
Abstract
This paper reviews the published work of me along with my students and close colleagues on the topic of heart rate variability biofeedback (HRVB). It includes early research by Vaschillo documenting resonance characteristics of the baroreflex system that causes large oscillations in heart rate when breathing at resonance frequency, research on heart rate variability as a marker of parasympathetic stress response in asthma, and HRVB as a treatment for asthma and depression. Many questions about HRVB remain unresolved, and important questions for future research are listed.
Similar content being viewed by others
Introduction
My first involvement in heart rate variability research came from my research on the psychophysiology of asthma, where I was interested in studying the phenomenon of stress-induced asthma (Isenberg et al., 1992). Since the autonomic nervous system interacts with asthma primarily through the effects of parasympathetic activity (Scott & Fryer, 2012), which, via the vagus nerve, acts to constrict the airways, I became interested in a noninvasive measure of parasympathetic function. I soon discovered the work of Stephen Porges (2011) on respiratory sinus arrhythmia (RSA), the pattern of HRV associated with breathing, whereby heart rate rises during inhalation and falls during exhalation, due to increased vagus nerve activity during exhalation. I contacted him, and began a collaboration that took us through a number of investigations. After learning about heart rate variability biofeedback (HRVB) in a visit to St. Petersburg, Russia, in 1992, I began a long collaboration with a scientist I met there, Evgeny Vaschillo, who eventually moved to the United States. He had done studies showing the mechanisms behind which HRVB produced high-amplitude oscillations in HRV (Vaschillo et al., 2002), and, working together at Rutgers University, we did a number of studies expanding upon his work. He became my mentor in this field, and should be credited as the one who made this method credible to the international biofeedback community. Soon afterward, at a meeting of the Association for, Applied Psychophysiology & Biofeedback, I attended a lecture on the topic of HRVB by Richard Gevirtz, who had independently developed an interest in the topic and, along with his many students, had begun research on the topic. Richard is the consummate teacher, whose acumen, energy, and engaging manner brought bright doctoral students to his laboratory, and gave them access to various clinical populations where they began collecting a substantial body of clinical data. With our complementary abilities and interests, he and I decided to combine forces in teaching and writing summary papers on HRVB (Gevirtz et al., 2016; Lehrer & Gevirtz, 2014, 2016, 2018), in a collaboration that has persisted to the current day, one of the most enjoyable and productive relationships in my professional career. Another collaboration that shaped my work was with Dwain Eckberg, who had done seminal work on the human baroreflex (Eckberg & Sleight, 1992), and introduced me to the work of Tom Kuusela, who had developed a program, WinCPRS (Absolute Aliens, Turku, Finland) that allowed us to assess the baroreflex easily through cross spectral analysis (Airaksinen et al., 1997) without the need for special maneuvers that would interfere with ordinary rest or HRVB procedures and that allowed us to measure phase relationships. It also allowed us to calculate transfer functions and phase relationships among respiration, beat-to-beat blood pressure and heart rate.
Review of Research and Findings
HRV biofeedback and asthma. According to previous research, about 40% of asthma patients had experience asthma attacks resulting from a period of stress (Isenberg et al., 1992). This initially had surprised me, because stress was usually associated with sympathetic arousal, which should improve asthma, since sympathetic stimulation dilates the airways (Garcia-Araujo et al., 2015). However, parasympathetic stress reactions are known (Eccles et al., 2015) and stress is known to increase inflammation (Rosenkranz et al., 2016), a causative factor in asthma. Gellhorn had shown that sympathetic arousal potentiates parasympathetic reactivity (Gellhorn and Loofbourrow, 1963), and, although sympathetic arousal usually exerts a blocking effect on parasympathetic activity, severe stress can trigger parasympathetic breakthroughs, so that both sympathetic and parasympathetic symptoms can occur, such as sexual arousal or hunger during severe stress. Also it was known that people with blood phobias tend to faint when exposed to blood (Sledge, 1978), a parasympathetically-mediated vasovagal reaction. Could it be possible that some asthma patients show a parasympathetic stress reaction? Passive coping with stress seems to be associated with parasympathetic arousal (Lehrer et al., 1996) as does, in asthma a repressive coping style (Feldman et al., 2002). Perhaps parasympathetic arousal is a component of a stress-related ‘play dead’ response to stress, and that this characterizes stress-related asthma exacerbations. We have not found evidence, however, for whether asthma patients with stress-related asthma symptoms have a greater tendency toward a passive coping style: a topic worthy of systematic study.
To measure parasympathetic function we measured RSA. In our first study we found that, in active coping tasks such as mental arithmetic and reaction time, respiratory resistance and RSA both decreased in asthma patients (Lehrer et al., 1996). These effects were absent during exposure to passive stressors such as watching an accident film, which participants rated as equally stressful. We also found a significant relationship between RSA amplitude and airway reactivity to methacholine (a parasympathetic stimulant used to test for presence and severity of asthma). Palmar skin conductance also was higher among patients with greater airway reactivity to methacholine, suggesting a greater sensitivity in the cholinergic system. (Although skin conductance is sympathetically mediated, the neurotransmitter is acetylcholine, as in the parasympathetic system.)
Additionally, results of a relaxation study for treating asthma yielded unexpected RSA findings (Lehrer, Generelli, et al., 1997). Although the effects of practicing relaxation appeared to produce small improvements in spirometry over the course of several months of practice, the short-term effects appeared to be countertherapeutic: decreases in spirometric measures of pulmonary function, correlated with increases in RSA. We interpreted this as an example of parasympathetic rebound induced by a sudden decrease in sympathetic arousal. The longer-term beneficial effects were attributed to decreased autonomic reactivity due to decreased levels of stress.
Another study assessing RSA was our first paced breathing study (Lehrer, Generelli, et al., 1997; Lehrer, Hochron, et al., 1997), where healthy people were asked to breathe through a resistive load at a pace of 0.125 Hz, a rate we now know to be considerably higher than the resonance frequency at which people breathe during HRVB (Sargunaraj et al., 1996). Nevertheless, RSA increased during paced breathing, perhaps reflecting what we now know to be the effect of breathing close to resonance frequency (even if not exactly at it [Vaschillo et al., 2002]), although it was lower during resistive breathing than while breathing without resistance, probably caused by suppression of vagal activity by the effort of breathing through a resistor. Interestingly, however, although RSA greatly increased, mean heart rate did not change. We interpreted the results as consistent with Porges’ theory of a polyvagal system, which postulates that oscillatory activity in heart rate is controlled by different processes than those controlling tonic parasympathetic activity, with the former representing control processes while the latter reflect vegetative arousal levels.
