
Abstract
Participation in high-quality early childhood education and care (ECEC) benefits children and society. Policy recognition of this manifests through government subsidy strategies to increase ECEC access in the years immediately preceding school. Yet despite this action, many children do not receive the recommended amount. This study utilizes a mixed-methods design to investigate ECEC participation barriers and facilitators in three Australian communities. Parents and service providers completed online questionnaires (45 parents, 63 providers) and semi-structured interviews (21 parents, 16 providers). Results showed that issues related to both direct (e.g., fees) and indirect (e.g., travel) costs are particularly important barriers for families, and are well-recognized by providers. A range of factors were also considered important for facilitating participation (e.g., effective promotion of the benefits linked to high-quality play-based learning in formal settings, professional training of staff). Findings demonstrated the ecological complexity of participation. Strategies to address barriers and harness facilitators are required across multiple levels.
Highlights
-
Participation in high-quality early childhood education benefits children.
-
Many children do not receive the recommended dose of early childhood education.
-
Parents and providers see various participation costs as important barriers.
-
Providers may underestimate barriers relating to maternal role beliefs.
-
Promotion of child benefits and staff training may facilitate participation.
Similar content being viewed by others

Early childhood education and care (ECEC) models delivered outside the family home include long day care, preschool or kindergarten, family day care, occasional care, and outside school-hours care. Research shows participation in formal ECEC models, particularly high-quality center-based care and preschool or kindergarten programs in the 1–2 years immediately preceding school, has a variety of benefits to child health and development (AIHW, 2015, Goldfeld et al., 2016, Warren, O’Connor, Smart, & Edwards, 2016). Investment in the delivery of high quality ECEC also has clear economic advantages, with benefits resulting from increases in productivity through greater labor force participation (of parents, and later children) and cost savings from anticipated reductions in expenditure associated with remedial education, unemployment, justice, and health services (Aos, Lieb, Mayfield, Miller, & Pennucci, 2004, Barnett & Masse, 2007, Heckman, 2006, Nores, Belfield, Barnett, & Schweinhart, 2005, PwC, 2014, 2019).
Early randomized controlled studies dating back to the 1960s and 1970s demonstrated that high quality ECEC participation for children from disadvantaged backgrounds led to improved academic achievement, later educational attainment and health outcomes measured decades later (Muennig, Schweinhart, Montie, & Neidell, 2009, Nores et al., 2005, Ramey et al., 2000). More recently, meta-analyses of experimental and quasi-experimental studies primarily targeting disadvantaged children have shown that ECEC participation has positive effects across a range of short, medium and long-term outcomes (Aos et al., 2004, McCoy et al., 2017).
There is also a growing body of literature demonstrating positive effects of universal ECEC participation (Van Huizen & Plantenga, 2018). Major longitudinal studies in the United Kingdom (e.g., the Effective Provision of Preschool Education study: Sammons et al., 2008, Sylva, Melhuish, Sammons, Siraj-Blatchford, & Taggart, 2004), United States (e.g., Early Childhood Longitudinal Study: Magnuson, Ruhm, & Waldfogel, 2004) and Australia (e.g., Longitudinal Study of Australian Children: Sanson et al., 2002, Warren & Haisken-DeNew, 2013) consistently demonstrate positive associations of preschool attendance with academic performance and some also show positive effects on social-emotional development outcomes. In Australia, population-level cross-sectional research has shown that compared with other forms of ECEC (e.g., family day care), preschool attendance in the year before starting school is associated with significantly lower odds of developmental vulnerability across a range of domains including physical health and well-being; social competence; language and cognitive skills, and communication skills and general knowledge (Goldfeld et al., 2016).
Despite the well-recognized benefits of participation in high quality ECEC, a significant proportion of children miss out (O’Connor et al., 2016). These children are disproportionately from culturally and linguistically diverse families (e.g., indigenous or migrant, non-English speaking backgrounds), those experiencing socio-economic disadvantage, and less stimulating home learning environments (Baxter & Hand, 2013, Biddle & Seth-Purdie, 2013, Coley, Votruba-Drzal, Collins, & Miller, 2014, Gilley, Tayler, Niklas, & Cloney, 2015, Magnuson & Waldfogel, 2005, O’Connor et al., 2016, Sylva et al., 2004). For example, studies have shown that the percentage of children enrolled in preschool in the year before starting school is lower among children from families with: a single-parent; non-English speaking background; lower levels of education; both parents unemployed; Aboriginal or Torres Strait Islander (ATSI) descent; residency in rural or remote areas or socioeconomically disadvantaged communities (AIHW, 2015, Biddle & Seth-Purdie, 2013, O’Connor et al., 2016, Warren et al., 2016). Similar trends have been observed in studies of attendance rates (ABS, 2020, Gilley et al., 2015). That is, even when children from disadvantaged groups enroll in preschool programs, they typically attend for fewer hours than their non-disadvantaged counterparts.
Yet, the number of preschool hours received (that is exposure to preschool as an effective intervention) is important. Reviews of previous research show from 2–3 years of age, part-time attendance is beneficial for the general population, and that disadvantaged children may benefit from more hours or full-time attendance (AIHW, 2015, Melhuish et al., 2015). For example, there is evidence that 15–30 h ECEC per week significantly predicts higher reading and mathematics skills among children from high-income families, but that at least 30 h per week is required before a significant association emerges for children from low income families (Loeb, Bridges, Bassok, Fuller, & Rumberger, 2007). Other evidence indicates 2 years of high quality ECEC for 15 h per week has a protective effect equivalent to having a tertiary-educated mother (Sylva, Melhuish, Sammons, Siraj-Blatchford, & Taggart, 2010). Though there is also some evidence that formal ECEC is associated with increased behavioral problems (Magnuson, Ruhm, & Waldfogel, 2007, Magnuson et al., 2004), the relationship is likely moderated by a variety of factors including family background, program quality, intensity and duration or starting age (Biddle & Seth-Purdie, 2013, Loeb et al., 2007, Magnuson et al., 2007).
Recognizing the positive effects of formal ECEC participation, several governments have developed national commitments to universal access in the year or 2 years prior to school commencement. In Australia, the 2008 National Partnership Agreement on Early Childhood Education introduced a commitment to preschool access for all children with an entitlement of 15 h per week, 40 weeks a year in the year before starting school (Harrington, 2014). The entitlement to free ECEC for all 3- and 4-year-old children is 15 h per week in England and 20 h per week in New Zealand (AIHW, 2015). A global benchmark set by the United Nations Children’s Fund similarly encourages preschool attendance for at least 15 h per week among 4–5 year old children (AIHW, 2015). Throughout this paper, we, therefore, refer to families with children receiving at least 15 h per week of formal ECEC (i.e., preschool or kindergarten or long day care) as recommended-attendance families. We use the term limited-attendance families for those not enrolled or not attending at least 15 h per week. However, as noted above, some research suggests that 15 h per week may not be sufficient to improve child development outcomes among the most disadvantaged children (Loeb et al., 2007, Warren et al., 2016).
Despite recognition of the advantages afforded by good quality ECEC, and international support for policy reform aiming to increase quality and access (Barnett, 2010, Harrington, 2014), there is little published research exploring the factors that facilitate or impede ECEC participation. Broad reviews of the literature on ‘hard-to-reach’ families document a wide range of barriers to accessing health, social, and education services (Boag-Munroe & Evangelou, 2012), and comprehensive investigations of the factors associated with selection of center-based ECEC models have been conducted (Coley et al., 2014). Yet, relatively few publications have specifically focused on (a) ECEC participation barriers and facilitators per se, or (b) the relative importance of different factors, as perceived by parents and providers.
