tried narcotics, were strongly associated with physical aggression in the total sample, and for boys and girls separately (Table 3, Total sample/Boys/Girls—Model 1). Interaction effects with sex were indicated for both conditions of alcohol intoxication and for having tried narcotics (Table 3, Total Sample—Model 1 with Interactions). Separate analyses by sex indicated also here larger ORs for girls (Table 3, Boys/Girls—Model 1). Above 10 alcohol intoxications compared to none increased the odds of physical fighting by 1699% for girls (OR = 17.99 [8.43–38.40]) and 666% for boys (OR = 7.66 [5.51–10.63]). Having tried narcotics increased the odds of fighting by 526% for girls (OR = 6.26 [3.44–11.39]) and 235% for boys (OR = 3.35 [2.37–4.74]). However, the confidence intervals for some of the variables were wider for girls than for boys, indicating less certainty in measurements. Margin plots based on the sex interaction analyses illustrate the probability of physical fighting by alcohol intoxication (Fig. 1e) and having tried narcotics (Fig. 1f). For example, the probability of physical fighting for boys who had more than 10 alcohol intoxications was 0.42, while it was 0.12 for girls. The graphs are steeper for boys for both variables, as would be expected due to the higher prevalence rate of physical aggression in boys. Alcohol intoxication, both conditions, and having tried narcotics remained statistically significant in the fully adjusted model for boys and girls (Table 3, Boys/Girls—Model 2).
Nagelkerke R2 for all the separate independent variables were in the range of 0.051 to 0.122 for boys (attention problems 0.122, anxiety and depression 0.057, self-esteem problems 0.057, loneliness 0.051, traumatic events 0.111, PTSD symptoms 0.061, alcohol intoxication 0.122, and tried narcotics 0.054), and in the range of 0.034 to 0.100 for girls (attention problems 0.100, anxiety and depression 0.059, self-esteem problems 0.034, loneliness 0.036, traumatic events 0.097, PTSD symptoms 0.063, alcohol intoxication 0.091, and tried narcotics 0.035). Nagelkerke R2 for the fully adjusted models was for boys 0.232 and for girls 0.263.
Taken together, these results indicate that, despite overall higher probabilities of engagement in physical fighting for boys, mental health concerns, trauma exposure, and substance use increase the relative risk of physical fighting more for girls than for boys.
Discussion
In this study, we used cross-sectional data from the Young-HUNT3 study to examine boys’ and girls’ concurrent associations between physical fighting and mental health problems, trauma exposure, and substance use. Our results indicated that inattention, anxiety and depression symptoms, self-esteem problems, loneliness, exposure to traumatic events, PTSD symptoms, alcohol intoxication, and having tried narcotics were associated with physical fighting in the total sample, as well as for boys and girls separately. Interaction effects for sex were indicated for all the variables except self-esteem problems and PTSD symptoms. In separate analyses for boys and girls, the clear tendency was that the odds ratios for all potential risk factor variables were higher for girls than for boys, indicating stronger associations for girls.
Consistent with previous studies (Arata et al., 2007; Bachman & Peralta, 2002; Dutton & Karakanta, 2013; Fontaine et al., 2008; Marsee, 2008; Reed et al., 2017), our results indicated that mental health symptoms, traumatic experiences, and substance use were associated with an increased risk of physical aggression in adolescents. The major goal of our study was to expand the understanding of sex differences in these associations. Based on both previous studies (Archer, 2004; Kann et al., 2018; Nivette et al., 2019), and our study, we know that boys engage in physical fighting more often than girls. Twenty-one percent of boys and three percent of girls reported participating in physical fighting in our study. Compared to the rates in the study by Kann et al. (2018), where 30 percent of boys and 17 percent of girls reported participating in physical fighting, our rates are somewhat lower. Our results indicated that on a multiplicative scale, the associations between attention problems, anxiety and depression, being lonely, experiencing traumatic events, and alcohol and narcotic use and physical fighting were stronger for girls than for boys. Our results are consistent with previous findings of a sex difference in the associations of physical fighting with anxiety and depression and with loneliness (Benarous et al., 2015; Storch et al., 2004). The results also supported a sex difference in the association with attention problems, although in the opposite direction of the findings by Ruchkin et al. (2008). Differences in attention measurements could be a possible explanation for this discrepancy, as the present study assessed attention problems while Ruchkin et al. (2008) assessed ADHD. With regard to traumatic experiences, the risk of physical aggression increased more for girls than for boys for each additional type of traumatic event (51% increase in odds for girls and 34% increase for boys), in contrast to the findings in the Duke et al. (2010) study (60% increase in odds for girls and 65% increase for boys). The trauma scale used in the present study assessed 11 different traumatic events, while the trauma scale in their study assessed only six events, focusing on abuse and household dysfunction, a difference that could have affected the results. Further, substance use in adolescence, both heavy drinking and narcotics use, showed strong associations for both sexes, but especially for girls (OR = 18 for alcohol intoxication > 10, and OR = 6 for tried narcotics). This is in contrast to the findings by Quinn et al. (2013), who also examined relative effects but found a stronger association between alcohol drinking and aggression for boys. Differences between the Quinn et al. (2013) study and the present study included age range of participants, measurement of alcohol use, and operational definition of aggression. Our study did find a significant sex effect for narcotics use, unlike previous studies (Bachman & Peralta, 2002; Swahn & Donovan, 2004), which did not find such an effect.