In still another study we tested Kotses’ theory that specifically relaxation of the facial muscles, by frontalis EMG biofeedback, would help asthma by decreasing vagus nerve activity through a vagal trigeminal reflex arc. Contrary to Kotses et al.’s theory, we found no relationship between changes in frontal EMG and changes in RSA, and, in this study, no effect of increasing frontalis muscle tension on changes in respiratory resistance (Lehrer, Hochron, et al., 1997). We also did two drug studies on healthy people showing that two parasympathetic blocking agents, atropine and ipratropium bromide, dramatically decreased RSA (Lehrer et al., 1994a, 1994b). Findings on the latter drug were particularly striking. Ipratropium bromde is often used as a second-line bronchodilator drug for asthma and other respiratory diseases, and it had been thought not to have systemic effects. Our results showed that it did. We also found a relationship between vagal activation and impaired stress-related respiratory function in asthma (Feldman et al., 2002) as revealed by the psychological characteristic of defensiveness, or “repressive coping style”, as measured by the Crowne-Marlowe Social Desirability Scale (Crowne & Marlowe, 1960). Among defensive asthma patients, as opposed to nondefensive asthma patients, in response to stressful laboratory tasks, we found a higher amplitude of RSA and a decrease in a spirometry measure (the amount of air exhaled in the first second of a forced expiratory maneuver from maximum vital capacity, or FEV1), suggesting a worsening of airway function, while nondefensive participants showed an increase. This result is consistent with other studies showing greater psychophysiological reactivity to stress among people who are defensive, but with a different direction of autonomic effects. Usually defensive people show greater sympathetic and diminished parasympathetic arousal in response to stress. In our study, nondefensive people showed this trend, including an improvement in pulmonary function, while defensive people showed the opposite. These results are consistent with the possibility that asthma patients who show greater asthma vulnerability to stress show stress-related parasympathetic arousal, mediating worsening of asthma.
In a later study, we found that HRV was a robust measure of workload among airline pilots exposed to various difficult tasks in a flight simulator (Lehrer et al., 2010b).
In a 1992 visit to St. Petersburg, Russia, during the period closely following the demise of communism, I had the occasion to visit a private institute, the Biosvyaz corporation, that was using biofeedback to teach people to increase their RSA. I have described this adventure in a memoir published in Biofeedback (Lehrer, 2013). To my great surprise, however, their target population was children with asthma. Contrary to my expectations that this should increase asthma symptoms in their patients, they claimed that all of them were getting better. To prove their point, they shared pre-post treatment pulmonary function data from 20 successive patients showing significant improvement in spirometry. Wanting greater exposure in the West, they invited me to collaborate with them in publishing these data (Lehrer et al., 2000). At the same time I was carrying out a small pilot study of EMG biofeedback-assisted relaxation effects on asthma, and I decided to include a condition in which patients were given heart rate variability biofeedback. With only six participants in each group, we found a significant interaction, showing decreases in respiratory resistance, as measured by forced oscillation pneumography, only among people receiving HRVB. But how could this be? The results obviously did not result from increased parasympathetic activity. Other options included effects of deep breathing, which may stretch the airways. Deep breathing is known to temporarily decrease airway reactivity in methacholine challenge test (Jackson et al., 2004). Another possibility was a decrease in airway inflammation, thought to be a fundamental mechanism for asthma (National Asthma Education & Prevention Program, 2007), and increased vagus nerve activity, the mechanism for biofeedback-induced increases in RSA. Increased vagus nerve activity known to decrease inflammation (Pavlov & Tracey, 2012).
We later had the opportunity to do two larger studies of HRV biofeedback to treat asthma. In the first, among people with varying levels of asthma severity (from mild to severe) we found that, compared with no treatment and a placebo condition involving false EEG biofeedback and listening to relaxing music, HRV biofeedback improved pulmonary function as measured by forced oscillation pneumography and decreased asthma symptoms while allowing decreases in consumption of asthma medications (Lehrer et al., 2004). We additionally found that the method completely eliminated asthma exacerbations during the three-month period of the study, and, on average, improved clinical level of asthma severity as measured by an index of pulmonary function, symptoms, and medication consumption. However the mechanism for these effects remained elusive. Asthma improvement did not correlate with changes in HRV or baroreflex activity. Also, despite lower levels of HRV during biofeedback and smaller increases over time, older participants showed the same or greater levels of asthma improvement (Lehrer et al., 2006).
In a later study (Lehrer et al., 2018) we asked the question of whether HRV biofeedback can substitute for asthma controller medication. In this case, we compared HRV biofeedback with real EEG biofeedback to increase frontal-to-occipital EEG alpha rhythms and paced breathing at relaxed baseline rate, usually approximately 15 breaths/min, among steroid naïve asthma patients with mild or moderate asthma. We found that the comparison condition did as well as HRV biofeedback in improving most indices of asthma: symptoms, pulmonary function, airway reactivity to methacholine, and albuterol use. Participants in both groups improved significantly, suggesting that HRV biofeedback did not have a specific effect, although the general procedure of paced breathing and relaxation may have been salutary ingredients. Of course, regression to the mean may also have occurred, so these results of the study are ambiguous. However, we found a decrease in airway inflammation, as measured by exhaled nitric oxide, only in the HRVB group, suggesting a specific biofeedback effect on this underlying condition.
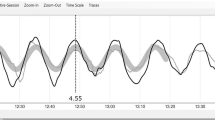
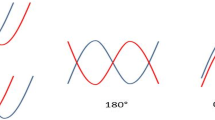
The dynamics of heart rate variability biofeedback. Understanding the mechanism for biofeedback effects required another trip to St. Petersberg, where I first met Evgeny Vaschillo, a physiologist and engineer who had done his doctoral research on the mechanisms by which heart rate variability biofeedback worked. In a small group of Soviet cosmonauts, he had found important frequency-related phase relationships between heart rate and beat-to-beat blood pressure. He had asked people to try to replicate a computer-generated sine wave oscillation signal with their heart rate, not telling them that the heart rate signal was in fact heart rate, nor telling them how to achieve this effect. In order to exactly replicate the stimulus signal, a peak-to-trough oscillation in heart rate of 60 beats/min was required for each oscillation. He found that the high-amplitude heart rate oscillations could only be replicated at one frequency for each person, and that this frequency varied between 4.5 and 6.5 cycles/min. Further, he found important frequency-dependent phase relationships among the stimulus signal, breathing, heart rate, and blood pressure. At the frequency of maximum heart rate oscillation amplitude, the following phases were observed: respiration was in phase with both the stimulus signal and heart rate (0° phase relationship) while heart rate and blood pressure oscillated with the opposite phase relationship (180 ). Thus when the stimulus prompted people to increase their heart rate they inhaled, and to decrease it they exhaled, with increases in heart rate and decreases in blood pressure exactly coinciding with inhalation and the opposite heart rate and blood pressure responses occurring with exhalation, a relationship found at no other frequency. Also, at exactly this frequency blood pressure oscillations were at their minimum amplitude. Only one possibility could explain these relationships: that breathing at that particular frequency produced maximal stimulation of the baroreflex. The baroreflex is a control reflex, such that increases in blood pressure produce decreases in heart rate. This, with a slight delay, produces a mechanical decrease in blood pressure (less blood flowing through the same size tube), with opposite heart rate effects occurring during decreases in blood pressure. However, the amplitude of the heart rate oscillation was greater than the sum of spontaneously-occurring rhythms produced by breathing (RSA) and the baroreflex. This could only be a characteristic of resonance. Indeed, the baroreflex system appeared to have the formal requirements for resonance effects: a feedback system with a constant delay (caused the time needed for blood pressure to change in response to heart rate changes) (Grodins, 1963). As Vaschillo and I discussed this work and its implications for the biofeedback discipline, we decided write a paper describing it in for publication in Applied Psychophysiology & Biofeedback. We had difficulty publishing it in several journals because reviewers could not believe that heart rate swings of close to 60 beats/min could reliably be produced in normal people, and even the biofeedback journal initially as reluctant to publish it because reviewers thought that the material was too abstruse; but it eventually it was published in this journal (Vaschillo et al., 2002), and has been widely cited since then. In this study Vaschillo had not prompted participants to modify HRV by changing respiration rates, although most presumably did. In a later paper, we reported that respiration and HRV were in phase with each other only at each participant’s resonance frequency (Vaschillo et al., 2004).
