
Abstract
Background
In this study, the effects of long-term pregabalin use on the choroid and retinal nerve fiber layer were investigated in the fibromyalgia disease.
Methods
The patient group consisted of 41 fibromyalgia patients using pregabalin. The control group consisted of 41 newly diagnosed fibromyalgia patients who had not received any treatment yet. Choroidal and retinal nerve fiber layer thickness measurements were performed with Cirrus HD-OCT (Carl Zeiss Meditec Inc., Dublin, CA, USA) 30 minutes after pupil dilation with 1% tropicamide.
Results
There was no difference in subfoveal choroidal thickness, nasal choroidal thickness and temporal choroidal thickness between the patient and control groups (p > 0.05). Increasing the duration of drug use within the patient group was found to thin the retinal nerve fiber layer (p < 0.05).
Conclusion
We found that pregabalin had no effect on the choroid, while it had a thinning effect for retinal nerve fiber layer. It is recommended not to be preferred pregabalin in fibromyalgia patients with retinal nerve fiber layer damage such as diabetic retinopathy and glaucoma. Patients treated with pregabalin should have regular control in the ophthalmology clinic.
Similar content being viewed by others

Introduction
Fibromyalgia (FM) is a clinical picture that includes many symptoms such as widespread chronic pain and fatigue, sleep disturbance, cognitive dysfunction, and depressive episodes [1]. The prevalence of fibromyalgia in the general population ranges from 0.2 to 6.6% [2]. Pregabalin is an α2-δ calcium channel ligand and has been approved by many countries such as the United States and Japan as the first choice in FM treatment [3].
It is known that various systemic diseases and topical or systemic drug use are associated with retinal toxicity [4]. Ocular side effects such as blurred vision, diplopia, ocular pain, photopsia and irritation have been reported for pregabalin which has a wide area of use such as the treatment of epilepsy, neuropathic pain and anxiety disorders, and can be used for many years, but its retinal and choroidal effects are still unknown [5].
The choroid consists of a vascular network that acts as a blood supply for the outer retina, optic nerve, and avascular fovea. The choroid has dense fiber plexuses innervated by both the sympathetic and parasympathetic parts of the autonomic nervous system. Additionally, there are primary afferent sensory fibers that lead to the trigeminal ganglion via the ophthalmic nerve [6]. Changes in choroidal circulation, autonomic nervous system inputs, or inflammation can lead to a change in choroidal thickness. Enhanced-depth imaging optical coherence tomography (EDI-OCT) allows fast and precise measurement of choroidal thickness. Therefore, the effects of various factors such as age, gender, smoking, and many local or systemic diseases on choroidal thickness have been evaluated in recent years [7]. In the literature, serous retinal detachment has been reported after the usage of high dose pregabalin, possibly due to increased choroidal vascular permeability caused by the effect of pregabalin [5].
Since the retina is an anatomical extension of the brain, it is thought that the retinal changes may occur in parallel with changes in the nervous system. Therefore, retinal nerve fiber layer (RNFL) examination with OCT has attracted considerable attention in terms of neurodegenerative diseases and effects of neurological drugs [8]. On the other hand, in rat retinas, α2-δ3 and α2-subunits were found in photoreceptors, bipolar cells, amacrine cells, and most cells in the ganglion cell layer of the retina [9]. We think that retinal interactions may occur with the pregabalin binding to the α2-δ subunits of presynaptic voltage-dependent calcium channels. There is no study yet reporting the effects of long-term pregabalin use on the retina and choroid. Therefore, in this study, we wanted to investigate the thickness changes that may occur in RNFL and choroid in chronic use of pregabalin.
Material-Methods
This cross-sectional trial was performed at the Clinic of Ophthalmology, Orthopaedics and Traumatology and Rheumatology, Niğde Ömer Halisdemir University Hospital, between 2018 and 2020. The study protocol was approved by the Ethics Review Board of Niğde Ömer Halisdemir University Hospital and written consent was obtained from each patient before the eye examination. The study was conducted in accordance with the principles of the Declaration of Helsinki.
