
Abstract
Aims/hypothesis
Estimates of the global prevalence of type 2 diabetes vary between 6% and 9%. The prevalence of type 2 diabetes has been investigated in psychiatric populations but a critical appraisal of the existing evidence is lacking, and an overview is needed. This umbrella review summarises existing systematic reviews of observational studies investigating the prevalence of type 2 diabetes in people with a psychiatric disorder.
Methods
We searched PubMed, EMBASE, PsycINFO and the Cochrane Database of Systematic Reviews from inception to 17 January 2021 and screened reference lists of included systematic reviews. On the basis of prespecified criteria, we included systematic reviews investigating the prevalence of type 2 diabetes in adults (aged ≥18 years) with a psychiatric disorder. Titles and abstracts of 5155 identified records and full texts of 431 selected studies were screened by two independent reviewers, based on predefined eligibility criteria and an a priori developed extraction form, following the PRISMA and MOOSE guidelines. Risk of bias was assessed with the ROBIS instrument. Data extracted from primary studies were synthesised using random-effects meta-analyses.
Results
A total of 32 systematic reviews with 245 unique primary studies were identified and met inclusion criteria. Twelve had low risk of bias. They reported type 2 diabetes prevalence estimates ranging from 5% to 22% depending on the specific psychiatric disorder. We meta-analysed data for ten categories of psychiatric disorders and found the following prevalence estimates of type 2 diabetes: in people with a sleep disorder: 40%; binge eating disorder: 21%; substance use disorder: 16%; anxiety disorder: 14%; bipolar disorder: 11%; psychosis: 11%; schizophrenia: 10%; a mixed group of psychiatric disorders: 10%; depression: 9%; and in people with an intellectual disability 8%. All meta-analyses revealed high levels of heterogeneity.
Conclusions/interpretation
Type 2 diabetes is a common comorbidity in people with a psychiatric disorder. Future research should investigate whether routine screening for type 2 diabetes and subsequent prevention initiatives for these people are warranted.
PROSPERO registration no. CRD42020159870.
Similar content being viewed by others



Introduction
Psychiatric disorders are common [1], can substantially impair quality of life [2], and are associated with elevated mortality rates [3, 4]. Excess mortality in individuals with a psychiatric disorder can be attributed not only to more frequent suicides and accidents but also to the high prevalence of comorbid somatic disorders in this population [5,6,7,8]. The prevalence of type 2 diabetes mellitus, for example, has been reported to be higher in people with bipolar disorder [9], schizophrenia [10] or major depression [11], compared with the general population. The global prevalence of type 2 diabetes has increased from 1990 onwards, current estimates ranging between 6.3% and 9.3%, and is expected to increase further within the next 20 years [12, 13]. During recent decades, systematic reviews have investigated the prevalence of type 2 diabetes in people with different psychiatric disorders. However, no systematic overview and critical appraisal of this literature is currently available.
To address this limitation, this umbrella review sought to summarise and critically assess the existing evidence on the prevalence of type 2 diabetes in people with a psychiatric disorder. We focused on systematic reviews of observational studies to generate a narrative synthesis of the prevalence estimates. Our review included a risk of bias assessment and meta-analyses of prevalence estimates from the primary studies included in the systematic reviews.
Methods
Protocol, registration and study design
We registered the protocol for this umbrella review at PROSPERO (registration no. CRD42020159870) and described it in an a priori published protocol [14]. We followed the Preferred Reporting Items for Systematics Reviews and Meta-Analyses (PRISMA) [15] and the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines [16] (ESM Tables 1 and 2). The umbrella review covers systematic reviews describing the prevalence of type 2 diabetes in people with a psychiatric disorder.