In the meantime we had been doing a study of paced breathing effects on heart rate variability, with breathing paced at various rates from 3 per min to 14, We found the highest amplitude of RSA at four and six breaths/min, with a decrease at three per min (Song & Lehrer, 2003). This finding replicated Vaschillo et al.’s finding of resonance in the neighborhood of six per min, and also replicated a finding from Vaschillo et al. (2002) that induced HRV amplitudes were at a minimum in the range of two to three cycles/min because of negative resonance at that frequency. Here heart rate and blood pressure were oscillating in phase with each other. In this relationship, as people tried to increase their heart rate by breathing, the baroreflex would act to decrease it. However resonance appeared to occur in the vascular system at that slow frequency, as maximal blood pressure swings occurred in this frequency range, but because HRV baroreflex gain was minimized, blood pressure swings were maximized.
In one of our later studies, at Rutgers University, we found that each person’s frequency of resonance was related to height and to gender, with slower frequencies for taller people and men than for shorter people and women (Vaschillo et al., 2006)—a relationship probably caused by blood volume. There was no relationship between asthma condition and resonance frequency, and none between age or weight and resonance frequency, the latter probably because adipose tissue contains little blood flow. We further found that resonance frequency appeared unchangeable, even after several months of biofeedback practice, where large increases were found in baroreflex gain and heart rate variability. We found that the average resonance frequency was 5.5 cycle times/min.
In a recent analysis of some data from our laboratory we revisited phase relationships between breathing and heart rate variability while breathing at resonance frequency (Lehrer, Kaur, et al., 2020). In my own advancing age, I had found that the phase between heart rate and respiration was no longer zero degrees, but that breathing tended to trail heart rate changes by almost 90 degrees, such that, to achieve maximum HRV amplitude, inhalation started toward the middle of each heart rate swing. In our data on 27 individuals, we found that the phase was related to age. Among young people, as studied by Vaschillo et al. (2002) the phase was indeed 0 degrees, but among older folks the phase approached 90 degrees. However, the resonance effects were the same. Respiration provided the rhythmic perturbation of heart rate that stimulated the baroreflex system at its resonance frequency, causing the same very large swings in heart rate variability found among younger people, However, just as heart rate variability in general is smaller among older people than younger, so is the increase at resonance frequency. The system does not appear as capable of generating the large HRV swings as we age, although clinical effects, at least for asthma, may be just as great.
In other studies, we examined the effect of HRV biofeedback on baroreflex gain in larger samples. Among healthy people (Lehrer et al., 2003) we found large immediate biofeedback effects on increasing baroreflex gain, i.e., the number of beats per minute changes in heart rate for each millimeter Hg change in blood pressure. Also, after three months of daily practice, we found an increase in resting biofeedback gain, when not practicing the technique. We concluded that the large immediate increases in baroreflex stimulation during biofeedback practice provided exercise to the baroreflexes, thus increasing efficiency of the reflex with time and practice. Nevertheless we found that HRV and baroreflex increases were significantly smaller among older people (over age 40) than younger (Vaschillo et al., 2006), just as resting HRV is known to have smaller amplitude in older people.
Biofeedback may not be the only method by which resonance frequency breathing might be taught. Others have found greatly increased HRV with a sinusoidal pattern after training in Yoga (Sharpe et al., 2021), and we have observed it among Zen monks (Lehrer et al., 1999) doing tanden breathing, where respiration rate approximated six breaths/min. Apparently meditative breathing according to these Eastern disciplines sensitizes people to the subtle sensations associated with resonance frequency effects on the baroreflex system. Also, breathing may not be the only way that resonance characteristics of the baroreflex system can be stimulated. In a reanalysis of data in a study by France et al. (2006) on rhythmical muscle tension, we found a resonance effect on HRV with rhythmical muscle tension at a rate of six per min (Lehrer et al., 2009). Vaschillo et al. (2011) replicated this work using muscle tension at various rates, and using rhythmical presentation of emotion-inducing pictures (Vaschillo et al., 2008). This is consistent with the conclusion that resonance effects of breathing six times/min is in fact a result of resonance characteristics of the baroreflex system, and not a peculiar characteristic of respiration.
In a theoretical paper, we examined HRV and HRV biofeedback in light of systems theory. Greater amplitude and greater complexity of HRV both are related to health. Thus the heart rate oscillations at various rates could be considered as control mechanisms, with amplitude related to the strength of various negative feedback loops in a complex control system, with complexity related to the multiplicity of such control loops (Lehrer& Eddie, 2013).
Inflammation. Despite the interesting effects of biofeedback on airway inflammation in asthma, the effects on inflammation remain uncertain, although the effects of inflammation on general resilience appear to be ameliorated by HRVB. In a series of studies we examined the effect on HRV of injecting an inflammatory cytokine, lipopolysaccharide, on heart rate variability, as well as other symptoms of inflammation among healthy young volunteers (Alvarez et al., 2007; Jan et al., 2009; Watson et al., 2008). The volunteers developed symptoms of illness during an 8-hour period, including fever, headache, photophobia, nausea, and vomiting. All frequencies of HRV were depressed, including those associated with sympathetic as well as parasympathetic activity, reflecting a decrease in general allostatic capacity. Low dose steroids were effective in reducing levels of endogenous inflammatory cytokines, but did not reverse the HRV effects (Alverez et al., 2007). In one study in this series, however, we trained participants in HRV biofeedback and had them practice the technique for 10 min out of every hour (Lehrer et al., 2010a). Although no effects on endogenous inflammatory cytokines were noted, all indices of HRV increased, almost to normal levels, suggesting an improvement in general biological resilience. Implications for infectious disease and post-surgical recovery were discussed, as these are conditions under which inflammatory activity can be life threatening, and improved resilience may prove beneficial. However, lack of effects on inflammatory cytokines suggests that increased vagus nerve activity was not sufficient to decrease inflammation. Perhaps the effects on airway inflammation in our asthma study reported above (Lehrer et al., 2018) were specific to the inflammatory cytokine affecting the lung, IL4, which was not measured in the current study, or that the effects of injecting lipopolysaccharide overwhelmed any possible biofeedback effects. Our findings are consistent with the work of others. A recent study by Hasty et al. (2020) found that decreases in HRV reliably predicted increases in C-reactive proteins during the disease process of COVID-19. Nolan et al. (2012) found a decrease in C-reactive proteins among hypertensive patients given HRVB.