The study group was formed by selecting from the patients with a diagnosis of FM who were sent to our clinic for eye examination by the orthopaedics and rheumatology department of our hospital. The study included 41 FM patients who did not have any eye disease and were treated with only 300 mg pregabalin for patient group and 41 newly diagnosed FM patients who were not treated yet for the control group. The patient and control groups consisted of volunteers who did not have any eye pathology except refractive error, had full vision in both eyes, and were similar in age and gender. In both groups, patients with myopic, hyperopic, or astigmatic refractive errors greater than 3.0 dioptres (D), patients with ocular disease or ocular surgery, and patients who were under 18, pregnant, or breastfeeding were excluded from the study. Patients with systemic disease other than FM in both groups were also excluded from the study.
Age, gender, clinical information, and the detailed medical history of all cases were recorded. An ophthalmic examination including best-corrected visual acuity, slit-lamp biomicroscopy, intraocular pressure (IOP) measurements in primary gaze position with non-contact tonometry, fundus evaluation after pupil dilatation using a 90.0 D lens, colour vision, direct-indirect pupillary reactions, relative afferent pupil defect (RAPD), and eye movements was performed. There was a high correlation between the measurements of the right and left eyes, and the right eye measurements were taken in the patient and control groups.
Choroidal thickness measurement with EDI-Optical Coherence Tomography
Choroidal thickness measurement was performed with Cirrus HD-OCT (Carl Zeiss Meditec Inc., Dublin, CA, USA) 30 minutes after pupil dilation with 1% tropicamide.
HD 5 Line Raster protocol was reduced to a single line and shot. Images with signal strength lower than 6 were excluded in the study. The choroid was imaged in the Cirrus HD-OCT with EDI mode. The subfoveal choroidal thickness and choroidal thicknesses at points 500 µm, 1000 µm, and 1500 µm temporal and nasal to the fovea were measured. Temporal and nasal choroidal thicknesses were calculated by taking the average of 3 choroidal thicknesses measured at 500-1000-1500 micron intervals from the subfoveal region. Since manual measurements were made, measurements were repeated by two independent persons.
Retinal nerve fiber layer thickness measurement with Optical Coherence Tomography
RNFL thickness measurement was performed with Cirrus HD-OCT (Carl Zeiss Meditec Inc., Dublin, CA, USA) 30 minutes after pupil dilation with tropicamide 1%. Images with signal strength lower than 6 were excluded in the study. RNFL thickness is determined by an automatic computer algorithm without the need for a user or reference plane.
Statistical analysis
Statistical analysis was performed in STATA 14 package program. Numerical variables were summarized with mean ± standard deviation [minimum - maximum] values. Categorical variables were shown with numbers and percentages. Normality of numerical variables was examined by Kolmogorov Smirnov test, and homogeneity of variances was examined by Levene test. Whether there was a difference between the two groups in terms of numerical variables was done by t test in independent groups if parametric test assumptions were met. If not provided, it was examined using the Mann Whitney U test. Multiple regression analysis was used to reveal independent factors affecting choroidal and RNFL thickness. Pearson Correlation test was used to determine the intercorrelation between eyes. Power analysis was executed by using G*Power 3.1. The analysis was performed using a two-tailed test, a strong effect size (d = 0.85) and an alpha of 0.05, and resulted in a sample size of minimum 37 patients for each group to achieve a power of 0,95. P < 0.05 was accepted statistically significant.
Results
In Table 1, the difference between the patient and control groups in terms of age and gender was tested, and it was found that there was no difference between the groups (p: 0.458 and 0.803 respectively).
High correlation was found between the right and left eyes in subfoveal choroidal thickness (SFCT), nasal choroidal thickness (NCT), temporal choroidal thickness (TCT) and RNFL thickness. (p = 0.000, r = 0.981; p = 0.000, r = 0.993; p = 0.000, r = 0.915; p = 0.000, r = 0.992 respectively)
In Table 2, SFCT, NCT, TCT and RNFL values of the right eyes were compared between the pregabalin group and the control group (p: 0.788, 0.756, 0.562, 0.003 respectively). When we evaluated the p-value for statistical significance, the right RNFL value in the group using pregabalin was lower than the control group, and the difference between them was statistically significant.