Search strategy and eligibility criteria
We searched four electronic databases (PubMed, EMBASE, PsycINFO and Cochrane Database of Systematic Reviews) from their inception to 17 January 2021. We used a structured search strategy with searches in four blocks: (1) block I, psychiatric disorders; (2) block II, diabetes; (3) block III, prevalence; and (4) block IV, systematic reviews. Search words and Medical Subject Headings (MeSH) terms within each block of the search were combined with an ‘OR’. In the final search, the blocks (I–IV) were combined with an ‘AND’. We included only systematic reviews in English, Dutch, German or Scandinavian language, with no limitations in publication date. The complete block search is reported in ESM Table 3.
More specifically, we included systematic reviews of observational studies, investigating the prevalence of type 2 diabetes in people with a psychiatric disorder. We used a definition of psychiatric disorders as psychiatric diagnoses mentioned in the ICD (http://apps.who.int/classifications/icd10/browse/2016/en) or Diagnostic and Statistical Manual of Mental Disorders (DSM) classification systems, or elevated levels of clusters of psychiatric symptoms (DSM III or DSM IV, axis I or axis II; DSM5 section II; ICD-10, F00-F99) [17,18,19,20]. We did not include reviews focusing on either a single psychiatric symptom or distress not described as a condition in the ICD or DSM classification systems (e.g. work-related stress and sleep duration). We included systematic reviews where the psychiatric disorders were assessed by diagnosis, diagnostic interviews, hospital records, prescriptions of psychotropic medication, or self-reported, and where type 2 diabetes was assessed by diagnosis, medical records, prescription of glucose-lowering medication, or self-reports. Only systematic reviews focusing on adult samples (age ≥18 years) were included. If no information was available regarding type of diabetes, we expected that most of the individuals had type 2 diabetes and included the study. Studies with a design other than a systematic review were excluded. Similarly, reviews without an explicit literature search strategy were regarded as unsystematic and were thus excluded.
We removed duplicates in merged searches from different databases with the reference managing package EndNote X8 (Clarivate Analytics, USA). Two independent reviewers (NL and SHS) selected studies to be read in full text by screening titles and abstracts using the software package Covidence (Melbourne, Australia), and subsequently selected studies for final inclusion based on the full text of these studies, based on the predefined eligibility criteria. If at least one of the reviewers regarded a record as potentially eligible during the title/abstract screening, the record was included and evaluated at the full-text level. Any disagreements at the full-text level were resolved after consulting a third author (FR). Finally, the reference lists of the included systematic reviews were manually screened for other potentially eligible systematic reviews.
Data extraction
Two independent reviewers (NL and SHS) extracted the following information from the included systematic reviews, using an extraction form we developed before extraction of the information: name of first author; year of publication; country where the study was conducted; type of study (systematic review with or without meta-analysis); type of psychiatric disorder(s); assessment of psychiatric disorder(s); assessment of type 2 diabetes; number of primary studies of the prevalence of type 2 diabetes; total number of study participants; and primary findings including information on the prevalence of type 2 diabetes, ORs and RRs, when possible. The first author (NL) extracted the following information from all primary studies included in the systematic reviews: name of first author; year of publication; total number of study participants; number of study participants with type 2 diabetes; and/or prevalence estimates. We divided the included systematic reviews into categories of psychiatric disorders and conducted a narrative data synthesis for each of the identified categories of psychiatric disorders.
Statistical analysis
If more than one systematic review described the prevalence of type 2 diabetes for each of the identified categories of psychiatric disorders, we conducted separate meta-analyses to summarise the results of a large number of prevalence estimates quantitatively. This was a deviation from the original PROSPERO protocol, although the amendment was described in our published protocol [14]. We conducted meta-analyses based on data extracted from the primary studies that were included in the systematic reviews. We defined the numerator as number of people with a psychiatric disorder and type 2 diabetes, and the denominator as total number of people with a psychiatric disorder in the primary study. We included each primary study only once in the meta-analysis. If several primary studies were based on the same sample, we included the study with the largest sample size. If data regarding the numerator and denominator were not available in the primary study, we extracted data from the original systematic review, when possible, as the authors of the systematic reviews in some cases had contacted the author of the primary study to obtain the relevant information. Where no data was available, we excluded the primary study from the meta-analyses.