Other clinical effects. We have found consistent effects of HRVB in treating depression. We found this incidentally in an uncontrolled study of HRVB to treat fibromyalgia (Hassett et al., 2007) and in in a targeted uncontrolled study of HRVB to treat major depressive disorder (Karavidas et al., 2007). Depression was also decreased, along with somatic symptoms, in patients with somatization disorder given a combination of HRVB and training with both progressive muscle relaxation and autogenic training (Katsamanis et al., 2011). In a study of HRVB given as an add-on to a remotely-administered program of cognitive behavior therapy, Economides et al. (2020) found greater decreases in depression than among a reference population without the add-on. This relationship has been replicated multiple times in controlled studies conducted elsewhere (Lehrer, Vaschillo, et al., 2020). We recently have been involved in an fMRI study of HRVB which seems to explain the specific effect on depression (Nashiro et al., 2021). In this study regular practice of HRVB over two months increased resting-state connectivity between a part of the brain stem involved in generation of emotion (amygdala) and a part of the cortex involved in modulation of emotion (prefrontal cortex cortex), with large oscillatory activity occurring throughout the brain during training. These results were substantially replicated in a study by Schumann et al., 2021.
We have also observed that HRVB has positive effects on a wide array of other conditions. A study by Sakakibara et al. (2013) found an increase in HRV during sleep when HRVB was practice before sleep, and a study by Eddie et al. (2014) found that a course of HRVB produced a greater reduction in substance craving among patients in an inpatient setting than treatment as usual. Feldman et al. (2016) found a reduction in both asthma and panic symptoms among patients with comorbid asthma and panic disorder, but found a similar decrease among patients given instruction in relaxed (but not slow) paced breathing and listening to relaxing music, but they found no relationship between improvement in symptoms and changes in either HRV or end tidal carbon dioxide (Nelson et al., 2020). Kim et al. (2019) did find a correlation between improvement in emotional control and increases in HRV resulting from HRVB training among patients with acquired brain injury. Van der Zwan et al. (2019) found an increase in feelings of well-being among women given HRVB compared with a waiting list control, and a decrease in anxiety symptoms among pregnant women reporting high levels of stress. In a meta-analysis of controlled studies evaluating respiratory retraining as a treatment for anxiety disorders, Leyro et al. (2021) found larger decreases in anxiety among studies employing biofeedback, mostly HRVB, as part of training than among people given other types of respiratory retraining. In a conservative meta-analysis of clinical HRVB effects, examining all measures taken in all studies of HRVB for all conditions, Lehrer, Kaur, et al. (2020) found a moderate effect size across problems and measures, with large effect sizes for improvements in artistic/athletic performance, depression, anger, anxiety, systolic blood pressure, respiratory disorders, and gastrointestinal disorders, with moderate effect sizes for pain, executive/cognitive function, and substance craving, and only small effect sizes for PTSD symptoms, fatigue, diastolic blood pressure, quality of life, sleep, diastolic blood pressure, and, surprisingly, daily stress.
Impact on the Field of HRVB Research
Our protocol of HRVB is often used as a standard for HRVB research. We have demonstrated the mechanisms by which HRVB produces high-amplitudes of HRV and stimulates homeostatic processes (Lehrer et al., 2013). We have done the preliminary studies demonstrating clinical as well as physiological effects of HRVB, and this has interested researchers from many fields. A search of heart rate variability biofeedback in Psycinfo now yields 183 papers.
Recommendations for Future Development of Our Work
We have just scratched the surface of what needs to be known about both the physiological and clinical effects of HRVB. Below are some unanswered research questions that immediately flow from our work.
Mechanisms and Physiological Effects of HRVB
-
1.
We do not know the reason why the phase relationship between heart rate oscillations and respiration is close to zero degrees among younger but not in older people when people breathe at resonance frequency of the baroreflex system. Answering this question may yield important information about the condition of the neurocardiac or cardiovascular system as it changes during the aging process.
-
2.
Our early paper on resonance (Vaschillo et al., 2002) suggests that the vascular tone loop of the baroreflex system may have resonance properties in the very low frequency range (close to 0.02 Hz). Vaschillo and his colleagues have done additional research validating this finding (Vaschillo & Vaschillo, 2020; Vaschillo et al., 2015). What, then, would be the results of doing biofeedback to target these resonance properties? Although it might be done by HRVB in this range, it might be more interesting to determine resonance characteristics and biofeedback effects of direct biofeedback for vascular tone. This might, for example, be done noninvasively by giving biofeedback for pulse transit time, which is considered to be a reasonable proxy measure of vascular tone. Because vascular problems are directly implicated in hypertension, answering this question could have important clinical implications.
-
3.
Other rhythms occur in other physiological systems, e.g. a three per min rhythm in the electrogastrogram (Stern et al., 1987). Might a resonance process occur at this frequency? What is the neurophysiological basis for the rhythm? What methods have the greatest power to stimulate such resonance effects. Breathing? Muscle tension? Walker et al. (1978) found that aspects of the electrogastrogram signal can be controlled voluntarily by biofeedback.
-
4.
What is the relationship between particular brain blood flow changes and various emotional, mental, and neuromuscular effects of HRVB?
Clinical Effects of HRVB
-
1.
For all applications of HRVB, what are the mechanisms of action. Although some of our studies do find changes in HRV amplitudes after a course of successful HRVB for a clinical condition, others find symptom changes without changes in resting HRV, although large effects universally occur during HRV practice sessions. There are sufficient studies using placebo-like controls to indicate that the clinical effects are not due merely to suggestion or a form of Hawthorne effect.
-
2.
For asthma, replication is needed to determine whether clinical effects are due to changes in inflammation. We did not find such a relationship in one study (Lehrer et al., 2018), but this study was done on relatively healthy people where the range for possible clinical improvement was small and the measure of inflammation insensitive. Studies of more severe asthma are warranted with more sensitive measures of airway inflammation, perhaps interleukin levels.
-
3.
Studies of several conditions using a paced breathing control at a frequency higher than resonance frequency still seems to produce clinically significant effects. Is there something about paced breathing at a naturally relaxed rate that produces important psychophysiological effects, and what might the mechanisms be? There is some evidence that breathing slightly away from exact resonance frequency has a slightly smaller clinical effect on blood pressure control (Lin et al., 2012) and anxiety (Steffen et al., 2017). This requires more investigation.
-
4.