In Table 3, the changes in the right eye values of the pregabalin group were tried to be determined using multiple linear regression analysis. In this analysis, after controlling the age and gender variables of the pregabalin group compared to the control group, we attempted to determine whether there was a statistically significant difference between the pregabalin group and the control group. Pregabalin use lost its statistical significance in terms of variables in the right eye (p: 0.180). It was determined that the age variable was negative and significant in almost all variables. This shows that as age increases, variables in the right eye are negatively affected.
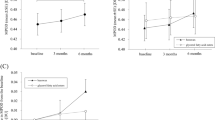
In Table 4, the duration of drug used on FM patients taking pregabalin is used as an independent variable. When we look at the table, it was found that RNFL variables decreased as the duration of drug use was extended, and this decrease was statistically significant at the level of 1% (p: 0.000). No effect of the duration of medicine use on other variables was found. The RNFL results of male patients in the same age group according to the duration of drug use are illustrated in the Fig. 1.

a Right RNFL image of 52-year-old male patient newly diagnosed with FM. b Right RNFL image of 49-year-old male patient treated with pregabalin for 2 years. c Right RNFL image of 53-year-old male patient treated with pregabalin for 4 years. d Right RNFL image of 56-year-old male patient treated with pregabalin for 6 years.
When the pregabalin group was examined in terms of duration of drug use; there were 5 patients in between 0-12 months, 5 patients in between 12-24 months, 13 patients in between 24-36 months, 3 patients in between 36-48 months, and 15 patients in over 48 months.
Discussion
To our knowledge, our study is the first study evaluating the effect of chronic pregabalin usage on choroid and RNFL in FM patients. While no effect of long-term drug use on choroid was observed in our study, a significant thinning in RNFL was detected. Although thinning was detected in RNFL in comparison to the control group, no significant difference was found in the multiple regression analysis. This may be due to the higher number of patients using drugs for less than 4 years in the pregabalin group.
Although the mechanism of action of pregabalin is not fully understood, it is explained by the fact that it reduces the release of many excitatory neurotransmitters such as glutamate, noradrenaline and substance P by modulating the depolarization-induced calcium flow [10]. It has also been shown to reduce sympathetic nervous system activity and inhibit sympathetically sustained pain [11]. Parveen et al. reported that oral pregabalin could be an effective premedication to alleviate the sympathetic response to tracheal intubation [12]. The choroidal circulation, which is structurally composed of branches of the ciliary arteries, is controlled neurogenically, unlike retinal vessels. Sympathetic innervation includes noradrenergic and neuropeptide fibers, while parasympathetic nerves are mainly cholinergic. Therefore, local mediators and sympathetic and parasympathetic systems are thought to play a role in changing choroidal thickness. In other words, inflammatory or pharmacological factors that might affect the autonomic nervous system may affect the choroid and cause perfusion changes [13]. Toledo et al. reported that the activity of Edinger-Westphalia nucleus neurons, which are responsible for the control of miosis and choroidal blood flow in birds, is mediated by glutamate [14]. Cuthbertson et al. showed that ciliary ganglion innervation affects choroidal blood flow in the upper and temporal parts of the eye in pigeons [15]. de Hoz R et al. reported that substance P positive intrinsic choroidal neurons are abundant especially in the central choroid and peripheral sensory innervation may play a role in this mechanism while regulating choroidal blood flow [16]. The choroidal blood flow and hence the thickness of the choroid are likely to be affected, since pregabalin reduces sympathetic system activity and reduces the release of many excitatory neurotransmitters such as glutamate, noradrenaline and substance P. To the best of our knowledge, there is no study examining the interaction between choroid and pregabalin in the literature. But Tanyıldız et al. mentioned that serous retinal detachment occurred by the increase in choroidal vessel permeability due to the use of high-dose pregabalin [5]. In our study, which we planned in line with this information, we did not see any effect of drug use on the choroid.