In the United States, qualitative studies with disadvantaged families from ethnically diverse and particularly Hispanic or African American communities have identified a range of barriers to ECEC participation (Ansari, Pivnick, Gershoff, Crosnoe, & Orozco-Lapray, 2020, Susman-Stillman, Englund, Storm, & Bailey, 2018). These include issues related to access, ethnic or racial discrimination, child illness (e.g., chronic health problems, medical appointments), demands of family life (e.g., balancing work and school schedules; housing instability; caring for sick or disabled relatives), transport access and reliability, additional childcare needed to enable attendance at short-day programs, and social isolation. In New Zealand, interviews with parents and providers indicate that cost (e.g., fees, transportation), accessibility (e.g., location, hours of operation, placement capacity) and cultural relevance (e.g., language and program content) of ECEC programs are the main barriers experienced by low income indigenous communities (Mitchell & Meagher-Lundberg, 2017). Similar barriers were identified in interviews conducted with families from several disadvantaged communities in New South Wales, Australia. Specifically, prominent themes related to cost, quality of services, transport, and a perception that young children should be cared for by mothers exclusively (Grace, Bowes, & Elcombe, 2014).
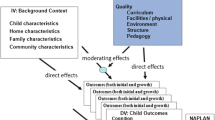
Previous research findings indicate that multi-faceted and interactive effects of personal and environmental factors influence ECEC participation (Coley et al., 2014, Susman-Stillman et al., 2018). One theoretical framework that recognizes such complexity in human behavior and may be useful for understanding ECEC participation is the Social-Ecological Model (SEM; CDC, 2020). This model identifies four nested, hierarchical levels of influence. Factors may be understood to operate at the level of the individual (e.g., knowledge, attitudes), interpersonal relationships (e.g., families, friends), program or service (e.g., staff competence, accessibility), and policy-enabling environment (e.g., funding, policy, laws). Categorization of factors at these levels should facilitate identification of critical leverage points to increase ECEC participation. Despite the potential utility of applying this theoretical framework to ECEC participation research, it has not yet been tested.
Another limitation of the existing literature is that there has been little within-study exploration of the views held by different stakeholders. Few of the studies cited above systematically explored the perceptions of both service providers and parents, and where both views were canvassed (e.g., Mitchell & Meagher-Lundberg, 2017), analysis was not conducted separately. Similarly, within-study comparison of different parent group perspectives (i.e., views among those with low versus high ECEC participation rates) was lacking. Stakeholders from each of these groups may have had different experiences and unique perspectives that have shaped their views. It is important to consider views from multiple perspectives to develop a comprehensive understanding of ECEC participation. Advantages include (a) reducing the likelihood that particular barriers or facilitators will be missed; (b) cross-validation of common barriers and facilitators; and (c) potential to diagnose divergences in views that may be contributing to unsatisfactory ECEC participation rates.
The extant literature is also predominantly qualitative in nature, drawing on interviews and focus groups. As the presence of a researcher and concerns with self-presentation may influence participant responses to interview questions, it is important to supplement such research with other methodologies (e.g., anonymous surveys). In addition to minimizing social pressures to respond a particular way or within a relatively short timeframe, questionnaires afford quantitative exploration of the relevant issues. In the case of ECEC participation research, quantitative investigation can extend the literature beyond identification of various barriers and facilitators to an understanding of which factors stakeholders most consistently rate as important. Mixed methods investigations are needed to more thoroughly investigate the complex issues affecting ECEC participation.
The aim of the present mixed methods study was to investigate various stakeholder views on formal ECEC participation in three Australian communities. More specifically, the study addressed the following research questions:
-
1.
Which potential barriers, previously identified in the research literature, are most consistently rated highly important by (a) limited-attendance families, and (b) ECEC providers?
-
2.
Which potential ECEC participation facilitators are most consistently rated highly important by (a) limited-attendance families; (b) recommended-attendance families; and (c) formal ECEC providers?
-
3.
Which specific issues underly the barriers and facilitators most consistently rated as highly important, and at what levels of the social-ecological model do barriers and facilitators operate?
-
4.
Do parents and providers have similar perspectives on ECEC participation barriers and facilitators?
Method
Research Design
The approach to inquiry was question-driven and conducted pragmatically, utilizing a convergent (i.e., concurrent) mixed methods data collection strategy (Fetters & Freshwater, 2015) comprising an online questionnaire and interview with an overlapping sample of participants. Qualitative and quantitative data were collected in parallel such that the analysis of one data set did not inform the development of the other. The analytic strategy included quantitative analysis of descriptive statistics from questionnaire responses and a codebook-based thematic analysis of interviews (Braun, Clarke, Hayfield, & Terry, 2019). Quantitative analyses measured the extent to which parents and providers considered a range of potential barriers and facilitators important while interview data provided more detailed insights into how barriers and facilitators were experienced, and why some were considered especially important. Differences in parent and provider perspective were explored. The investigation was part of a larger project that included a parallel study of participation in parenting programs (Molloy et al., 2020). The methodological approach for both studies was similar, and studies were jointly approved by the [institution omitted for blind review] Human Ethics Committee (#2019.016).
Researcher Description
The project was designed and conducted by a team comprising predominantly Caucasian Australian female researchers with formal tertiary qualifications in psychology and pediatrics, and previous experience conducting both quantitative and qualitative research with marginalized populations. Additionally, significant input from Caucasian Australian males with formal business qualifications and experience in the private and not-for-profit sectors contributed significantly to the conceptualization of the study.
Researcher-Participant Relationship
Relationships between the research team and key stakeholders were established in an earlier study of ECEC quality in three target communities. Whereas the study coordinators had established prior relationships with key stakeholders, most researchers conducting interviews had not.
Participants
Primary caregiver and provider participants were drawn from three Australian local government areas including two metropolitan and one regional jurisdiction (Brimbank, Wyndham and Central Goldfields, respectively). Population statistics indicate higher rates of unemployment and lower levels of education among communities in these areas, relative to the broader Australian population (ABS. 2016 (2016)). Previous research (Molloy et al., 2020) indicates a substantive proportion (up to 70%) of children attending preschool or kindergarten in these areas do not receive at least 15 h per week in the year before school, and that the proportion is even higher among children with indicators of disadvantage (e.g., disability, parent welfare, non-English speaking background).
Primary caregiver participants were predominantly biological parents, though the study was open to others (e.g., grandparents, step-parents, foster parents, or other carers). For brevity, the term “parent” is used. Parents were eligible to participate in the questionnaire if they had a child aged 2–5 years who was not yet attending primary school. Parents were also eligible to participate in the interview, if their child was either not enrolled in a formal ECEC program (defined as long day care or kindergarten program for the year before starting school, or 3-year-old kindergarten program), or attended the ECEC program less than 15 h per week. That is, parents were eligible to participate in the questionnaire regardless of ECEC attendance amount but interviews were restricted to those who received less than 15 h ECEC per week. In total, 45 parents completed the questionnaire and 21 completed the interview. Though some parents completing the interview also completed a questionnaire, not all did so. Table 1 describes the demographic profile of parent questionnaire respondents.
Interviewees shared similar characteristics: 91% were mothers, 53% were 26–36 years of age, 33% had a Non-English-Speaking Background, 91% did not identify as a refugee or asylum seeker, and 95% indicated they were not of Aboriginal or Torres Strait Islander decent. Approximately half of all parent interviewees were from regional Victoria (52%).