Is it possible that longer-standing clinical effects are due to the cumulative immediate effects of HRVB rather than to effects of HRVB on baseline psychophysiological processes? Is it possible, for example, that frequent experiences of improving mood or ending panic attacks by doing resonance frequency breathing may have more enduring cognitive and psychophysiological effects, either from greater sense of self-efficacy in controlling symptoms or from changes in sensitivity in the brain and body to stimuli that produce these symptoms? For asthma, what are the effects of resonance frequency breathing during an asthma exacerbation? Are these responsible for our findings (Lehrer et al., 2004) of not a single asthma exacerbation requiring an increase in asthma medications among patients given HRVB? Indeed, what are the elements in HRVB that help asthma? One possibility, as discussed above, is a decrease in airway inflammation. Another possibility, however, may simply be effects of deep breathing, which may stretch smooth muscles in the airways. It is known that a single deep breath after a dose of methacholine can decrease bronchoconstriction caused by methacholine and improve performance on a methacholine challenge test (Jackson et al., 2004). Other deep breathing methods, from yoga to playing the didgeridoo also seem to help asthma (Eley, 2013). Is it possible that breathing slowly but not at resonance frequency would have exactly the same effect as HRVB? This may be the case even for paced breathing at a faster relaxed respiration rate (Feldman et al., 2016; Lehrer et al., 2018).
-
5.
Our meta-analysis (Lehrer, Kaur, et al., 2020) found smaller HRVB effects for fatigue and PTSD than for anxiety and depression. Is it possible that some dissociative symptoms in PTSD and in fatigue may be expressed in vagal hyperreactivity, and that stimulation of RSA by HRVB may have combined effects of increasing symptoms while the general decrease in autonomic lability decreases them? We did not see evidence for detrimental effects of HRVB on these conditions, but the clinical effects, across studies, tended to be small, possibly due to these mixed effects. Is it possible, then, that stimulation of regulatory processes by methods other than breathing may have stronger effects, e.g., by rhythmical muscle tension? Ditto et al. (2003) presented evidence that this method may be particularly useful for people suffering from episodes of vasovagal reactions during blood donation. Here, rhythmical muscular stimulation at resonance frequency may stimulate a sympathetic branch of the baroreflex system, and improve sympathetically-mediated regulatory processes. This effect may even be stronger if stimulation is at the resonance frequency of the vascular baroreflex system, which is under sympathetic control (Young et al., 2016), while the stimulation of the heart rate component of the baroreflex by paced breathing is primarily vagally mediated (del Paso et al., 2013).
-
6.
How much daily practice of HRVB is needed for lasting clinical and psychophysiological effects? We have prescribed two 20-min practice sessions daily, but few people actually do practice this amount. How much practice is actually needed to strengthen the baroreflex and produce meaningful clinical effects?
-
7.
Might resonance frequency breathing be clinically helpful for people suffering from acute inflammatory reactions, such as those produced by COVID-19 or post-surgically?
-
8.
For acute severe respiratory conditions, might effects on quality of life and oxygenation be better if respiration were in phase with HRV, such that inhalation always occurs during increases in HR in RSA (Hayano et al., 1996)? This normally does not occur in older people breathing as resonance frequency. A zero-degree phase relationship might be expected to maximize gas exchange efficiency. On the other hand, if this frequency is not close to resonance frequency, presumably the effects would be smaller on baroreflex training and possible emotional projections in the brain
-
9.
In general, more replication is needed for application to all clinical conditions. There are very few studies for any specific condition, and these are often from the same laboratory. Not having financial resources necessary for Phase III clinical trials, evidence for biofeedback effects must be obtained from looking at multiple small studies, perhaps using meta-analytic methods. Replication by different investigators is essential for confidence in results.
-
10.
Is stimulation at resonance frequency of the baroreflex system necessarily the best frequency for all conditions? For example, it is known that a healthy electrogastrogram rhythm is at the rate of approximately three times a min (Stern et al., 1987). For gastrointestinal disorders, might it be more beneficial to stimulate the system at this rate rather than at the baroreflex rate closer to six times a min, and might this prove to be a resonance frequency for gastric activity? Might a resonance process occur at three per min in gastrointestinal measures?
References
Airaksinen, K. E., Tahvanainen, K. U., Kuusela, T. A., Huikuri, H. V., Niemela, M. J., Karjalainen, P., & Eckberg, D. L. (1997). Cross spectral analysis in assessment of baroreflex gain in patients with coronary artery disease. Annals of Noninvasive Electrocardiology, 2, 229–235. https://doi.org/10.1111/j.1542-474x.1997.tb00331.x
Alvarez, S. M., Katsamanis Karavidas, M., Coyle, S. M., Lu, S. E., Macor, M., Oikawa, L. O., Lehrer, P. M., Calvano, S. E., & Lowry, S. F. (2007). Low-dose steroid alters in vivo endotoxin-induced systemic inflammation but does not influence autonomic dysfunction. Journal of Endotoxin Research, 13, 358–368. https://doi.org/10.1177/096805190708646
Crowne, D. P., & Marlowe, D. (1960). A new scale of social desirability independent of psychopathology. Journal of Consulting Psychology, 24, 349–354. https://doi.org/10.1037/h0047358
del Paso, G. A. R., Langewitz, W., Mulder, L. J. M., van Roon, A., & Duschek, S. (2013). The utility of low frequency heart rate variability as an index of sympathetic cardiac tone: A review with emphasis on a reanalysis of previous studies. Psychophysiology, 50(477), 487. https://doi.org/10.1111/psyp.12027
Ditto, B., Wilkins, J.-A., France, C. R., Lavoie, P., & Adler, P. S. J. (2003). On-site training in applied muscle tension to reduce vasovagal reactions to blood donation. Journal of Behavioral Medicine, 26, 53–65. https://doi.org/10.1023/A:1021795022380
Eccles, J. A., Owens, A. P., Mathias, C. J., Umeda, S., & Critchley, H. D. (2015). Neurovisceral phenotypes in the expression of psychiatric symptoms. Frontiers in Neuroscience, 9, 4. https://doi.org/10.3389/fnins.2015.00004
Eckberg, D. L., & Sleight, P. (1992). Human baroreflexes in health and disease. Clarendon Press.