Physical aggression was more prevalent in boys, and, as illustrated in the margin plots (Fig. 1), increases in risk factors were associated with higher absolute risk differences for boys. However, comparing only absolute probabilities prevents an understanding of relative effects of risk factors and how these risk factors differentially impact girls. Examining sex differences with relative effect measurements, and showing probability plots of physical aggression by sex, as we did, provides an important and more nuanced understanding of how key risk factors for physical aggression operate differently for boys and for girls.
Risk factors of aggression that were investigated in this study - symptoms of psychopathology, trauma exposure, and substance use - are likely to co-occur. In the fully adjusted model, all independent variables were entered simultaneously to identify unique effects of the different variables. The association with attention problems, experiencing traumatic events, and substance use remained statistically significant for both boys and girls, and PTSD symptoms only for boys, while the other associations became non-significant. The strong association between attention problems and physical aggression is consistent with previous findings (Fontaine et al., 2008; Reed et al., 2017), as is the association with substance use (Bachman & Peralta, 2002; Swahn & Donovan, 2004; Tomlinson et al., 2016) and alcohol consumption in particular (Kivimäki et al., 2014; Quinn et al., 2013; Robertson et al., 2020). The finding of a unique association between trauma exposure and physical fighting is also consistent with previous findings of traumatic events predicting physical aggression (Arata et al., 2007; Marsee, 2008). Leban and Gibson (2020) found that ACEs affected delinquent behavior only for boys, while our results showed that both boys’ and girls’ physically aggressive behaviors were associated with ACEs. However, different aggression measurements, delinquent behavior versus physical fighting, between the two studies complicate a direct comparison. In the fully adjusted model for boys in our study, PTSD symptoms remained statistically significant, while the association became non-significant for girls. This is in line with the findings of Aebi et al. (2017) that the effect of experiencing traumatic events on physical aggression was mediated through PTSD symptoms only for boys. Our finding that anxiety and depression, loneliness, and self-esteem became non-significant in the fully adjusted model indicates that these risk factors were related to, but did not exert a unique association with physical aggression. This is consistent with previous findings showing ambiguous associations between mental health factors and aggression (Hatfield & Dula, 2014; Murray et al., 2018; Schinka et al., 2013; Stickley et al., 2014; Walker & Gudjonsson, 2006). However, precautions must be taken when interpreting the fully adjusted models in our study. Including all variables in a fully adjusted model could introduce unwanted collider biases (Rothman, 2012), limiting the validity of the results.
Physical fighting has long been considered a separate and particularly troublesome dimension of disruptive behavioral problems (Bolhuis et al., 2017; Loeber & Hay, 1994). It is shown to lead to detrimental and long-lasting individual and societal costs, as physical aggression in childhood and adolescence is shown to be a strong predictor of adolescent delinquency and adult criminality (Huesmann et al., 2009, 2002; Nagin & Tremblay, 1999; Pingault et al., 2013). Mental health disorders associated with aggression and/or impulsivity have been identified as the strongest predictor of both juvenile delinquency and recidivism (Barrett et al., 2014), and, specifically, in juvenile justice samples of girls (Barrett et al., 2015). In our study, mental health variables were associated with an increased risk of physical fighting for both sexes, although the associations were found to be stronger for girls than for boys. Thus, screening for mental health difficulties and providing appropriate treatment services should be an important step to prevent both physical fighting and delinquency, and it is particularly needed for girls at risk for delinquency.
Considerable progress has been made during the last decades in the development and implementation of evidence-based psychosocial treatments targeting aggression and prevention of juvenile delinquency (Eyberg et al., 2008; McCart & Sheidow, 2016; Sukhodolsky & Ruchkin, 2006). Multiple intervention approaches have been developed, including Multisystemic Therapy (MST) (Henggeler et al., 2009), Functional Family Therapy (FFT) (Alexander & Robbins, 2010), Parent Management Training (PMT) (Forgatch & Patterson, 2010), school-based Fast Track prevention program (Bierman et al., 2019), and cognitive-behavioral therapy for anger and aggression in children and adolescents (Sukhodolsky & Scahill, 2012). These interventions differ in their relative emphasis on child skills for regulating emotions and problem-solving or on caregiver skills of recognizing and rewarding positive behaviors and improving parent-child interaction. Other multi-component approaches offer system-based and ecological interventions that incorporate parents, peers, school, and community factors. Given that aggression is associated with risk factors at different social-ecological levels (Bronfenbrenner, 1979; Farrington et al., 2017), the complexity of problem behaviors should be considered when selecting interventions in clinical or community settings, as multi-component interventions are more likely needed for more complex and serious forms of conduct problems (Berg et al., 2020; Frick et al., 2014; McCart & Sheidow, 2016).