A range of professionals with experience and/or expertize in early childhood services were invited to participate. Questionnaires were restricted to those indicating that they currently worked in a preschool, kindergarten or long day care service, but interviews were open to a wider range of providers (e.g., Maternal and Child Health nurses, supported playgroup facilitators, family day care providers, occasional care workers, parenting program facilitators). In total, 63 providers completed the questionnaire and 16 completed the interview. See Table 2 for the demographic profile of providers completing the questionnaire. Interviewees comprised a mix of professionals who had direct contact with families (n = 9) or administrative roles (n = 7), and worked in regional (n = 9) or suburban (n = 7) communities.
Recruitment Procedures
Consultations with peak bodies (i.e., professional and advocacy organizations such as Early Childhood Australia, Early Learning Association Australia) and early childhood services were leveraged to recruit participants. Primary contacts employed within ECEC services were asked to promote the study among clients and the ECEC workforce using a variety of strategies (e.g., dissemination through professional networks, intranet, emails, flyers, announcements at meetings, word-of-mouth). Subsequently, a snowball sampling method was used whereby participants were encouraged to invite others who might be eligible and interested in participating. The questionnaire link was advertised in the Childhood Early Learning Australia newsletter and Facebook page. Browser cookies were not used to prevent participants from completing the questionnaire multiple times. The rationale for this was to ensure that providers could participate at work on shared devices, and parents without internet access or electronic devices at home could also use shared resources (e.g., friends’ devices, public library computers). Eligible participants who finished questionnaires were also invited to complete interviews. As approved by the ethics committee, interview parents received a $20 supermarket gift card as a token of appreciation. Recruitment took place between April 2019 and October 2020, however, almost all parent questionnaire respondents (n = 42, 93%) participated prior to the emergence of COVID-19 or disruptions to accessing ECEC as a result of the global pandemic. In contrast, most providers participated after March 2020 (n = 53, 84%).
Quantitative Instruments
English-language questionnaires were constructed to assess the extent to which various factors were considered barriers to, or facilitators of, ECEC participation. Separate versions were constructed so that parents considered how their personal circumstances affected ECEC participation whereas providers considered the factors with reference to families in their community (see online supplementary file). Questionnaires were also tailored so that parents who indicated their child received at least 15 h of formal ECEC per week were asked about facilitators only. All questionnaires included screening and demographic items, questions regarding disadvantage, and a list of potential barriers and facilitators. In cases where families had multiple children aged 2–5 years, parents were instructed to answer with reference to their eldest child. Questionnaires were constructed to take less than 15 min and were primarily web-based though paper versions were also available. Online versions were hosted using RedCap software (Harris et al., 2019), and utilized the compulsory question function for eligibility screening items only. Usability was tested prior to going live, confirming participants were able to navigate back and forth through the 7–13 web pages.
Eligibility screening
To assess participant eligibility the parent questionnaire asked “Are you a parent or guardian or caregiver of a child aged 2–5 years who has not yet started school?”. To assess provider eligibility respondents indicated the type of ECEC service in which they were involved. Check-boxes were used (for long day care, family day care, occasional care, supported playgroups, schooling, maternal and child health) and a free response option was available to expand on any other type of early childhood or family service.
Demographic profile
All questionnaires included respondent gender and education items. Parent versions also included items to indicate: age, family income, language, Aboriginal or Torres Strait Islander (ATSI) heritage, and refugee status. Gender, ATSI, and refugee items included “prefer not to answer” options. Following the main demographic items, respondents were asked whether they considered their own (parents) or some family clients (providers) “current living circumstances as disadvantaged, vulnerable, and/or living in adversity”. Those answering affirmatively were asked to select the forms of disadvantage most relevant from the following list: unemployment, low income, poverty, low education, homelessness or unstable housing, youth, rural or remote location, lack of social support or help, ethnicity or culture, refugee or asylum seeker, immigrant, physical health or disability issues, mental health concerns, family violence, drug or alcohol issues, and ‘other’.
ECEC participation status
To determine formal ECEC participation status and separate limited-attendance from recommended-attendance families, several items concerned enrollment and attendance. More specifically, these asked whether the child was formally enrolled in a preschool or kindergarten service and/or a long day care service, the number of hours enrolled per week for each service, and the number of hours the child typically attended each service. Following previous research, other models of ECEC were considered informal.
Barriers and facilitators
To determine the perceived importance of factors thought to influence participation in formal ECEC services, respondents were presented with a list of potential barriers and facilitators. Item development was informed by analysis of themes previously identified in the research literature (Ansari et al., 2020, Coe, Gibson, Spencer, & Stuttaford, 2008, Grace et al., 2014, Mitchell & Meagher-Lundberg, 2017, Susman-Stillman et al., 2018) and consultation with experts in the field. Each item was rated on a 5-point scale ranging from ‘not at all important’ or “not very important” through “somewhat important” to “very important” or “extremely important”. Example barrier items from the parent questionnaire include: “problems with the childcare service location” and “the cost of services”. Example facilitators include: “free transport to/from the service” and “having information about the likely benefits of my child attending the service”.
Item construction was tailored so that wording and selection was appropriate and relevant for each respondent group. For example, those indicating that their child did not attend a formal ECEC service were asked whether there were no places available at their preferred service, whereas those indicating that their child attended less than 15 h were asked whether there were not enough spaces for their child to attend for more hours. Parents who had not enrolled their eligible child in ECEC services were asked to consider barriers to enrollment, whereas parents of limited-attenders rated the extent to which each potential barrier impacted attendance. Provider items referred to “families” whereas parent items were presented in the first person. For facilitators, all parents were instructed to consider the extent to which each factor was or would be important ‘to whether or not (and how much) your child attends kindergarten/preschool and/or long day care’.
Qualitative Interviews
The purpose of qualitative interviews was to explore in depth how barriers and facilitators were experienced by families, and how providers perceived family experiences. Mean duration was 21 min (SD = 11, range 6–38 min) for parents and 41 min (SD = 13, range 24–71 min) for providers. The majority were conducted in person (n = 9 parents, 13 providers) with the remainder by telephone (for participants who indicated this would be more convenient). All commenced with an assessment of participant consent and screening items to confirm eligibility (i.e., parent respondents had a child 2–5 years of age not currently receiving 15 h or more ECEC or enrolled at school, and providers worked in child or family services). Demographic information for parents covered age, relationship to- and living situation with- the child, education, postcode, indigenous background, and refugee or asylum seeker status.
Interviews were semi-structured and conducted reflexively so that questions were appropriate to the ECEC status of respondents. Interviewers first asked whether the family used preschool or kindergarten, long day care services, or any other forms of care. They then asked open-ended questions to ascertain why eligible children received the type and amount of care reported (or lack thereof), and whether families (a) faced any difficulties in accessing services, (b) found participation challenging in any ways, (c) had considered in what circumstances participation might increase, or (d) if anything could be done to ensure children received the amount of ECEC parents would like. More detailed information about the schedule used to guide interviewers is available from the corresponding author upon request. All responses were recorded and transcribed verbatim.
Data Analysis
Survey data were imported into STATA and checked for consistency and response bias. Descriptive statistics were prepared separately for providers and parents. Parent responses were further separated by ECEC participation status so that families with limited attendance (i.e., non-enrollment or less than 15 h per week) could be compared with recommended-attendance families. Although it is possible to differentiate limited-attendance families who had enrolled their child(ren) from those who had not, these sub-samples were small and data was combined.