In recent years, measurement of RNFL thickness with OCT has become a valuable diagnostic tool to detect the effect of various drugs and neurodegenerative diseases in the retina [17,18,19]. Since the retina is of neuroectoderm origin, it has been reported that α2-δ subunits, which are the target of pregabalin, are found in photoreceptors, bipolar cells, amacrine cells and the ganglion cell layer of the retina [9]. However, there is no study that directly examines the effect of the pregabalin on RNFL. The effect of pregabalin in ocular areas such as diabetic retinopathy and glaucoma has been studied [20,21,22]. Ali et al. reported that in diabetic retinopathy in rats, pregabalin partially alleviated retinal apoptosis by reducing glutamate, and therefore pregabalin can be used in the treatment of diabetic retinopathy [20]. Moriya et al. reported the neuroprotective effects of pregabalin in a rat facial nerve avulsion model [23]. Ibrahim et al. mentioned the effect of pregabalin in reducing eye tension, and perhaps this result may have an effect that can prevent RNFL thinning in glaucoma [22]. Despite the neuroprotective effects of pregabalin reported in the literature, there are also studies reporting that the drug is neurotoxic. In a study investigating the effects of long-term and high-dose pregabalin use in rats, it was found that pregabalin increased oxidative stress and induced neuronal apoptosis in cerebral cortical tissue [24]. In a very recently published study, chronic use of pregabalin in rats was examined and it was found that chronic drug use increased apoptosis and gliosis as a result of oxidative stress in histological frontal cortex samples [25]. Kamel reported the neurotoxic effects in chronic use of pregabalin in rat brains [26]. Ninomiya et al. mentioned the retinal dysfunction effect of pregabalin. They showed that 10 months of pregabalin use can cause erroneous synaptic transfer from rod/cone photoreceptors to bipolar cells in the patient [27]. In addition, retinal teratogenicity of pregabalin in the chick embryo model was investigated by Seçinti, and it was reported that the use of pregabalin during pregnancy may be teratogenic due to damage to the retinal layers [28]. Considering the literature studies, it is highly probable that pregabalin has an effect on retinal cells, but no definite information has yet been revealed in terms of its mechanism of action and results. This may be due to the fact that its effect occurs by reducing the release of multiple neurotransmitters and this multifactorial situation also leads to more complex results. In our study, we found a significantly thinner RNFL in contrary to the protective effect.
What needs to be mentioned in our study is literature studies reporting that FM affects choroidal thickness and RNFL. Ulusoy et al. showed that choroidal thickness decreased in patients with FM and was associated with disease activity [29]. Garcia-Martin et al. reported that FM was associated with RNFL thinning [30]. However, in both studies, the medical treatment patients received was not mentioned. It is doubtful that this effect is due to FM.
One of the confounding factors in our study; since the control group consisted of newly diagnosed FM patients, the similarity between the two groups in terms of disease duration is doubtful. It was impossible for us to determine how long the newly diagnosed patients had been suffering from the disease. If we were to create a similar group in terms of disease duration from the moment of diagnosis, this time other pharmacological agents used in the treatment would have interacted. However, since the eye effects of FM are not certain, this cannot be said to be a definite limiting factor. In the statistical results made considering these conditions, we found that the use of pregabalin did not affect the choroid and RNFL in the comparison between the patient and control group. But in the multiple regression analysis performed in the pregabalin group, the duration of drug use appears as an independent risk factor in RNFL examination.
The small sample size is one of the main limitations of our study. We had to complete our study with small study groups because the prevalence of FM was not common and the exclusion of patients with systemic diseases and the eye pathologies.
Another limitation of the study was the manual measurement of choroidal thickness. Therefore, in our study, evaluations were made and compared by two independent researchers to check the reliability.
As a result, prolonged use of pregabalin, whose mechanism of action is mixed, has no effect on the choroid, while it has a thinning effect for RNFL. For this reason, it is recommended not to be preferred in patients with RNFL damage such as diabetic retinopathy and glaucoma when choosing drugs in FM patients. Patients receiving pregabalin treatment should be regularly examined in the ophthalmology clinic.