We used a random-effects model for all meta-analyses. In order to stabilise the variance, we used double arcsine transformations and the inverse variance method [21]. We calculated the I2 metrics to evaluate between-study heterogeneity [22, 23]. In our published protocol [14], we planned to use Egger’s test to examine publication bias [24]. However, concerns have been raised about the sensitivity of Egger’s test to detect asymmetry when the number of included studies is small [25]. Therefore, we decided to use two more recent methods, the Doi plot and the Luis Furuya-Kanamori (LFK) index, to identify publication bias. In the LFK index a value beyond ±1 is deemed consistent with publication bias and this index has been shown to be more sensitive than Egger’s test [25]. All meta-analyses were conducted in MetaXL version 5.3, a software package for meta-analysis in Microsoft Excel [21, 26].
Risk of bias assessment
Two independent reviewers (NL and either SHS or LK) assessed the risk of bias for each of the included systematic reviews, using the Risk of Bias in Systematic Reviews (ROBIS) tool [27]. A third author (LK or SHS) resolved disagreements. We assessed the following four types of risk of bias: (1) study eligibility criteria; (2) identification and selection of studies; (3) data collection and study appraisal; and (4) synthesis and findings. Based on how we assessed potential risk of bias within these four types, we assessed an overall risk of bias in the systematic review (high, low or unclear risk of bias).
Results
Study selection and characteristics
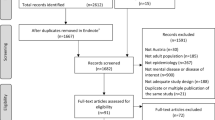
In total, we identified 32 systematic reviews including a total of 245 unique primary studies focusing on prevalence of type 2 diabetes in psychiatric disorders from 431 full-text screenings and 5155 records found in the dataset searches (Fig. 1). The included systematic reviews were focused on 11 categories of psychiatric disorders: (1) schizophrenia (n = 7) [10, 28,29,30,31,32,33]; (2) bipolar disorder (n = 4) [9, 31, 34, 35]; (3) depression (n = 3) [11, 31, 36]; (4) substance use disorder (n = 3) [31, 37, 38]; (5) anxiety disorder (n = 2) [31, 39]; (6) eating disorder (n = 2) [40, 41]; (7) intellectual disability (n = 2) [42, 43]; (8) psychosis (n = 2) [44, 45]; (9) sleep disorder (n = 2) [46, 47]; (10) dementia (n = 1) [48]; and (11) a ‘mixed’ group that comprised different types of psychiatric disorders (n = 9) [31, 49,50,51,52,53,54,55,56].

Study flowchart
We present the characteristics of the 32 systematic reviews in Table 1. Nineteen (59%) of the 32 systematic reviews originated from Europe, six (19%) from the USA, four (13%) from Australia and one (3%) from each of Chile, China and Ethiopia. Different methods were used to identify psychiatric disorders and type 2 diabetes, including diagnostic criteria, prescription data, screening, admission status, medical records, diagnostic tests, surveys, questionnaires, interviews and self-reports. In most of the systematic reviews (91%, 29/32), multiple types of assessments were used. A considerable proportion (41%, 13/32) did not report the type of assessment for psychiatric disorders or type 2 diabetes. Several systematic reviews were based on an overlapping set of primary studies. We report an overview of the 245 unique primary studies of the prevalence of type 2 diabetes in ESM Table 4.
Risk of bias assessment
We report an overview of the risk of bias assessment in Table 2 and ESM Fig. 1. Twenty of the included systematic reviews had a high risk of bias [28,29,30,31,32,33,34,35,36, 41, 42, 45, 47,48,49, 51, 52, 54,55,56] while 12 had a low risk of bias [9,10,11, 37,38,39,40, 43, 44, 46, 50, 53]. We found high concerns regarding the identification and selection of studies in 19 reviews (59%) and concerns regarding the data collection and study appraisal in 18 reviews (56%).