Economides, M., Lehrer, P., Ranta, K., Nazander, A., Hilgert, O., Raevuori, A., Gevirtz, R., Khazan, I., & Forman-Hoffman, V. L. (2020). Feasibility and efficacy of the addition of heart rate variability biofeedback to a remote digital health intervention for depression. Applied Psychophysiology & Biofeedback, 45, 75–86. https://doi.org/10.1007/s10484-020-09458-z
Eddie, D., Kim, C., Lehrer, P., Deneke, E., & Bates, M. E. (2014). A pilot study of brief heart rate variability biofeedback to reduce craving in young adult men receiving inpatient treatment for substance use disorders. Applied Psychophysiology & Biofeedback, 39, 181–192. https://doi.org/10.1007/s10484-014-9251-zx
Eley, R. (2013). The potential effects of the didgeridoo as an indigenous intervention for Australian aborigines: A post analysis. Music and Medicine, 5, 84–92. https://doi.org/10.1177/1943862113476306
Feldman, J. M., Lehrer, P. M., Hochron, S. M., & Schwartz, G. E. (2002). Defensiveness and individual response stereotypy in asthma. Psychosomatic Medicine, 64, 294–301. https://doi.org/10.1097/00006842-200203000-00013
Feldman, J. M., Matte, L., Interian, A., Lehrer, P. M., Lu, S. E., Scheckner, B., Steinberg, D. M., Oken, T., Kotay, A., Sinha, S., & Shim, C. (2016). Psychological treatment of comorbid asthma and panic disorder in latino adults: Results from a randomized controlled trial. Behaviour Research & Therapy, 87, 142–154. https://doi.org/10.1016/j.brat.2016.09.007
France, C. R., France, J. L., & Patterson, S. M. (2006). Blood pressure and cerebral oxygenation responses to skeletal muscle tension: A comparison of two physical maneuvers to prevent vasovagal reactions. Clinical Physiology & Functional Imaging, 26, 21–25. https://doi.org/10.1111/j.1475-097X.2005.00642.x
Garcia-Araujo, A. S., Pires Di Lorenzo, V. A., Labadessa, I. G., Jurgensen, S. P., Di Thommazo-Luporini, L., Garbim, C. L., & Borghi-Silva, A. (2015). Increased sympathetic modulation and decreased response of the heart rate variability in controlled asthma. Journal of Asthma, 52, 246–253. https://doi.org/10.3109/02770903.2014.957765
Gellhorn, E., & Loofbourrow, G. N. (1963). Emotions and emotional disorders: A neurophysiological study. Hoeber Medical Division, Harper and Row.
Gevirtz, R., Schwartz, M. S., & Lehrer, P. M. (2016). Cardiorespiratory measurement and assessment in applied psychophysiology. In M. S. Schwartz & F. Andrasik (Eds.), Biofeedback: a practitioner’s guide (4th ed., pp. 85–97). New York: Guilford.
Grodins, F. S. (1963). Control theory and biological systems. Columbia University Press.
Hassett, A. L., Radvanski, D. C., Vaschillo, E. G., Vaschillo, B., Sigal, L. H., Karavidas, M. K., Buyske, S., & Lehrer, P. M. (2007). A pilot study of the efficacy of heart rate variability (hrv) biofeedback in patients with fibromyalgia. Applied Psychophysiology & Biofeedback, 32, 1–10. https://doi.org/10.1007/s10484-006-9028-0
Hasty, F., Garcia, G., Davila, C. H., Wittels, S. H., Hendricks, S., & Chong, S. (2020). Heart rate variability as a possible predictive marker for acute inflammatory response in covid-19 patients. Military Medicine. https://doi.org/10.1093/milmed/usaa405
Hayano, J., Yasuma, F., Okada, A., Mukai, S., & Fujinami, T. (1996). Respiratory sinus arrhythmia. A phenomenon improving pulmonary gas exchange and circulatory efficiency. Circulation, 94, 842–847. https://doi.org/10.1161/01.CIR.94.4.842
Isenberg, S. A., Lehrer, P. M., & Hochron, S. (1992). The effects of suggestion and emotional arousal on pulmonary function in asthma: A review and a hypothesis regarding vagal mediation. Psychosomatic Medicine, 54, 192–216. https://doi.org/10.1097/00006842-199203000-00006
Jackson, A. C., Murphy, M. M., Rassulo, J., Celli, B. R., & Ingram, R. H. (2004). Deep breath reversal and exponential return of methacholine-induced obstruction in asthmatic and nonasthmatic subjects. Journal of Applied Physiology, 96, 137–142. https://doi.org/10.1152/japplphysiol.00504.2003
Jan, B. U., Coyle, S. M., Oikawa, L. O., Lu, S. E., Calvano, S. E., Lehrer, P. M., & Lowry, S. F. (2009). Influence of acute epinephrine infusion on endotoxin-induced parameters of heart rate variability: A randomized controlled trial. Annals of Surgery, 249, 750–756. https://doi.org/10.1097/SLA.0b013e3181a40193
Karavidas, M. K., Lehrer, P. M., Vaschillo, E., Vaschillo, B., Marin, H., Buyske, S., Malinovsky, I., Radvanski, D., & Hassett, A. (2007). Preliminary results of an open label study of heart rate variability biofeedback for the treatment of major depression. Applied Psychophysiology & Biofeedback, 32, 19–30. https://doi.org/10.1007/s10484-006-9029-z
Katsamanis, M., Lehrer, P. M., Escobar, J. I., Gara, M. A., Kotay, A., & Liu, R. (2011). Psychophysiologic treatment for patients with medically unexplained symptoms: A randomized controlled trial. Psychosomatics, 52, 218–229. https://doi.org/10.1016/j.psym.2011.01.015
Kim, S., Zemon, V., Lehrer, P., McCraty, R., Cavallo, M. M., Raghavan, P., Ginsberg, J. J., & Foley, F. W. (2019). Emotion regulation after acquired brain injury: A study of heart rate variability, attentional control, and psychophysiology. Brain Injury, 33, 1012–1020. https://doi.org/10.1080/02699052.2019.1593506
Lehrer, P. (2013). History of heart rate variability biofeedback research: A personal and scientific voyage. Biofeedback, 41, 88–97. https://doi.org/10.5298/1081-5937-41.3.03
Lehrer, P., & Eddie, D. (2013). Dynamic processes in regulation and some implications for biofeedback and biobehavioral interventions. Applied Psychophysiology & Biofeedback, 38, 143–155. https://doi.org/10.1007/s10484-013-9217-6
Lehrer, P., & Gevirtz, R. (2014). Heart rate variability biofeedback: How and why does it work? Frontiers in Psychology, 21, 756. https://doi.org/10.3389/fpsyg.2014.00756
Lehrer, P. M., & Gevirtz, R. (2016). Cardiorespiratory biofeedback. In M. S. Schwartz & F. Andrasik (Eds.), Biofeedback: A practitioner’s guide (4th ed., pp. 196–216). NY: Guilford.
Lehrer, P. M., & Gevirtz, R. (2018). Heart rate variability biofeedback. In J. Magnavita (Ed.), Incorporating technology in mental health practice (pp. 123–142). American Psychological Association.