Implications
Several interventions have been shown to reduce violence in adolescence (Eyberg et al., 2008; McCart & Sheidow, 2016; McGuire, 2008), and it is, therefore, important to assess relevant risk factors and identify adolescents at risk as early as possible. The results of our study indicate that interventions aimed at reducing physical fighting in adolescence should carefully evaluate attentional problems, history of substance use, and history of exposure to trauma. Underage drinking, and especially heavy alcohol use, has shown strong associations with physical aggression, and, in the context of other negative consequences of adolescent drinking, such as dependency and neurocognitive deficits (Marshall, 2014; Zeigler et al., 2005), reducing underage drinking should be a target for policy-makers. Physical fighting is more prevalent in boys, and, not surprisingly, many treatment studies have been conducted in samples with a higher number of male than female participants. In our study, several of the risk factors showed a stronger association with aggression in adolescent girls compared to boys. The findings suggest that programs that offer treatments for young girls with ADHD symptoms, trauma experiences, and substance use, may help reduce the probability of physically aggressive behavior later in adolescence.
Limitations
The main limitation of our study is that our dependent variable, physical aggression, was based on only one item measuring participation in physical fighting. Although we do not have data on the reliability of the one-item measure of physical aggression in this study, acceptable levels of test-retest reliability of physical aggression have been demonstrated in studies using more nuanced measures of physical aggression (Coccaro et al., 1997; Webster et al., 2014, 2015). Other forms of physical aggression were not assessed in this study, which may have contributed to the lower prevalence of physical aggression. Also, previous empirical findings on the association between depression and aggression are more consistent than previous findings on the relationship between anxiety and aggression (Dutton & Karakanta, 2013; Hatfield & Dula, 2014; Murray et al., 2018), and a combined scale of the two constructs (anxiety and depression) could have affected the results. Additionally, none of the variables or scales from the Young-HUNT3 questionnaire have diagnostic precision. Some of the scales are shortened versions of original screening instruments, e.g., SCL-5 and 4-item Rosenberg Self-Esteem Scale. Another limitation is that all data were collected by self-report, and shared method variance could have affected the results. Lastly, the study is based on a cross-sectional sample, precluding causal interpretations of the effects of the investigated risk factors on physical aggression.
Conclusion
Our study aimed to expand the understanding of boys’ and girls’ physical fighting in adolescence using a large non-clinical sample. We identified several associations between physical aggression and mental health problems, trauma exposure, and substance use for boys and girls and found several significant sex effects. The results indicate that boys’ and girls’ physically aggressive behaviors are associated mainly with the same risk factors. However, the associations between physical aggression and inattention, anxiety and depression, loneliness, trauma exposure, alcohol intoxication, and narcotics use were stronger for girls than for boys. The findings further our understanding of sex differences in physical aggression in adolescence and can be used to improve clinical and societal interventions aimed at reducing or preventing aggressive behavior and its consequences.
References
Aebi, M., Mohler-Kuo, M., Barra, S., Schnyder, U., Maier, T., & Landolt, M. A. (2017). Posttraumatic stress and youth violence perpetration: A population-based cross-sectional study. European Psychiatry, 40, 88–95. https://doi.org/10.1016/j.eurpsy.2016.08.007
Alessandri, G., Vecchione, M., Eisenberg, N., & Laguna, M. (2015). On the factor structure of the Rosenberg (1965) general self-esteem scale. Psychological Assessment, 27(2), 621–635. https://doi.org/10.1037/pas0000073
Alexander, J. F., & Robbins, M. S. (2010). Functional family therapy. In R. C. Murrihy, A. D. Kidman, & T. H. Ollendick (Eds.), Clinical handbook of assessing and treating conduct problems in youth (pp. 245–271). Springer. https://doi.org/10.1007/978-1-4419-6297-3_10
Arata, C. M., Langhinrichsen-Rohling, J., Bowers, D., & O’Brien, N. (2007). Differential correlates of multi-type maltreatment among urban youth. Child Abuse & Neglect, 31(4), 393–415. https://doi.org/10.1016/j.chiabu.2006.09.006