Interview transcripts were uploaded to NVivo for thematic analysis. The unit of analysis was individual comments (i.e., a single sentence could contain multiple themes and each was coded). Comments were categorized according to the four levels of the SEM framework (individual; relationship-interpersonal; program-service; policy-enabling environment). As sub-categories emerged within each level, these were added to the coding guide. The guide was initially developed by three researchers who coded all transcripts. When uncertainty arose around coding data or creating new codes, discussions were held by the team to resolve these issues. Data was then double-coded by two trained researchers. Themes and sub-themes were analysed separately for provider and parent interviews.
The strategy adopted to integrate findings from quantitative and qualitative methods involved identifying the barriers and facilitators most consistently rated highly important and mapping these to corresponding themes emerging in the qualitative analysis.
Results
Questionnaire participation rates were acceptable and completion rates were high (Eysenbach, 2004). Of 63 consenting parents, 45 (71%) participated (i.e., progressed beyond the demographic section of the questionnaire) and, of these, 44 (98%) completed all but the final section of the questionnaire. Of 88 consenting providers, 63 (72%) participated with all but 1 (98%) answering items on the final page of the questionnaire.
Quantitative Analyses
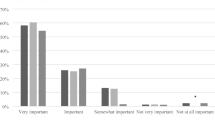
Table 3 shows the percentage of respondents rating each potential barrier very or extremely important, by respondent group. For brevity, we refer to the collapsed responses as highly important and the provider version of items is listed; references to ‘family’ were presented in the first person for parents. Barriers are presented in order of importance (according to providers), not order of presentation in the questionnaire.
Overall, providers were more inclined than parents to rate each of the potential barriers as highly important, with one exception (relating to maternal role beliefs). Of the 17 items presented to providers, 12 were endorsed as highly important by at least half the sample, and all but one by more than a third. In contrast, only one of the items presented to parents was rated highly important by at least half the participants (service costs), and one other (maternal role) by at least a third of the participants. One in five parents rated more than two barriers as highly important.
Among limited-attendance families, the barriers most consistently rated highly important were: (a) cost of services (50%) and (b) a view that it is a mother’s role to educate and care for her young children (42%). For providers, the barriers most consistently rated highly important related to: (a) the benefits of formal ECEC being unclear to families (89%), (b) families not knowing how to access services (79%), and (c) the cost of services (73%).
Table 4 shows the percentage of respondents rating each potential facilitator very or extremely important, by respondent group. Among limited-attendance families, the potential facilitators most consistently rated highly important were: (a) knowing that educators and/or staff are professionally trained (73%), (b) having food provided at the service (60%), and (c) having information about the likely benefits of ECEC attendance (50%). The potential facilitator next most consistently rated highly important related to provision of all-day sessions rather than shorter blocks spread over the week (33%). For recommended-attendance families, the potential facilitators most consistently rated highly important were: (a) knowing that educators and/or staff are professionally trained (93%), (b) having good communication about what is involved in ECEC (93%), (c) having information about the likely benefits of ECEC (76%), and (d) feeling that educators understood their child (70%). Among providers, the potential facilitators most consistently rated highly important were: (a) ensuring that families feel educators understand their child (97%), (b) having good communication about what is involved in ECEC (90%), and (c) families having information about the likely benefits of ECEC (82%). A large percentage of providers also rated as highly important: (d) knowing that educators and/or staff are professionally trained (80%). Thus, two of the top four facilitators as rated by providers were also among the top three facilitators as rated by parents.
Consistent with the barrier ratings, providers were generally more inclined than parents to rate each of the potential facilitators highly important, with only two exceptions; though both groups rated educator training and provision of food at services important, parents were more inclined to do so. Of the 17 items administered, 11 were rated highly important by more than half the providers, 7 by recommended-attendance families, and 3 by limited-attendance families.
Qualitative Analyses
Of the 31 parents who consented to participate in the interview, 21 met eligibility criteria. Of the 16 consenting providers, all were eligible and completed the interview. Drawing on the SEM, interview responses were coded with emergent themes mapped to the four levels of the framework: individual, interpersonal-relationship, program-service, or policy-enabling environment. Detailed results are shown in Supplementary Tables A.1, A.2. The number of respondents citing factors at each level may be less than the sum of respondents coded for each sub-theme. This is because multiple sub-themes were coded where participants discussed more than one issue.
Overview of barriers and facilitators
As shown in Table A.1 (online only), analysis of qualitative interviews revealed almost all parents identified barriers operating at the individual and program-service level. About half discussed issues at the policy-environment level, and just over a quarter raised interpersonal-relationship level themes. A similar pattern was observed for providers: all discussed barriers at the individual and program-service levels, whereas fewer (about two thirds) discussed issues at the policy-environment level. In contrast to parents, most providers also discussed interpersonal-relationship issues.
Table A.2 (online only) shows almost all parents and all providers identified facilitators at the program-service level. About half the parents discussed individual and policy-environment level facilitators, and just under a quarter discussed interpersonal-relationship level themes. Almost all providers also discussed policy-enabling environment themes. Fewer (about a third) discussed individual and interpersonal-relationship level facilitators.
Individual level barriers and facilitators
At the individual level, the most common barriers discussed by parents related to logistics, economic disadvantage, and child health or behavioral issues. The most common themes to emerge in interviews with providers related to parent disadvantage, parent attitudes or beliefs, and logistics. Sub-themes relating to disadvantage and logistics were similar for parents and providers. Respondents from both groups noted that low incomes and unemployment made it difficult for parents to afford service fees or transportation costs incurred to access ECEC services (e.g., fuel, fare, vehicle registration, and maintenance). Logistics sub-themes were also similar across groups with both discussing competing demands (for work and family schedules), and problems with transport (e.g., due to not owning a car, not having a licence to drive, or living too far from services to walk). Where parents discussed child health, most focused on children contracting illnesses at ECEC services and the harms this caused the family, either physically and/or financially. For families who are self-employed or in casual positions, the effects of ECEC participation on health may be critical. Medical appointments or treatments and physical stamina were also discussed, though to a lesser extent. With regard to parent attitudes and beliefs, both parents and providers discussed concerns about child readiness. As one parent put it: “They are only little; they still need time with their family”. Providers also focused heavily on parents not appreciating the value of ECEC participation. This often related to misconceptions about play-based learning and seeing services as merely (expensive) babysitting arrangements.
At the individual level, the main facilitator themes to emerge concerned parent beliefs or attitudes. Both parents and providers discussed the opportunities afforded by ECEC participation for social skills development with peers, school readiness (e.g., toilet training, listening to educators etc.), and parent respite.
Interpersonal-relationship level barriers and facilitators
Whereas few parents discussed barriers at the interpersonal-relationship level, a substantive proportion of providers discussed several ways in which family dynamics and complex issues could impede ECEC participation. For providers, the most common sub-theme related to family violence. In contrast, both parents and providers noted facilitating aspects of the social environment. Several respondents stated that knowledge of ECEC services had been facilitated by discussions with family members, or friends and acquaintances from community service settings (e.g., playgroups, schools) and facilities (e.g., parks, playgrounds).