Summary
What was known before
-
Before our study, there was no study about the effects of pregabalin on the choroid and RNFL
What this study adds
-
In our study, it was found that pregabalin did not affect the choroid and it was observed that it thinned the RNFL in chronic use. We think that pregabalin use should not be preferred in individuals with diseases affecting RNFL such as glaucoma.
References
Häuser W, Fitzcharles MA. Facts and myths pertaining to fibromyalgia. Dialogues Clin Neurosci. 2018;20:53–62.
Marques AP, Santo ASDE, Berssaneti AA, Matsutani LA, Yuan SLK. Prevalence of fibromyalgia: literature review update. Rev Bras Reumatol Engl Ed. 2017;57:356–63.
Arnold LM, Choy E, Clauw DJ, Oka H, Whalen E, Semel D, et al. An evidence-based review of pregabalin for the treatment of fibromyalgia. Curr Med Res Opin. 2018;34:1397–409.
Tsang SH, Sharma T. Drug-induced retinal toxicity. Adv Exp Med Biol. 2018;1085:227–32.
Tanyıldız B, Kandemir B, Mangan MS, Tangılntız A, Göktaş E, Şimşek Ş. Bilateral serous macular detachment after attempted suicide with pregabalin. Turk J Ophthalmol. 2018;48:254–7.
Nickla DL, Wallman J. The multifunctional choroid. Prog Retin Eye Res. 2010;29:144–68.
Yıldırım G, Şahlı E, Alp MN. Evaluation of the Effect of Proptosis on Choroidal Thickness in Graves’ Ophthalmopathy. Turk J Ophthalmol. 2020;50:221–7.
Kalenderoglu A, Orum MH, Karadag AS, Kustepe A, Celik M, Egilmez OB, et al. Increases in retinal nerve fiber layer thickness may represent the neuroprotective effect of cannabis: an optical coherence tomography study. J Addict Dis. 2020;38:280–90.
Huang J, Zhou L, Wang H, Luo J, Zeng L, Xiong K, et al. Distribution of thrombospondins and their neuronal receptor α2δ1 in the rat retina. Exp Eye Res. 2013;111:36–49.
Kavoussi R. Pregabalin: From molecule to medicine. Eur Neuropsychopharmacol. 2006;16:S128–33. Suppl 2
White AT, Light KC, Bateman L, Hughen RW, Vanhaitsma TA, Light AR. Effect of pregabalin on cardiovascular responses to exercise and postexercise pain and fatigue in fibromyalgia: a randomized, double-blind, crossover pilot study. Pain Res Treat. 2015;2015:136409.
Parveen S, Negi DS, Kumar R, Bagwan MC. Oral clonidine vs oral pregabalin premedication to attenuate pressor response to direct laryngoscopy in patients undergoing laparoscopic cholecystectomy: a randomized double blind study. J Clin Diagn Res. 2016;10:UC21–UC25.
Kur J, Newman EA, Chan-Ling T. Cellular and physiological mechanisms underlying blood flow regulation in the retina and choroid in health and disease. Prog Retin Eye Res. 2012;31:377–406.
Toledo CA, Reiner A, Patel RS, Vitale AW, Klein JM, Dalsania BJ, et al. Immunohistochemical localization of AMPA-type glutamate receptor subunits in the nucleus of the Edinger-Westphal in embryonic chick. Neurosci Lett. 2011;498:199–203.
Cuthbertson S, White J, Fitzgerald ME, Shih YF, Reiner A. Distribution within the choroid of cholinergic nerve fibers from the ciliary ganglion in pigeons. Vis Res. 1996;36:775–86.
de Hoz R, Ramírez AI, Salazar JJ, Rojas B, Ramírez JM, Triviño A. Substance P and calcitonin gene-related peptide intrinsic choroidal neurons in human choroidal whole-mounts. Histol Histopathol. 2008;23:1249–58.