Archer, J. (2004). Sex differences in aggression in real-world settings: A meta-analytic review. Review of General Psychology, 8(4), 291–322. https://doi.org/10.1037/1089-2680.8.4.291
Arnett, A. B., Pennington, B. F., Willcutt, E. G., DeFries, J. C., & Olson, R. K. (2015). Sex differences in ADHD symptom severity. Journal of Child Psychology and Psychiatry, 56(6), 632–639. https://doi.org/10.1111/jcpp.12337
Bachman, R., & Peralta, R. (2002). The relationship between drinking and violence in an adolescent population: Does gender matter? Deviant Behavior, 23(1), 1–19. https://doi.org/10.1080/016396202317192008
Baglivio, M. T., Epps, N., Swartz, K., Huq, M. S., Sheer, A., & Hardt, N. S. (2014). The prevalence of adverse childhood experiences (ACE) in the lives of juvenile offenders. Journal of Juvenile Justice, 3(2). https://www.prisonpolicy.org/scans/Prevalence_of_ACE.pdf
Baillargeon, R. H., Zoccolillo, M., Keenan, K., Côté, S., Pérusse, D., Wu, H.-X., Boivin, M., & Tremblay, R. E. (2007). Gender differences in physical aggression: A prospective population-based survey of children before and after 2 years of age. Developmental Psychology, 43(1), 13 https://doi.org/10.1037/0012-1649.43.1.13
Barrett, D. E., Ju, S., Katsiyannis, A., & Zhang, D. (2015). Females in the juvenile justice system: Influences on delinquency and recidivism. Journal of Child and Family Studies, 24(2), 427–433. https://doi.org/10.1007/s10826-013-9853-8
Barrett, D. E., Katsiyannis, A., Zhang, D., & Zhang, D. (2014). Delinquency and recidivism: A multicohort, matched-control study of the role of early adverse experiences, mental health problems, and disabilities. Journal of Emotional and Behavioral Disorders, 22(1), 3–15. https://doi.org/10.1177/1063426612470514
Benarous, X., Hassler, C., Falissard, B., Consoli, A., & Cohen, D. (2015). Do girls with depressive symptoms exhibit more physical aggression than boys? A cross sectional study in a national adolescent sample. Child and Adolescent Psychiatry and Mental Health, 9(1), 41 https://doi.org/10.1186/s13034-015-0064-5
Berg, R. C., Johansen, T. B., Jardim, P. S. J., Forsetlund, L., & Nguyen., L. (2020). Tiltak for barn og unge med atferdsvansker eller som har begått kriminelle handlinger: en oversikt over systematiske oversikter. [Interventions for children and youth with behavioral problems or criminal behavior: an overview of reviews]. Folkehelsinstituttet. https://www.fhi.no/en/publ/2020/Interventions-for-children-and-youth-with-behavioral-problems-or-criminal-behavior/
Bierman, K. L., Coie, J. D., Dodge, K. A., Greenberg, M. T., Lochman, J. E., McMahon, R. J., & Pinderhughes, E. E. (2019). The Fast Track program for children at risk: Preventing antisocial behavior. Guilford Publications
Blaauw, B. A., Dyb, G., Hagen, K., Holmen, T. L., Linde, M., Wentzel-Larsen, T., & Zwart, J.-A. (2015). The relationship of anxiety, depression and behavioral problems with recurrent headache in late adolescence–a Young-HUNT follow-up study. The Journal of Headache and Pain, 16(1), 10 https://doi.org/10.1186/1129-2377-16-10
Bolhuis, K., Lubke, G. H., van der Ende, J., Bartels, M., van Beijsterveldt, C. E. M., Lichtenstein, P., Larsson, H., Jaddoe, V. W. V., Kushner, S. A., Verhulst, F. C., Boomsma, D. I., & Tiemeier, H. (2017). Disentangling heterogeneity of childhood disruptive behavior problems into dimensions and subgroups. Journal of the American Academy of Child and Adolescent Psychiatry, 56(8), 678–686. https://doi.org/10.1016/j.jaac.2017.05.019
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Harvard University Press
Card, N. A., Stucky, B. D., Sawalani, G. M., & Little, T. D. (2008). Direct and indirect aggression during childhood and adolescence: A meta-analytic review of gender differences, intercorrelations, and relations to maladjustment. Child Development, 79(5), 1185–1229. https://doi.org/10.1111/j.1467-8624.2008.01184.x
Cleverley, K., Szatmari, P., Vaillancourt, T., Boyle, M., & Lipman, E. (2012). Developmental trajectories of physical and indirect aggression from late childhood to adolescence: Sex differences and outcomes in emerging adulthood. Journal of the American Academy of Child and Adolescent Psychiatry, 51(10), 1037–1051. https://doi.org/10.1016/j.jaac.2012.07.010
Coccaro, E. F., Berman, M. E., & Kavoussi, R. J. (1997). Assessment of life history of aggression: Development and psychometric characteristics. Psychiatry Research, 73(3), 147–157. https://doi.org/10.1016/S0165-1781(97)00119-4