Program-service level barriers and facilitators
At the program-service level, the most common barrier theme to emerge in interviews for both parents and providers related to accessibility. Within this theme, the most common sub-theme related to service fees, though difficulties with service location and limited places or long waitlists were also discussed. Other major themes emerging for both parents and providers related to program formatting (particularly inconvenient session timing and duration) and service procedures (e.g., confusing or complex enrollment processes). As one parent observed: “your local center offers three short days, but you work and need long days”. Though accessibility, program formatting, and service procedures emerged as the major themes for both parents and providers, barriers relating to ECEC staff skills (e.g., rapport building and sensitive engagement with families) were discussed by a substantive proportion of providers but relatively few parents.
Consistent with barrier themes, the main facilitator themes emerging for parents related to accessibility, program formatting and services procedures. For providers, the main facilitators concerned staff, service procedures, and accessibility. Thus, service accessibility and service procedures were among the main sub-themes to emerge in both parent and provider interviews. Among both parents and providers, accessibility sub-themes included affordability, location, and transport. Respondents noted that participation was or would be facilitated when fees were heavily subsidized or waived, services were within walking distance of family residences, or able to facilitate transportation of children in some way. Suggested transportation arrangements included utilization of a school bus, and access to fuel vouchers.
The main service procedure facilitation sub-themes focused on inter-agency collaboration and easing enrollment processes, with the two often interlinked. For example, several respondents indicated that maternal and child health nurses are well-positioned to promote ECEC enrollment, providing timely information at routine check-ups about how, when, and where to enroll in ECEC services. Other opportunities for cross-promotion included partnering with libraries, primary and allied health providers, and human services. Strategies for assisting families to complete enrollment procedures included simplified registration, data linking to immunization and birth records, and personalized assistance to overcome challenges presented by both online and paper-based systems. One service provider noted: “we will quite often sit down with the families, fill out the forms with them”.
In addition to facilitating service accessibility and procedures, program formatting was a prominent sub-theme for parents. Several indicated greater flexibility in session timing, duration, or frequency to better co-ordinate with other responsibilities (e.g., work, care for school-age or infant siblings), could increase participation. Some also suggested greater flexibility in session timing and duration was needed to better suit their child’s health or development (e.g., shorter days for 3-year-old children). For providers, staff skills emerged as a prominent facilitator sub-theme. Comments mainly focused on the critical importance of educator competence in building rapport and respectful relationships with families.
Policy-environment level barriers and facilitators
At the policy-environment level, approximately two thirds of all parent and provider interviewees discussed barriers relating to government policies. These mostly concerned eligibility criteria for accessing subsidized ECEC, particularly relating to family income, but also to restrictions to eligibility based on child age and citizenship or visa-type. Another theme that emerged for both parents and providers concerned funding to better support children with additional health care or developmental needs. Difficulties with inadequate infrastructure were raised less frequently but both parents and providers suggested the quantity and capacity of existing ECEC services, and availability of public transport, was inadequate in their geographic location.
In terms of facilitation, both parents and providers discussed aspects of government policy and infrastructure that would increase ECEC participation. Most discussion of government policy related to heavily subsidized or free ECEC, though two providers suggested legislation making ECEC participation mandatory would increase service use. With regard to infrastructure both parents and providers indicated a need for (a) more ECEC centers or increased service capacity within the local area, and (b) public transport options for families who do not have access to a car or driver license or cannot walk to the nearest ECEC service.
Summary of Key Insights Emerging from the Questionnaire and Interviews
Table 5 shows how the qualitative interviews drew out specific issues underlying the barriers and facilitators identified as important in the questionnaire. It also shows where the interviews identified critical issues that did not emerge as strongly in the questionnaire. Overall, the three main messages to consistently emerge from the questionnaire and interviews pertained to ECEC costs, awareness of benefits, and staff skills or training. The one theme that appeared more salient in interviews than questionnaires concerned ECEC program scheduling and how this interacts with the various other competing demands families encounter. In contrast, it was the questionnaire that identified the importance of maternal roles, and although not discussed at length, interviews provided key insights into factors that might underpin endorsement of this factor. The selected quotes suggest, for example, that the maternal role barrier may be underpinned by parent perceptions of child development, feelings of anxiety, and prescriptive views about legitimate uses of parent time.
Discussion
Previous research has shown substantive variation in the proportion of children accessing ECEC in the year before school (Goldfeld et al., 2016, O’Connor et al., 2016), but limited exploration of the barriers and facilitators experienced by and most important to Australian families. This study contributes to existing ECEC participation research in several important ways. First, it simultaneously investigates both parent and provider perspectives. Second, it not only identifies key barriers and facilitators, but also provides an indication of relative importance of these factors for different stakeholders. Third, it utilizes a theory-based approach to form a structured and policy-relevant understanding of the ecological complexity that shapes ECEC participation. Finally, the mixed methods approach draws out specific details of how Australian families experience major barriers and facilitators to suggest specific strategies that hold promise for increasing ECEC participation.
Barriers
Consistent with prior research where Australian parents frequently raised themes related to cost and maternal role perceptions (Grace et al., 2014), the present study similarly found these were especially pertinent barriers to ECEC participation. These barriers were most consistently rated highly important by parent questionnaire respondents, and issues with costs were especially salient in interviews. Almost three quarters of providers and half the parent questionnaire respondents in this study rated cost as highly important, and issues relating to costs were discussed in many of the interviews. These findings suggest that cost may be the largest barrier to parents accessing the recommended ECEC dose, despite national policy statements that ECEC should be accessible to parents “in a manner that ensures cost does not present a barrier” (Harrington, 2014).
The importance of cost is consistent with previous research, which shows preschool attendance is typically higher in jurisdictions where preschool programs are government-funded (Baxter & Hand, 2013, Bennett & Tayler, 2006, O’Connor et al., 2016). This barrier must be addressed if participation rates are to increase. Interviews suggest strategies to address ECEC costs will need to consider broadening eligibility criteria for accessing subsidized care, particularly for those with no health care card or visa-based residency. Additional strategies could explore ways to reduce: indirect costs associated with transport (e.g., fuel, car maintenance); cumulative fees for families with multiple children; and hidden costs such as having to take time off paid work when children contract illnesses at ECEC services. The problem with illness may be exacerbated in a post-COVID environment, until wide-scale full-dose vaccination is possible. As it is common for children to experience multiple illnesses each year and common cold symptoms (e.g., cough) can linger for months, families may be unable to justify paying for ECEC places when children are frequently unable to attend for extended periods.
The finding that maternal role perceptions were rated highly important by more than a third of both parents and providers is also consistent with previous research. Indeed, this emerged as a major theme in interviews conducted with another Australian sample - parents from disadvantaged communities in NSW (Grace et al., 2014). Interviews in the present investigation suggested both maternal rights and responsibilities are at play here. Responses reflected both (a) views that families have an inherent right to care for and educate their young children, enjoying this short and precious period in life, and (b) societal norms and prescriptive expectations (e.g., that if a mother is not working, children should be at home). Tied to both views, and consistent with previous Australian research (e.g., Hand, Baxter, Sweid, Bluett-Boyd, & Price-Robertson, 2014), was a clear and consistent perception that young children are not developmentally ready to attend formal ECEC settings and that family-based care is more appropriate. Understanding these nuances is important for formulating strategies to address the ‘maternal role’ barrier.