Lehrer, P., Hochron, S. M., Rausch, L., & Carr, R. (1994a). The effects of atropine on respiratory sinus arrhythmia in asthma. Respiratory Medicine, 88, 357–361. https://doi.org/10.1016/0954-6111(94)90041-8
Lehrer, P., Hochron, S. M., Rausch, L., & Carr, R. (1994b). Effects of aerosol ipratropium bromide on cardiac vagal tone. Chest, 105, 1701–1704. https://doi.org/10.1378/chest.105.6.1701
Lehrer, P., Hochron, S., Carr, R., Edelberg, R., Hamer, R., Jackson, A., & Porges, S. (1996). Behavioral task-induced brochodilation in asthma during active and passive tasks: A possible cholinergic link to psychologically-induced airway changes. Psychosomatic Medicine, 58, 413–422. https://doi.org/10.1097/00006842-199609000-00004
Lehrer, P., Generelli, P., & Hochron, S. (1997). The effect of facial and trapezius muscle tension on respiratory impedance in asthma. Applied Psychophysiology & Biofeedback, 22(1), 43–54. https://doi.org/10.1023/A:1026237725681
Lehrer, P. M., Hochron, S. M., Mayne, T., Isenberg, S., Lasoski, A. M., Carlson, V., Gilchrist, J., & Porges, S. (1997). Relationship between changes in EMG and respiratory sinus arrhythmia in a study of relaxation therapy for asthma. Applied Psychophysiology & Biofeedback, 22(3), 183–191. https://doi.org/10.1023/A:1026263826106
Lehrer, P., Sasaki, Y., & Saito, Y. (1999). Zazen and cardiac variability. Psychosomatic Medicine, 61, 812–821. https://doi.org/10.1097/00006842-199911000-00014
Lehrer, P., Smetankin, A., & Potapova, T. (2000). Respiratory sinus arrhythmia biofeedback therapy for asthma: A report of 20 unmedicated pediatric cases using the Smetankin method. Applied Psychophysiology & Biofeedback, 25, 193–200. https://doi.org/10.1023/a:1009506909815
Lehrer, P., Vaschillo, E., Vaschillo, B., Lu, S.-E., Eckberg, D. L., Edelberg, R., Shih, W. J., Lin, Y., Kuusela, T. A., Tahvanainen, K. U. O., & Hamer, R. (2003). Heart rate variability biofeedback increases baroreflex gain and peak expiratory flow. Psychosomatic Medicine, 65, 796–805. https://doi.org/10.1097/01.psy.0000089200.81962.19
Lehrer, P., Vaschillo, E., Vaschillo, B., Lu, S.-E., Scardella, A., Siddique, M., & Habib, R. (2004). Biofeedback treatment for asthma. Chest, 126, 352–361. https://doi.org/10.1378/chest.126.2.352
Lehrer, P., Vaschillo, E., Lu, S.-E., Eckberg, D., Vaschillo, B., Scardella, A., & Habib, R. (2006). Heart rate variability biofeedback: Effects of age on heart rate variability, baroreflex gain, and asthma. Chest, 129, 278–284. https://doi.org/10.1378/chest.129.2.278
Lehrer, P., Vaschillo, E., Trost, Z., & France, C. R. (2009). Effects of rhythmical muscle tension at 0.1hz on cardiovascular resonance and the baroreflex. Biological Psychology, 81, 24–30. https://doi.org/10.1016/j.biopsycho.2009.01.003
Lehrer, P., Karavidas, M. K., Lu, S.-E., Coyle, S. M., Oikawa, L. O., Macor, M., Calvano, S. E., & Lowry, S. F. (2010a). Voluntarily produced increases in heart rate variability modulate autonomic effects of endotoxin induced systemic inflammation: An exploratory study. Applied Psychophysiology & Biofeedback, 35, 303–315. https://doi.org/10.1007/s10484-010-9139-5
Lehrer, P., Karavidas, M., Lu, S. E., Vaschillo, E., Vaschillo, B., & Cheng, A. (2010b). Cardiac data increase association between self-report and both expert ratings of task load and task performance in flight simulator tasks: An exploratory study. International Journal of Psychophysiology, 76, 80–87. https://doi.org/10.1016/j.ijpsycho.2010.02.006
Lehrer, P., Vaschillo, B., Zucker, T., Graves, J., Katsamanis, M., Aviles, M., & Wamboldt, F. (2013). Protocol for heart rate variability biofeedback training. Biofeedback, 41, 98–109. https://doi.org/10.5298/1081-5937-41.3.08
Lehrer, P. M., Irvin, C. G., Lu, S.-E., Scardella, A., Roehmheld-Hamm, B., Aviles-Velez, M., Graves, J., Vaschillo, E. G., Vaschillo, B., Hoyte, F., & Wamboldt, F. S. (2018). Heart rate variability biofeedback does not substitute for asthma steroid controller medication. Applied Psychophysiology & Biofeedback, 43(1), 57–71. https://doi.org/10.1007/s10484-017-9382-0
Lehrer, P., Kaur, K., Sharma, A., Shah, K., Huseby, R., Bhavsar, J., & Zhang, Y. (2020). Heart rate variability biofeedback improves emotional and physical health and performance: A systematic review and meta analysis. Applied Psychophysiology & Biofeedback, 45(3), 100–129. https://doi.org/10.1007/s10484-020-09466-z
Lehrer, P. M., Vaschillo, E. G., & Vidali, V. (2020). Heart rate and breathing are not always in phase during resonance frequency breathing. Applied Psychophysiology & Biofeedback, 45(3), 109–129. https://doi.org/10.1007/s10484-020-09459-y
Leyro, T. M., Versella, M. V., Yang, M. J., Brinkman, H. R., Hoyt, D. L., & Lehrer, P. (2021). Respiratory therapy for the treatment of anxiety: Meta-analytic review and regression. Clinical Psychology Review, 84, 101980. https://doi.org/10.1016/j.cpr.2021.101980
Lin, G., Xiang, Q., Wang, S., Wang, S., Chen, S., Shao, L., Zhao, Y., & Wang, T. (2012). Heart rate variability biofeedback decreases blood pressure in prehypertensive subjects by improving autonomic function and baroreflex. Journal of Alternative & Complementary Medicine, 18, 143–152. https://doi.org/10.1089/acm.2010.0607
Nashiro, K., Min, J., Yoo, H. J., Cho, C., Bachman, S. L., Dutt, S., Thayer, J. F., Lehrer, P., Feng, T., Mercer, N., Nasseri, P., Wang, D., Chang, C., Marmarelis, V. Z., Narayanan, S., Nation, D. A., & Mather, M. (2021). Enhancing the brain’s emotion regulation capacity with a randomised trial of a 5-week heart rate variability biofeedback intervention. MedRxiv, 130, 54. https://doi.org/10.1101/2021.09.28.21264206
National Asthma Education and Prevention Program. (2007). Expert panel report 3 (epr-3): Guidelines for the diagnosis and management of asthma-summary report 2007. Journal of Allergy & Clinical Immunology, 120, S94-138.