Connor, D. F., Newcorn, J. H., Saylor, K. E., Amann, B. H., Scahill, L., Robb, A. S., Jensen, P. S., Vitiello, B., Findling, R. L., & Buitelaar, J. K. (2019). Maladaptive aggression: With a focus on impulsive aggression in children and adolescents. Journal of Child and Adolescent Psychopharmacology, 29(8), 576–591. https://doi.org/10.1089/cap.2019.0039
Cote, S. M., Vaillancourt, T., LeBlanc, J. C., Nagin, D. S., & Tremblay, R. E. (2006). The development of physical aggression from toddlerhood to pre-adolescence: A nation wide longitudinal study of Canadian children. Journal of Abnormal Child Psychology, 34(1), 71–85. https://doi.org/10.1007/s10802-005-9001-z
D’zurilla, T. J., Chang, E. C., & Sanna, L. J. (2003). Self-esteem and social problem solving as predictors of aggression in college students. Journal of Social and Clinical Psychology, 22(4), 424–440. https://doi.org/10.1521/jscp.22.4.424.22897
Donnellan, M. B., Trzesniewski, K. H., Robins, R. W., Moffitt, T. E., & Caspi, A. (2005). Low self-esteem is related to aggression, antisocial behavior, and delinquency. Psychological Science, 16(4), 328–335. https://doi.org/10.1111/j.0956-7976.2005.01535.x
Duke, N. N., Pettingell, S. L., McMorris, B. J., & Borowsky, I. W. (2010). Adolescent violence perpetration: associations with multiple types of adverse childhood experiences. Pediatrics, 125(4), e778–e786. https://doi.org/10.1542/peds.2009-0597
Dutton, D. G., & Karakanta, C. (2013). Depression as a risk marker for aggression: A critical review. Aggression and Violent Behavior, 18(2), 310–319. https://doi.org/10.1016/j.avb.2012.12.002
Eyberg, S. M., Nelson, M. M., & Boggs, S. R. (2008). Evidence-based psychosocial treatments for children and adolescents with disruptive behavior. Journal of Clinical Child and Adolescent Psychology, 37(1), 215–237. https://doi.org/10.1080/15374410701820117
Farrington, D. P., Gaffney, H., & Ttofi, M. M. (2017). Systematic reviews of explanatory risk factors for violence, offending, and delinquency. Aggression and Violent Behavior, 33, 24–36. https://doi.org/10.1016/j.avb.2016.11.004
Fontaine, N., Carbonneau, R., Barker, E. D., Vitaro, F., Hebert, M., Cote, S. M., Nagin, D. S., Zoccolillo, M., & Tremblay, R. E. (2008). Girls’ hyperactivity and physical aggression during childhood and adjustment problems in early adulthood: a 15-year longitudinal study. Archives of General Psychiatry, 65(3), 320–328. https://doi.org/10.1001/archgenpsychiatry.2007.41
Forgatch, M., & Patterson, G. (2010). Parent management training—Oregon model: An intervention for antisocial behavior in children and adolescents In J. Weisz & A. Kazdin (Eds.), Evidence-based psychotherapies for children and adolescents. Guilford Press
Frick, P. J., Ray, J. V., Thornton, L. C., & Kahn, R. E. (2014). Annual research review: A developmental psychopathology approach to understanding callous-unemotional traits in children and adolescents with serious conduct problems. Journal of Child Psychology and Psychiatry, 55(6), 532–548. https://doi.org/10.1111/jcpp.12152
Froyland, L. R., & von Soest, T. (2020). Adolescent boys’ physical fighting and adult life outcomes: Examining the interplay with intelligence. Aggressive Behavior, 46(1), 72–83. https://doi.org/10.1002/ab.21871
Galambos, N. L., Barker, E. T., & Almeida, D. M. (2003). Parents do matter: Trajectories of change in externalizing and internalizing problems in early adolescence. Child Development, 74(2), 578–594. https://doi.org/10.1111/1467-8624.7402017
Hagquist, C. (2010). Discrepant trends in mental health complaints among younger and older adolescents in Sweden: An analysis of WHO data 1985–2005. Journal of Adolescent Health, 46(3), 258–264. https://doi.org/10.1016/j.jadohealth.2009.07.003
Hatfield, J., & Dula, C. S. (2014). Impulsivity and physical aggression: examining the moderating role of anxiety. The American Journal of Psychology, 127(2), 233–243. https://doi.org/10.5406/amerjpsyc.127.2.0233
Henggeler, S. W., Schoenwald, S. K., Borduin, C. M., Rowland, M. D., & Cunningham, P. B. (2009). Multisystemic therapy for antisocial behavior in children and adolescents. Guilford Press
Holmen, T. L., Bratberg, G., Krokstad, S., Langhammer, A., Hveem, K., Midthjell, K., Heggland, J., & Holmen, J. (2014). Cohort profile of the Young-HUNT Study, Norway: A population-based study of adolescents. International Journal of Epidemiology, 43(2), 536–544. https://doi.org/10.1093/ije/dys232
Huesmann, L. R., Dubow, E. F., & Boxer, P. (2009). Continuity of aggression from childhood to early adulthood as a predictor of life outcomes: Implications for the adolescent‐limited and life‐course‐persistent models. Aggressive Behavior: Official Journal of the International Society for Research on Aggression, 35(2), 136–149. https://doi.org/10.1002/ab.20300