Extending findings from prior research, the study found providers were generally more inclined than parents to rate each of the potential barriers (and facilitators) as highly important. This likely reflects differences in perspective and the framing of questionnaire and interview questions; parents were instructed to consider personal experiences, whereas providers considered collective experiences. It is likely that providers also had in mind populations experiencing more intense and varied forms of disadvantage than those experienced by the parent sample. This is important to consider as the data from providers suggests that in addition to prohibitive costs, low ECEC participation may also be driven by poor or ineffective promotion of the benefits ECEC provides children and their families, and how families can access ECEC services. Consistent with this, interviews with parents suggested there may be some misconceptions about the benefits of play-based learning, and confusion or difficulty with enrollment processes. Our findings suggest a need to address beliefs that play-based learning is not ‘educational’ and provide practical assistance with enrollment processes (e.g., language translation, finding immunization information).
It is interesting that the sole barrier not endorsed by a larger proportion of providers than parents related to maternal roles. It may be that providers underestimate this barrier and need to better promote within communities a view that it is normal, acceptable and beneficial for mothers to share care and education responsibilities with formal ECEC services. The importance of promoting the benefits of ECEC participation is well appreciated by providers but may be more effective if coupled with initiatives to address maternal role barriers. Although several limited-attendance families indicated an ability to visit or attend to their children while at a service would facilitate participation, further research is needed to identify other specific strategies providers could implement to better acknowledge maternal role beliefs and support family priorities.
Overall, the analysis of ECEC barriers indicates that the barriers considered most important by parents and providers are similar. The findings suggest a need to (a) reduce service costs, (b) more effectively promote the benefits of ECEC participation, and (c) change attitudes about maternal roles.
Facilitators
The investigation of potential facilitators showed substantive alignment in the factors most parents and providers considered particularly important. Consistent with prior research (Grace et al., 2014), parents considered staff training an especially important facilitator. Questionnaire responses showed educator and staff training was consistently rated highly important by both parents and providers. Though few parents expanded on the importance of staff skills in the interviews, providers indicated that skills in establishing sensitive and supportive relationships with families are critical to facilitating ECEC participation. Parent responses to questionnaire items assessing the importance of good communication, and perceiving that educators understand their children, were also consistent with this view. Indeed, these were among the top four facilitators endorsed by parents whose children received the recommended ECEC dose, and among the top five for parents whose children did not. For limited-attendance families, communication and understanding were rated highly important by almost half the sample. Given the smaller sample size this should be interpreted cautiously, but may indicate that for these parents, such facilitators may not be sufficient to increase ECEC participation. For example, it may be that other factors need to be addressed first (e.g., cost, maternal role beliefs). Alternatively, it could be that problems with communication and perceptions of educator understanding at local ECEC services hindered full participation for these parents. However, this seems unlikely given few parents in this group indicated in either the questionnaire or interview that a lack of staff skills or disrespectful educators were barriers to participation.
Across all respondent groups, having information about the likely benefits of one’s child attending a formal ECEC service was also consistently rated highly important and was among the top four facilitators in the questionnaire. Interviews indicated that parents appreciated the opportunities ECEC afforded school readiness and social-emotional skills development, though these appeared less salient to those who had not yet enrolled their children in kindergarten or LDC. Interviews also illustrated a variety of strategies that could better communicate and directly demonstrate the benefits of attendance. These included disseminating pamphlets, hosting open days, and running activities for children at local markets where educators can talk with parents and display the types of learning resources and opportunities on offer at local services. Providers also recognized the outreach opportunities afforded by such strategies for building relationships with families in their community, and assisting parents to overcome specific barriers associated with enrollment procedures.
In contrast to the general alignment across groups regarding the facilitators most consistently rated highly important (i.e., staff training and understanding, good communication, benefits of attendance), there was notable variation in the relative ranking of having food provided at ECEC services. This facilitator was the second most important for limited-attendance families, but eleventh for providers, and one of only a few potential facilitators more consistently rated highly important by parents than providers. This may suggest providers underestimate the importance of food as a potential facilitator. Interestingly, the importance of food was not discussed in interviews by many parents or providers. Rather, the main focus was on strategies that increase service availability (e.g., having enough services or service capacity) and accessibility (e.g., low or no cost, transportation). Nevertheless, the finding that more than half of all respondent groups rated it highly important suggests providing food at services may be a useful strategy for increasing participation. This may especially be the case for families experiencing food insecurity.
Broad Implications
Overall, the findings indicate that ECEC participation is shaped by multiple factors operating across a range of social-ecological levels and this is consistent with previous research (Grace et al., 2014, Hand et al., 2014). For each family, there are likely to be multiple barriers and facilitators operating at various levels. As such, multi-tiered approaches may be needed to effectively increase ECEC participation. Though some program-service level barriers might be addressed directly by program providers (e.g., better promotion of benefits and local staff skills), efforts to address issues at the policy-enabling environment level (e.g., access to free care, funding to increase service capacity) are probably needed to have a substantive effect on ECEC participation.
Barriers to ECEC participation occur within a broad social context and interact with national issues such as housing affordability, food insecurity, and inequitable access to workplace entitlements. Within this context, many families may struggle to overcome barriers that might be considered mere inconveniences (e.g., program formatting, service location, children contracting common illnesses): depending on family circumstances, such barriers can be insurmountable at the individual family and program-service levels. Without strategies to address barriers operating at the highest levels of the social-ecological model, ECEC participation may remain infeasible and incompatible with the demands of daily living for many families. However, reform at the policy-enabling environment level, coupled with the implementation of program-service level efforts at the frontline, could significantly improve ECEC participation.
Limitations
Consistent with previous research (Ansari et al., 2020, Grace et al., 2014, Hand et al., 2014, Susman-Stillman et al., 2018), the results rely on a convenience sample, and this may introduce some bias. It is unclear how many potential participants viewed but did not submit a questionnaire. However, questionnaire and interview completion rates were very high among those who consented to participate, and demographic data indicated the socio-economic status of parent participants was reasonably diverse. As anticipated, there were challenges in recruiting a large sample of families who had not enrolled their children in ECEC services. Nevertheless, approximately half the limited-attendance group comprised families who had not enrolled their children at all, and the identification of facilitating factors among families with higher attendance rates provides useful direction for the development of practices and policies to increase participation.
Along a similar line, few parent participants considered themselves disadvantaged, vulnerable, or experiencing adversity. As such, the findings from parent participants may underestimate the importance of many ECEC barriers for such groups. On the other hand, almost all providers indicated that their ECEC organization served some disadvantaged families. Having canvassed the views of providers partially offsets the risk of underestimating the importance of potential barriers.
Finally, it is important to acknowledge that experimental research is needed to test causal relationships between barriers (or facilitators) and ECEC participation levels. However, canvassing parent and provider perspectives promotes a comprehensive and deep understanding of the complex issues at play. This groundwork is crucial for ensuring that the development of initiatives to boost ECEC participation is informed, efficient and acceptable. It provides services with specific ideas for diagnosis of local barriers and possible solutions to trial within their specific context.
Directions for Future Research
This study has documented a range of barriers hampering ECEC participation, the perceived importance of those barriers, and a variety of strategies thought to facilitate ECEC participation among families from a range of socio-economic backgrounds (in terms of education and income). However, further research is needed to explore the factors affecting ECEC participation among more specific sub-groups such as rural and remote versus urban populations, and families experiencing different forms of disadvantage (e.g., single-parent families, relatively young parenthood, extreme poverty, disability, or health issues). Such work is needed not only to determine the extent to which the factors identified in the current research influence ECEC participation among these groups, but to check for additional barriers and facilitators. Along a similar line, there is also a need to conduct research with fathers. Current methods of enlisting parents in ECEC research inadvertently target mothers as they are typically more engaged in all ECEC service types. The experiences, thoughts, feelings, and behaviors of fathers have been neglected in early childhood research (Ames, Glenton, & Lewin, 2017, Ancell, Bruns, & Chitiyo, 2016), but are likely very important for understanding how family dynamics might influence ECEC participation. This information could be particularly instructive for the development of strategies to address maternal role beliefs that block ECEC participation.