Nelson, K. L., Lu, S. E., Oken, T., Lehrer, P. M., & Feldman, J. M. (2020). Further exploration of treatment response in Latinos with comorbid asthma and panic disorder: A brief report of hrv and etco2 as potential mediators of treatment response. Applied Psychophysiology & Biofeedback, 45, 67–74. https://doi.org/10.1007/s10484-020-09454-3
Nolan, R. P., Floras, J. S., Ahmed, L., Harvey, P. J., Hiscock, N., Hendrickx, H., & Talbot, D. (2012). Behavioural modification of the cholinergic anti-inflammatory response to c-reactive protein in patients with hypertension. Journal of Internal Medicine, 272, 161–169. https://doi.org/10.1111/j.1365-2796.2012.02523.x
Pavlov, V. A., & Tracey, K. J. (2012). The vagus nerve and the inflammatory reflex–linking immunity and metabolism. Nature Reviews Endocrinology, 8, 743–754. https://doi.org/10.1038/nrendo.2012.189
Porges, S. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, self-regulation. Norton.
Rosenkranz, M. A., Esnault, S., Christian, B. T., Crisafi, G., Gresham, L. K., Higgins, A. T., Moore, M. N., Moore, S. M., Weng, H. Y., Salk, R. H., Busse, W. W., & Davidson, R. J. (2016). Mind-body interactions in the regulation of airway inflammation in asthma: A PET study of acute and chronic stress. Brain, Behavior, and Immunity, 58, 18–30. https://doi.org/10.1016/j.bbi.2016.03.024
Sakakibara, M., Hayano, J., Oikawa, L. O., Katsamanis, M., & Lehrer, P. (2013). Heart rate variability biofeedback improves cardiorespiratory resting function during sleep. Applied Psychophysiology & Biofeedback, 38, 265–271. https://doi.org/10.1007/s10484-013-9232-7
Sargunaraj, D., Lehrer, P., Hochron, S. M., Rausch, L., Edelberg, R., & Porges, S. (1996). Cardiac Rhythm Effects of.125Hz Paced breathing through a resistive load: Implications for paced breathing therapy and porges’ poly-vagal theory. Biofeedback and Self-Regulation, 121, 131–147. https://doi.org/10.1007/BF02284692
Schumann, A., de la Cruz, F., Köhler, S., Brotte, L., & Bär, K. J. (2021). The Influence of heart rate variability biofeedback on cardiac regulation and functional brain connectivity. Frontiers in Neuroscience, 15, 691988. https://doi.org/10.3389/fnins.2021.691988
Scott, G. D., & Fryer, A. D. (2012). Role of parasympathetic nerves and muscarinic receptors in allergy and asthma. Chemical Immunology & Allergy, 98, 48–69. https://doi.org/10.1159/000336498
Sharpe, E., Lacombe, A., Sadowski, A., Phipps, J., Heer, R., Rajurkar, S., Hanes, D., Jindal, R. D., & Bradley, R. (2021). Investigating components of pranayama for effects on heart rate variability. Journal of Psychosomatic Research, 148, 110569. https://doi.org/10.1016/j.jpsychores.2021.110569
Sledge, W. H. (1978). Antecedent psychological factors in the onset of vasovagal syncope. Psychosomatic Medicine, 40, 568–579. https://doi.org/10.1097/00006842-197811000-00004
Song, H.-S., & Lehrer, P. (2003). The effects of specific respiratory rates on heart rate and heart rate variability. Applied Psychophysiology & Biofeedback, 28, 13–24. https://doi.org/10.1023/a:1022312815649
Steffen, P., Austin, T., DeBarros, A., & Brown, T. (2017). The impact of resonance frequency breathing on measures of heart rate variability, blood pressure, and mood. Frontiers in Public Health. https://doi.org/10.3389/fpubh.2017.00222
Stern, R. M., Koch, K. L., Stewart, W. R., & Vasey, M. W. (1987). Electrogastrography: Current issues in validation and methodology. Psychophysiology, 24, 55–64. https://doi.org/10.1111/j.1469-8986.1987.tb01862.x
van der Zwan, J. E., Huizink, A. C., Lehrer, P. M., Koot, H. M., & de Vente, W. (2019). The effect of heart rate variability biofeedback training on mental health of pregnant and non-pregnant women: a randomized controlled trial. International Journal of Environmental Research & Public Health [electronic Resource]. https://doi.org/10.3390/ijerph16061051
Vaschillo, B., & Vaschillo, E. G. (2020). Can arterial elasticity be estimated from heart rate variability response to paced 0.66 Hz sighing? Psychophysiology, 57, e13552. https://doi.org/10.1111/psyp.13552
Vaschillo, E., Vaschillo, B., & Lehrer, P. (2004). Heartbeat synchronizes with respiratory rhythm only under specific circumstances. Chest, 126, 1385–1386. https://doi.org/10.1378/chest.126.4.1385-a
Vaschillo, E., Vaschillo, B., & Lehrer, P. (2006). Characteristics of resonance in heart rate variability stimulated by biofeedback. Applied Psychophysiology & Biofeedback, 31, 129–142. https://doi.org/10.1007/s10484-006-9009-3
Vaschillo, E. G., Bates, M. E., Vaschillo, B., Lehrer, P., Udo, T., Mun, E. Y., & Ray, S. (2008). Heart rate variability response to alcohol, placebo, and emotional picture cue challenges: Effects of 0.1-hz stimulation. Psychophysiology, 45, 847–858. https://doi.org/10.1111/j.1469-8986.2008.00673.x
Vaschillo, E., Lehrer, P., Rishe, N., & Konstantinov, M. (2002). Heart rate variability biofeedback as a method for assessing baroreflex function: A preliminary study of resonance in the cardiovascular system. Applied Psychophysiology & Biofeedback, 27, 1–27.
Vaschillo, E. G., Vaschillo, B., Buckman, J. F., Nguyen-Louie, T., Heiss, S., Pandina, R. J., & Bates, M. E. (2015). The effects of sighing on the cardiovascular system. Biological Psychology, 106, 86–95. https://doi.org/10.1016/j.biopsycho.2015.02.007
Vaschillo, E. G., Vaschillo, B., Pandina, R. J., & Bates, M. E. (2011). Resonances in the cardiovascular system caused by rhythmical muscle tension. Psychophysiology, 48, 927–936. https://doi.org/10.1111/j.1469-8986.2010.01156.x
Walker, B. B., Lawton, C. A., & Sandman, C. A. (1978). Voluntary control of electrogastric activity. Psychosomatic Medicine, 40, 610–619. https://doi.org/10.1097/00006842-197812000-00003
Watson, S., Karavidas, M., Kunar, A., Coyle, S., Macor, M., Lehrer, P., Calvano, S., & Lowry, S. (2008). Influence of gender on endotoxin-induced parameters of heart rate variability and innate immune response. Journal of the American College of Surgeons, 207, 39–40.
Young, B. E., Kaur, J., & Vranish, J. R. (2016). Methodological assessment of sympathetic vascular transduction. The Journal of Physiology, 594, 6809–6810. https://doi.org/10.1113/JP273436
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lehrer, P. My Life in HRV Biofeedback Research. Appl Psychophysiol Biofeedback 47, 289–298 (2022). https://doi.org/10.1007/s10484-022-09535-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10484-022-09535-5