Huesmann, L. R., Eron, L. D., & Dubow, E. F. (2002). Childhood predictors of adult criminality: are all risk factors reflected in childhood aggressiveness? Criminal Behaviour and Mental Health, 12(3), 185–208. https://doi.org/10.1002/cbm.496
Kann, L., McManus, T., Harris, W. A., Shanklin, S. L., Flint, K. H., Queen, B., Lowry, R., Chyen, D., Whittle, L., & Thornton, J. (2018). Youth risk behavior surveillance—United States, 2017. MMWR Surveillance Summaries, 67(8). https://doi.org/10.15585/mmwr.ss6708a1
Kassing, F., Godwin, J., Lochman, J. E., Coie, J. D., Bierman, K. L., Dodge, K. A., Greenberg, M. T., McMahon, R. J., & Pinderhughes, E. E., Conduct Problems Prevention Research, G. (2019). Using early childhood behavior problems to predict adult convictions [Article]. Journal of Abnormal Child Psychology, 47(5), 765–778. https://doi.org/10.1007/s10802-018-0478-7
Kivimäki, P., Kekkonen, V., Valtonen, H., Tolmunen, T., Honkalampi, K., Tacke, U., Hintikka, J., Lehto, S. M., & Laukkanen, E. (2014). Alcohol use among adolescents, aggressive behaviour, and internalizing problems. Journal of Adolescence, 37(6), 945–951. https://doi.org/10.1016/j.adolescence.2014.06.011
Knol, M. J., VanderWeele, T. J., Groenwold, R. H., Klungel, O. H., Rovers, M. M., & Grobbee, D. E. (2011). Estimating measures of interaction on an additive scale for preventive exposures. European Journal of Epidemiology, 26(6), 433–438. https://doi.org/10.1007/s10654-011-9554-9
Krokstad, S., Langhammer, A., Hveem, K., Holmen, T. L., Midthjell, K., Stene, T. R., Bratberg, G., Heggland, J., & Holmen, J. (2013). Cohort profile: The HUNT Study, Norway. International Journal of Epidemiology, 42(4), 968–977. https://doi.org/10.1093/ije/dys095
Lansford, J. E., Skinner, A. T., Sorbring, E., Giunta, L. D., Deater‐Deckard, K., Dodge, K. A., Malone, P. S., Oburu, P., Pastorelli, C., & Tapanya, S. (2012). Boys’ and girls’ relational and physical aggression in nine countries. Aggressive Behavior, 38(4), 298–308. https://doi.org/10.1002/ab.21433
Leban, L., & Gibson, C. L. (2020). The role of gender in the relationship between adverse childhood experiences and delinquency and substance use in adolescence. Journal of Criminal Justice, 66, 101637. https://doi.org/10.1016/j.jcrimjus.2019.101637
Loeber, R., & Hay, D. F. (1994). Developmental approaches to aggression and conduct problems. In M. Rutter & D. F. Hay (Eds.), Development through life: a handbook for clinicians (pp. 488–516). Blackwell Scientific Publications
Macmillan, R. (2001). Violence and the life course: The consequences of victimization for personal and social development. Annual Review of Sociology, 27(1), 1–22. https://doi.org/10.1146/annurev.soc.27.1.1
Marsee, M. A. (2008). Reactive aggression and posttraumatic stress in adolescents affected by Hurricane Katrina. Journal of Clinical Child & Adolescent Psychology, 37(3), 519–529. https://doi.org/10.1080/15374410802148152
Marshall, E. J. (2014). Adolescent alcohol use: risks and consequences. Alcohol Alcohol, 49(2), 160–164. https://doi.org/10.1093/alcalc/agt180
McCart, M. R., & Sheidow, A. J. (2016). Evidence-based psychosocial treatments for adolescents with disruptive behavior. Journal of Clinical Child and Adolescent Psychology, 45(5), 529–563. https://doi.org/10.1080/15374416.2016.1146990
McGuire, J. (2008). A review of effective interventions for reducing aggression and violence. Philosophical Transactions of the Royal Society B: Biological Sciences, 363(1503), 2577–2597. https://doi.org/10.1098/rstb.2008.0035
Merikangas, K. R., He, J.-p, Burstein, M., Swanson, S. A., Avenevoli, S., Cui, L., Benjet, C., Georgiades, K., & Swendsen, J. (2010). Lifetime prevalence of mental disorders in US adolescents: results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). Journal of the American Academy of Child & Adolescent Psychiatry, 49(10), 980–989. https://doi.org/10.1016/j.jaac.2010.05.017
Mokdad, A. H., Forouzanfar, M. H., Daoud, F., Mokdad, A. A., El Bcheraoui, C., Moradi-Lakeh, M., Kyu, H. H., Barber, R. M., Wagner, J., & Cercy, K. (2016). Global burden of diseases, injuries, and risk factors for young people’s health during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet, 387(10036), 2383–2401. https://doi.org/10.1016/S0140-6736(16)00648-6
Murray, A. L., Booth, T., Obsuth, I., Zirk-Sadowski, J., Eisner, M., & Ribeaud, D. (2018). Testing the exacerbation and attenuation hypotheses of the role of anxiety in the relation between ADHD and reactive/proactive aggression: A 10-year longitudinal study. Psychiatry Research, 269, 585–592. https://doi.org/10.1016/j.psychres.2018.08.120