Lee EJ, Kim SJ, Han JC, Eo DR, Lee MG, Ham DI, et al. Peripapillary retinal nerve fiber layer thicknesses did not change in long-term hydroxychloroquine users. Korean J Ophthalmol. 2018;32:459–69.
Jin KW, Lee JY, Rhiu S, Choi DG. Longitudinal evaluation of visual function and structure for detection of subclinical Ethambutol-induced optic neuropathy. PLoS One. 2019;14:e0215297.
Moseng L, Sæter M, Mørch-Johnsen GH, Hoff JM, Gajda A, Brodtkorb E, et al. Retinal nerve fiber layer attenuation: clinical indicator for vigabatrin toxicity. Acta Ophthalmol. 2011;89:452–8.
Ali SA, Zaitone SA, Dessouki AA, Ali AA. Pregabalin affords retinal neuroprotection in diabetic rats: Suppression of retinal glutamate, microglia cell expression and apoptotic cell death. Exp Eye Res. 2019;184:78–90.
Chintalapudi SR, Maria D, Di Wang X, Bailey JNC. NEIGHBORHOOD consortium; International Glaucoma Genetics consortium, et al. Systems genetics identifies a role for Cacna2d1 regulation in elevated intraocular pressure and glaucoma susceptibility. Nat Commun. 2017;8:1755.
Ibrahim MM, Maria DN, Mishra SR, Guragain D, Wang X, Jablonski MM. Once daily pregabalin eye drops for management of glaucoma. ACS Nano. 2019;13:13728–44.
Moriya S, Hasegawa M, Inamasu J, Kogame H, Hirose Y, Higashi R, et al. Neuroprotective effects of pregabalin in a rat model of intracisternal facial nerve avulsion. J Neurosurg Sci. 2017;61:495–503.
Taha SHN, Zaghloul HS, Ali AAER, Gaballah IF, Rashed LA, Aboulhoda BE. The neurotoxic effect of long-term use of high-dose Pregabalin and the role of alpha tocopherol in amelioration: implication of MAPK signaling with oxidative stress and apoptosis. Naunyn Schmiedebergs Arch Pharmacol. 2020;393:1635–48.
Elgazzar FM, Elseady WS, Hafez AS. Neurotoxic effects of pregabalin dependence on the brain frontal cortex in adult male albino rats. Neurotoxicology. 2021;83:146–55.
Kamel MA. Study on DNA damage and oxidative stress and some biochemical alterations of long term administration of alpha-2 delta (Α2-Δ) ligand pregabalin and the possibility of Zingiber officinale in ameliorating these effects in rats. World J Pharm Res. 2016;5:1528–45.
Ninomiya W, Mizobuchi K, Hayashi T, Okude S, Katagiri S, Kubo A, et al. Electroretinographic abnormalities associated with pregabalin: a case report. Doc Ophthalmol. 2020;140:279–87.
Secinti IE. Retinal teratogenicity of pregabalin in chick embryo model. Cutan Ocul Toxicol. 2020;39:304–10.
Ulusoy MO, Kal A, Işik-Ulusoy S, Kal Ö. Choroidal thickness in patients with fibromyalgia and correlation with disease severity. Indian J Ophthalmol. 2018;66:428–32.
Garcia-Martin E, Garcia-Campayo J, Puebla-Guedea M, Ascaso FJ, Roca M, Gutierrez-Ruiz F, et al. Fibromyalgia is correlated with retinal nerve fiber layer thinning. PLoS One. 2016;11:e0161574.
Author information
Authors and Affiliations
Contributions
GYB was responsible for the study design, data collection and analysis, writing of the. manuscript and creation of the figures. KRZ and KEB were responsible for parts of the data collection. EK and EBK were responsible for manuscript review. The final version was of the manuscript was approved by all authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Biçer, G.Y., Zor, K.R., Biçer, K.E. et al. Can the long term using of pregabalin in fibromyalgia affect the choroid and retinal nerve fiber layer?. Eye 36, 2318–2322 (2022). https://doi.org/10.1038/s41433-021-01864-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-021-01864-9