Further research is also needed to identify and test specific strategies for addressing ECEC participation barriers. For each barrier, there are likely to be solutions operating at different levels of the social-ecological model. For example, strategies to reduce participation costs, or promote the benefits of ECEC participation, can be applied at both program-service and policy-environment levels. At the program-service level, indirect transportation costs could be reduced by the operation of kindergarten buses (potentially in partnership with primary schools) or facilitation of family car-pooling. At the policy-environment level, costs could be reduced by providing free public transport to and from ECEC services, expanding government eligibility criteria for access to subsidized ECEC, or providing incentives for services to reduce fees. Likewise, strategies to promote parent awareness of ECEC benefits may operate at different levels (e.g., government-funded national media campaigns, employment of outreach coordinators, grassroots advertising by providers). Future research should also explore the acceptability, feasibility, and effectiveness of various strategies to increase ECEC participation.
Conclusion
Overall, this study shows considerable convergence across parent and provider views on the importance of various ECEC participation barriers and facilitators, and highlights specific divergences. Findings indicate the need to: (a) reduce both direct and indirect service costs; (b) increase flexibility in program formatting so participation can be coordinated with the demands of work and other family responsibilities; (c) more effectively promote the benefits of play-based learning in formal ECEC settings; and (d) change attitudes about maternal roles and child readiness to participate in ECEC. Application of the SEM framework to interview data demonstrates the ecological complexity of ECEC participation, and illustrates the importance of both addressing barriers and harnessing facilitators across multiple levels. As such, the study provides a valuable resource for policy development and decision-making that could substantively increase ECEC participation, and by extension reduce both the individual and societal economic burdens associated with missed ECEC opportunities.
Data Availability
In compliance with ethics approval raw data is not publicly available. It will be stored electronically and then destroyed either 7 years following project completion or 5 years from publication of results.
References
ABS. (2016). 2016 Census QuickStats. Retrieved from https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/036. Accessed 9 September 2021.
ABS. (2020). Preschool Education Australia 2019. Retrieved from https://www.abs.gov.au/statistics/people/education/preschool-education-australia/latest-release#data-download. Accessed 9 September 2021.
AIHW. (2015). Literature review of the impact of early childhood education and care on learning and development: working paper, Cat. no. CWS 53. Canberra: Australian Institute of Health and Welfare.
Ames, H. M., Glenton, C., & Lewin, S. (2017). Parents’ and informal caregivers’ views and experiences of communication about routine childhood vaccination: a synthesis of qualitative evidence. Cochrane Database of Systematic Reviews, 2, CD011787 https://doi.org/10.1002/14651858.CD011787.pub2.
Ancell, K., Bruns, D., & Chitiyo, J. (2016). The importance of father involvement in early childhood programs. Young Exceptional Children, 21, 22–33. https://doi.org/10.1177/1096250615621355.
Ansari, A., Pivnick, L., Gershoff, E., Crosnoe, R., & Orozco-Lapray, D. (2020). What do parents want from preschool? Perspectives of low-income Latino/a immigrant families. Early Childhood Research Quarterly, 52, 38–48. https://doi.org/10.1016/j.ecresq.2018.08.007.
Aos, S., Lieb, R., Mayfield, J., Miller, M., & Pennucci, A. (2004). Benefits and costs of prevention and early intervention programs for youth. Olympia: Washington State Institute for Public Policy.
Barnett, W. S. (2010). Universal and targeted approaches to preschool education in the United States. International Journal of Child Care and Education Policy, 4, 1–12.
Barnett, W. S., & Masse, L. N. (2007). Comparative benefit-cost analysis of the Abecedarian program and its policy implications. Economics of Education Review, 26, 113–125. https://doi.org/10.1016/j.econedurev.2005.10.007.
Baxter, J., & Hand, K. (2013). Access to early childhood education in Australia (Research Report no. 24). Melbourne: Australian Institute of Family Studies.
Bennett, J., & Tayler, C. P. (2006). Starting strong II: Early childhood education and care. Paris, France: OECD.
Biddle, N., & Seth-Purdie, R. (2013). Development risk exposure and participation in early childhood education: How can we reach the most vulnerable children? Canberra: HC Coombs Policy Forum & Social Policy Institute, Australian National University.
Boag-Munroe, G., & Evangelou, M. (2012). From hard to reach to how to reach: A systematic review of the literature on hard-to-reach families. Research Papers in Education, 27, 209–239. https://doi.org/10.1080/02671522.2010.509515.
Braun, V., Clarke, V., Hayfield, N., & Terry, G. (2019). Thematic analysis. In P. Liamputtong (Ed.), Handbook of Research Methods in Health Social Sciences (pp. 843-860). Singapore: Springer Nature.
CDC. (2020). The Social Ecological Model: A framework for prevention. Retrieved from https://www.cdc.gov/violenceprevention/publichealthissue/social-ecologicalmodel.html. Accessed 9 September 2021.
Coe, C., Gibson, A., Spencer, N., & Stuttaford, M. (2008). Sure start: voices of the ‘hard-to-reach’. Child Care Health Development, 34, 447–453. https://doi.org/10.1111/j.1365-2214.2008.00816.x.
Coley, R. L., Votruba-Drzal, E., Collins, M. A., & Miller, P. (2014). Selection into early education and care settings: Differences by developmental period. Early Childhood Research Quarterly, 29, 319–332. https://doi.org/10.1016/j.ecresq.2014.03.006.
Eysenbach, G. (2004). Improving the quality of web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). Journal of Medical Internet Research, 6, e34 https://doi.org/10.2196/jmir.6.3.e34.
Fetters, M., & Freshwater, D. (2015). Publishing a methodological mixed methods research article. Journal of Mixed Methods Research, 9, 203–213. https://doi.org/10.1177/1558689815594687.
Gilley, T., Tayler, C., Niklas, F., & Cloney, D. (2015). Too late and not enough for some children: early childhood education and care (ECEC) program usage patterns in the years before school in Australia. International Journal of Child Care and Education Policy, 9. https://doi.org/10.1186/s40723-015-0012-0.
Goldfeld, S., O’Connor, E., O’Connor, M., Sayers, M., Moore, T., Kvalsvig, A., & Brinkman, S. (2016). The role of preschool in promoting children’s healthy development: Evidence from an Australian population cohort. Early Childhood Research Quarterly, 35, 40–48. https://doi.org/10.1016/j.ecresq.2015.11.001.
Grace, R., Bowes, J., & Elcombe, E. (2014). Child participation and family engagement with early childhood education and care services in disadvantaged Australian communities. International Journal of Early Childhood, 46, 271–298. https://doi.org/10.1007/s13158-014-0112-y.
Hand, K., Baxter, J., Sweid, R., Bluett-Boyd, N., & Price-Robertson, R. (2014). Access to early childhood education in Australia: Insights from a qualitative study (Research Report No. 28). Melbourne: Australian Institute of Family Studies.
Harrington, M. (2014). Universal access to early childhood education: A quick guide. Canberra: Australian Department of Parliamentary Services.