Nagin, D., & Tremblay, R. E. (1999). Trajectories of boys’ physical aggression, opposition, and hyperactivity on the path to physically violent and nonviolent juvenile delinquency. Child Development, 70(5), 1181–1196. https://doi.org/10.1111/1467-8624.00086
Nivette, A., Sutherland, A., Eisner, M., & Murray, J. (2019). Sex differences in adolescent physical aggression: Evidence from sixty‐three low‐and middle‐income countries. Aggressive Behavior, 45(1), 82–92. https://doi.org/10.1002/ab.21799
Odgers, C. L., Moffitt, T. E., Broadbent, J. M., Dickson, N., Hancox, R. J., Harrington, H., Poulton, R., Sears, M. R., Thomson, W. M., & Caspi, A. (2008). Female and male antisocial trajectories: from childhood origins to adult outcomes. Development and Psychopathology, 20(2), 673–716. https://doi.org/10.1017/S0954579408000333
Pingault, J. B., Cote, S. M., Lacourse, E., Galera, C., Vitaro, F., & Tremblay, R. E. (2013). Childhood hyperactivity, physical aggression and criminality: a 19-year prospective population-based study. PLoS ONE, 8(5), e62594. https://doi.org/10.1371/journal.pone.0062594
Quinn, P. D., Stappenbeck, C. A., & Fromme, K. (2013). An event-level examination of sex differences and subjective intoxication in alcohol-related aggression. Experimental and Clinical Psychopharmacology, 21(2), 93 https://doi.org/10.1037/a0031552
Racz, S. J., & McMahon, R. J. (2011). The relationship between parental knowledge and monitoring and child and adolescent conduct problems: a 10-year update. Clinical Child and Family Psychology Review, 14(4), 377–398. https://doi.org/10.1007/s10567-011-0099-y
Reed, M. O., Jakubovski, E., Johnson, J. A., & Bloch, M. H. (2017). Predictors of long-term school-based behavioral outcomes in the multimodal treatment study of children with attention-deficit/hyperactivity disorder. Journal of Child and Adolescent Psychopharmacology, 27(4), 296–309. https://doi.org/10.1089/cap.2015.0168
Robertson, K., Forbes, S., & Thyne, M. (2020). Perpetration of alcohol-related aggression by male and female college students: An examination of overt and relational aggression. Journal of Interpersonal Violence, 35(5-6), 1454–1475. https://doi.org/10.1177/0886260517696872
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton University Press
Rothman, K. J. (2012). Epidemiology: an introduction. Oxford University Press
Ruchkin, V., Henrich, C. C., Jones, S. M., Vermeiren, R., & Schwab-Stone, M. (2007). Violence exposure and psychopathology in urban youth: The mediating role of posttraumatic stress. Journal of Abnormal Child Psychology, 35(4), 578–593. https://doi.org/10.1007/s10802-007-9114-7
Ruchkin, V., Lorberg, B., Koposov, R., Schwab-Stone, M., & Sukhodolsky, D. G. (2008). ADHD symptoms and associated psychopathology in a community sample of adolescents from the European north of Russia. Journal of Attention Disorders, 12(1), 54–63. https://doi.org/10.1177/1087054707305169
Schinka, K. C., van Dulmen, M. H., Mata, A. D., Bossarte, R., & Swahn, M. (2013). Psychosocial predictors and outcomes of loneliness trajectories from childhood to early adolescence. Journal of Adolescence, 36(6), 1251–1260. https://doi.org/10.1016/j.adolescence.2013.08.002
Skrove, M., Romundstad, P., & Indredavik, M. S. (2013). Resilience, lifestyle and symptoms of anxiety and depression in adolescence: the Young-HUNT study. Social Psychiatry and Psychiatric Epidemiology, 48(3), 407–416. https://doi.org/10.1007/s00127-012-0561-2
Skrove, M., Romundstad, P., & Indredavik, M. S. (2015). Chronic multisite pain in adolescent girls and boys with emotional and behavioral problems: the Young-HUNT study. European Child and Adolescent Psychiatry, 24(5), 503–515. https://doi.org/10.1007/s00787-014-0601-4
Steinberg, A. M., Brymer, M. J., Decker, K. B., & Pynoos, R. S. (2004). The University of California at Los Angeles Post-traumatic Stress Disorder Reaction Index. Current Psychiatry Reports, 6(2), 96–100. https://doi.org/10.1007/s11920-004-0048-2
Stickley, A., Koyanagi, A., Koposov, R., Schwab-Stone, M., & Ruchkin, V. (2014). Loneliness and health risk behaviours among Russian and US adolescents: a cross-sectional study. BMC Public Health, 14(1), 366. https://doi.org/10.1186/1471-2458-14-366
Storch, E. A., Bagner, D. M., Geffken, G. R., & Baumeister, A. L. (2004). Association between overt and relational aggression and psychosocial adjustment in undergraduate college students. Violence and Victims, 19(6), 689. https://doi.org/10.1891/vivi.19.6.689.66342.