Harris, P. A., Taylor, R., Minor, B. L., Elliott, V., Fernandez, M., O’Neal, L., Duda, S. N. (2019). The REDCap consortium: Building an international community of software partners. Journal of Biomedical Informatics. https://doi.org/10.1016/j.jbi.2019.103208.
Heckman, J. (2006). The economics of investing in children. Retrieved from http://www.ucd.ie/geary/static/publications/policybriefings/geary_report1.pdf.
Loeb, S., Bridges, M., Bassok, D., Fuller, B., & Rumberger, R. W. (2007). How much is too much? The influence of preschool centers on children’s social and cognitive development. Economics of Education Review, 26, 52–66. https://doi.org/10.1016/j.econedurev.2005.11.005.
Magnuson, K., Ruhm, C. J., & Waldfogel (2007). Does prekindergarten improve school preparation and performance? Economics of Education Review, 26, 33–51. https://doi.org/10.1016/j.econedurev.2005.09.008.
Magnuson, K., Ruhm, C. J., & Waldfogel, J. (2004). Does prekindergarten improve school preparation and performance? Cambridge Massachusetts: National Bureau of Economic Research.
Magnuson, K., & Waldfogel, J. (2005). Early childhood care and education: Effects on ethnic and racial gaps in school readiness. The Future of Children, 15, 169–196. https://doi.org/10.1353/foc.2005.0005.
McCoy, D. C., Yoshikawa, H., Ziol-Guest, K. M., Duncan, G. J., Schindler, H. S., Magnuson, K., & Shonkoff, J. P. (2017). Impacts of early childhood education on medium- and long-term educational outcomes. Educational Researcher, 46, 474–487. https://doi.org/10.3102/0013189X17737739.
Melhuish, E., Ereky-Stevens, K., Petrogiannis, K., Ariescu, A., Penderi, E., Rentzou, K.,… Leseman, P. (2015). A review of research on the effects of early childhood Education and Education and Care (ECEC) upon child development; CARE project curriculum quality analysis and impact review of European Early Childhood Education and Care (ECEC). Retrieved from http://ecec-care.org/resources/publications/.
Mitchell, L., & Meagher-Lundberg, P. (2017). Brokering to support participation of disadvantaged families in early childhood education. British Educational Research Journal, 43, 952–967. https://doi.org/10.1002/berj.3296.
Molloy, C., Lam, J., Laughlin, A., Quinn, P., Beatson, R., Harrop, C., . . . Goldfeld, S. (2020). Participation in early childhood education and care: Barriers and facilitators. A Restacking the Odds Solutions Report. Melbourne: Murdoch Children’s Research Institute. Royal Children’s Hospital, Human Ethics Committee (#2019.016)
Muennig, P., Schweinhart, L., Montie, J., & Neidell, M. (2009). Effects of a prekindergarten educational intervention on adult health: 37-year follow-up results of a randomized controlled trial. Research and Practice, 99, 1431–1437.
Nores, M., Belfield, C., Barnett, S. W. & Schweinhart, L. (2005). Updating the economic impacts of the High/Scope Perry Preschool Program. Educational Evaluation & Policy Analysis, 27, 245–261. https://www.jstor.org/stable/3699571.
O’Connor, M., Gray, S., Tarasuik, J., O’Connor, E., Kvalsvig, A., Incledon, E., & Goldfeld, S. (2016). Preschool attendance trends in Australia: Evidence from two sequential population cohorts. Early Childhood Research Quarterly, 35, 31–39. https://doi.org/10.1016/j.ecresq.2015.11.004.
PwC. (2014). Putting a value on early childhood education and care in Australia. Retrieved from https://www.pwc.com.au/publications/early-childhood-education.html.
PwC. (2019). A Smart investment for a smarter Australia: Economic analysis of universal early childhood education in the year before school in australia. Melbourne: PriceWaterhouseCooper.
Ramey, C., Campbell, F., Burchinal, M., Skinner, M., Gardner, D., & Ramey, S. (2000). Persistent effects of early childhood education on high-risk children and their mothers. Applied Developmental Science, 4, 2–14. https://doi.org/10.1207/S1532480XADS0401_1.
Sammons, P., Sylva, K., Melhuish, E., Siraj-Blatchford, I., Taggart, B., Hunt, S., & Jelicic, H. (2008). Effective pre-school and primary education 3-11 project (EPPE 3-11): Influences on children’s cognitive and social development in year 6. United Kingdom: Department for Children, Schools and Families.
Sanson, A., Nicholson, J., Ungerer, J., Zubrick, S., Wilson, K., Ainley, J., Wake, M. (2002). Introducing the longitudinal study of Australian children: LSAC discussion paper No. 1. Melbourne: Australian Institute of Family Studies.
Susman-Stillman, A., Englund, M. M., Storm, K. J., & Bailey, A. E. (2018). Understanding barriers and solutions affecting preschool attendance in low-income families. Journal of Education for Students Placed at Risk (JESPAR), 23, 170–186. https://doi.org/10.1080/10824669.2018.1434657.
Sylva, K., Melhuish, E., Sammons, P., Siraj-Blatchford, I., & Taggart, B. (2010). Early childhood matters: Evidence from the effective pre-school and primary education project. London: Routledge.
Sylva, K., Melhuish, E. C., Sammons, P., Siraj-Blatchford, I., & Taggart, B. (2004). The Effective Provision of Pre-school Education (EPPE) Project: Findings from pre-school to end of key stage 1. Nottingham, United Kingdom: Department of Education and Skills.
Van Huizen, T., & Plantenga, J. (2018). Do children benefit from universal early childhood education and care? A meta-analysis of evidence from natural experiments. Economics of Education Review, 66, 206–222. https://doi.org/10.1016/j.econedurev.2018.08.001.
Warren, D., & Haisken-DeNew. (2013). Early bird catches the worm: The causal impact of pre-school participation and teacher qualification on Year 3 national NAPLAN cognitive tests. Melbourne: Melbourne Institute of Applied Economic and Social Research.
Warren, D., O’Connor, M., Smart, D., & Edwards, B. (2016). A critical review of the early childhood literature. Melbourne: Australian Institute of Family Studies.
Acknowledgements
We thank Caitlin Macmillan, Janine Lam, Adrian Laughlin, Shona Cawley, Deb Osborne, and Ifrah Abdullahi for assistance collecting and coding the data.
Funding
This work was supported by the Paul Ramsay Foundation, Eureka Benevolent Foundation, Commonwealth Department of Social Services, and the Victorian Government’s Operational Infrastructure Support Program and Department of Education and Training. Prof Goldfeld is supported by an Australian National Health and Medical Research Council (NHMRC) Practitioner Fellowship [APP1155290].
Author information
Authors and Affiliations
Contributions
C.M.: conceptualization, funding acquisition, project administration, supervision, methodology, validation, writing-review & editing; R.B.: formal analysis, writing-original draft, writing-review & editing; Z.F.: investigation, formal analysis, writing-review & editing; C.H., N.P. & S.G.: conceptualization, funding acquisition, writing-review & editing.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Ethics Approval
The study was approved by the Royal Children’s Hospital Human Ethics Committee and performed in accordance with the Declaration of Helsinki.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
About this article

Cite this article
Beatson, R., Molloy, C., Fehlberg, Z. et al. Early Childhood Education Participation: A Mixed-Methods Study of Parent and Provider Perceived Barriers and Facilitators. J Child Fam Stud 31, 2929–2946 (2022). https://doi.org/10.1007/s10826-022-02274-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-022-02274-5