Storksen, I., Roysamb, E., Holmen, T. L., & Tambs, K. (2006). Adolescent adjustment and well-being: Effects of parental divorce and distress. Scandinavian Journal of Psychology, 47(1), 75–84. https://doi.org/10.1111/j.1467-9450.2006.00494.x
Strand, B. H., Dalgard, O. S., Tambs, K., & Rognerud, M. (2003). Measuring the mental health status of the Norwegian population: a comparison of the instruments SCL-25, SCL-10, SCL-5 and MHI-5 (SF-36). Nordic Journal of Psychiatry, 57(2), 113–118. https://doi.org/10.1080/08039480310000932
Strandheim, A., Holmen, T. L., Coombes, L., & Bentzen, N. (2009). Alcohol intoxication and mental health among adolescents–a population review of 8983 young people, 13-19 years in North-Trondelag, Norway: The Young-HUNT Study. Child and Adolescent Psychiatry and Mental Health, 3(1), 18. https://doi.org/10.1186/1753-2000-3-18
Sukhodolsky, D. G., & Ruchkin, V. (2006). Evidence-based psychosocial treatments in the juvenile justice system. Child and Adolescent Psychiatric Clinics of North America, 15(2), 501–516, https://doi.org/10.1016/j.chc.2005.11.005
Sukhodolsky, D. G., & Scahill, L. (2012). Cognitive-behavioral therapy for anger and aggression in children. Guilford Press
Swahn, M. H., & Donovan, J. E. (2004). Correlates and predictors of violent behavior among adolescent drinkers. Journal of Adolescent Health, 34(6), 480–492. https://doi.org/10.1016/j.jadohealth.2003.08.018
Tambs, K., & Moum, T. (1993). How well can a few questionnaire items indicate anxiety and depression? Acta Psychiatrica Scandinavica, 87(5), 364–367. https://doi.org/10.1111/j.1600-0447.1993.tb03388.x
Thompson, E. L., & Farrell, A. D. (2019). Longitudinal relations between trauma‐related psychological distress and physical aggression among urban early adolescents. Journal of Clinical Psychology, 75(9), 1626–1642. https://doi.org/10.1002/jclp.22781
Tomlinson, M. F., Brown, M., & Hoaken, P. N. S. (2016). Recreational drug use and human aggressive behavior: A comprehensive review since 2003. Aggression and Violent Behavior, 27, 9–29. https://doi.org/10.1016/j.avb.2016.02.004
Tremblay, R. E. (2000). The development of agressive behaviour during childhood: What have we learned in the past century? International Journal of Behavioral Development, 24(2), 129–141. https://doi.org/10.1080/016502500383232
Tremblay, R. E. (2014). Early development of physical aggression and early risk factors for chronic physical aggression in humans. Current Topics in Behavioral Neurosciences, 17, 315–327. https://doi.org/10.1007/7854_2013_262
Underwood, M. K., Galenand, B. R., & Paquette, J. A. (2001). Top ten challenges for understanding gender and aggression in children: Why can’t we all just get along? Social Development, 10(2), 248–266. https://doi.org/10.1111/1467-9507.00162
Valois, R. F., MacDonald, J. M., Bretous, L., Fischer, M. A., & Drane, J. W. (2002). Risk factors and behaviors associated with adolescent violence and aggression. American Journal of Health Behavior, 26(6), 454–464. https://doi.org/10.5993/AJHB.26.6.6
Walker, J. S., & Gudjonsson, G. H. (2006). The Maudsley violence questionnaire: Relationship to personality and self-reported offending. Personality and Individual Differences, 40(4), 795–806. https://doi.org/10.1016/j.paid.2005.09.009
Webster, G. D., DeWall, C. N., Pond, Jr, R. S., Deckman, T., Jonason, P. K., Le, B. M., Nichols, A. L., Schember, T. O., Crysel, L. C., & Crosier, B. S. (2014). The brief aggression questionnaire: Psychometric and behavioral evidence for an efficient measure of trait aggression. Aggressive Behavior, 40(2), 120–139. https://doi.org/10.1002/ab.21507
Webster, G. D., DeWall, C. N., Pond, Jr, R. S., Deckman, T., Jonason, P. K., Le, B. M., Nichols, A. L., Schember, T. O., Crysel, L. C., & Crosier, B. S. (2015). The brief aggression questionnaire: Structure, validity, reliability, and generalizability. Journal of Personality Assessment, 97(6), 638–649. https://doi.org/10.1080/00223891.2015.1044093
Wells, S., Mihic, L., Tremblay, P. F., Graham, K., & Demers, A. (2008). Where, with whom, and how much alcohol is consumed on drinking events involving aggression? Event‐level associations in a Canadian national survey of university students. Alcoholism: Clinical and Experimental Research, 32(3), 522–533. https://doi.org/10.1111/j.1530-0277.2007.00596.x
Zeigler, D. W., Wang, C. C., Yoast, R. A., Dickinson, B. D., McCaffree, M. A., Robinowitz, C. B., & Sterling, M. L. (2005). The neurocognitive effects of alcohol on adolescents and college students. Preventive Medicine, 40(1), 23–32. https://doi.org/10.1016/j.ypmed.2004.04.044
Funding
This study is funded by the Department of Clinical and Molecular Medicine, Faculty of Medicine and Health Science, The Norwegian University of Science and Technology (NTNU). The study is part of a collaboration between NTNU and Yale University. M.H. has received travel grants for a study stay at Child Study Center, Yale University School of Medicine, from The Liaison Committee for Education, Research and Innovation in Central Norway and from Fulbright Norway. Open access funding provided by NTNU Norwegian University of Science and Technology (incl St. Olavs Hospital - Trondheim University Hospital).
Author information
Authors and Affiliations
Contributions
All authors have made substantial contributions to the study. The first draft of the manuscript was written by M.H., and all authors have commented on previous versions of the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Ethical Approval
The study is Data Protection Impact Assessment (DPIA) approved by NTNU and approved by the Regional Committee for Medical and Health Research Ethics (REK) in Norway (2017/1208/REK-midt).
Informed Consent
Participation in the Young-HUNT study was voluntary. All participants had to provide informed written consent to participate. For subjects under 16 years of age, parents had to provide written consent.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Henriksen, M., Skrove, M., Hoftun, G.B. et al. Sex Differences and Similarities in Risk Factors of Physical Aggression in Adolescence. J Child Fam Stud 32, 1177–1191 (2023). https://doi.org/10.1007/s10826-022-02284-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-022-02284-3