Narrative synthesis
An overview of prevalence estimates for each category of psychiatric disorder is shown in Table 3. In the 32 systematic reviews, prevalence estimates for type 2 diabetes in people with identified psychiatric disorders ranged between 1.3% and 66.0%. When only including systematic reviews with low risk of bias (n = 12), the prevalence estimates of type 2 diabetes ranged from 5.1% to 22.3%. In the systematic reviews with low risk of bias, the highest prevalence estimates of type 2 diabetes was reported in people with a sleep disorder (22.3%) [46], psychosis (18.9%) [44] and a substance use disorder (11.9–15.6%) [37, 38]. Forty-four per cent (14/32) of the included systematic reviews made comparisons with control groups and reported increased risk of type 2 diabetes in people with psychiatric disorders. In one of the included systematic reviews investigating people with an intellectual disability, three primary studies reported less prevalence of diabetes in people with an intellectual disability compared with the general population [42].
Meta-analyses of the prevalence of type 2 diabetes
For ten of the 11 categories of psychiatric disorders, more than one systematic review reported the prevalence of people with type 2 diabetes. We therefore conducted new meta-analyses of type 2 diabetes prevalence estimates for each of these categories of psychiatric disorders. These ten meta-analyses included between six and 153 unique primary studies depending on the psychiatric disorder, and an overview of the estimated prevalence estimates for each of the categories is presented in Table 4. According to our meta-analyses, people with a sleep disorder have the highest prevalence of type 2 diabetes (39.7% [95% CI 34.9, 44.7%]), followed by those with a binge eating disorder (20.7% [95% CI 7.6, 37.4]), a substance use disorder (15.6% [95% CI 10.3, 21.7]), an anxiety disorder (13.7% [95% CI 7.7, 20.9]), bipolar disorder (11.4% [95% CI 7.8, 15.6]) and psychosis (11.1% [95% CI 7.3, 15.5]). We found the lowest prevalence of type 2 diabetes in people with an intellectual disability (8.1% [95% CI 6.5, 9.8]). We present forest plots for all meta-analyses in ESM Fig. 2.
In all meta-analyses, a high level of between-study heterogeneity was detected (I2 0.89–0.99). We found substantial publication bias in the four meta-analyses focusing on schizophrenia, substance use disorder, binge eating disorder and mixed group of psychiatric disorders. We found only minor publication bias in the meta-analysis of type 2 diabetes prevalence in people with psychosis. We present Doi plots for all meta-analyses in ESM Fig. 3.
Discussion
In this umbrella review, we systematically summarised and critically assessed the existing evidence on the prevalence of type 2 diabetes in people with a psychiatric disorder.
We meta-analysed data from primary studies for ten categories of psychiatric disorders revealing prevalence estimates between 8% and 40%. Our meta-analyses were based on primary studies from several systematic reviews and therefore were built on more data than previous meta-analyses. Overall, we found that most of the meta-analyses revealed type 2 diabetes prevalence estimates that were comparable with existing meta-analyses within each of the categories of psychiatric disorders [9,10,11, 38,39,40, 44, 46, 50, 53]. However, meta-analysed data revealed notably high prevalence estimates for sleep disorder (40%) and binge eating disorder (20%). Sleep disorder, as defined in DSM5, constitute a subgroup of psychiatric disorders [19] and have high comorbidity with several other somatic diseases [57, 58]. In our umbrella review, most of the primary studies were conducted among people with additional somatic diseases such as chronic kidney disease. It is likely that this physical comorbidity contributes to the high type 2 diabetes prevalence estimates in people with a sleep disorder. A previous review suggested the association between sleep disorders and type 2 diabetes is bidirectional, with sleep disorders being a risk factor for type 2 diabetes and type 2 diabetes (especially when combined with poor metabolic control) being a risk factor for sleep disorders [59]. For people with a binge eating disorder, the type 2 diabetes prevalence estimates were based on data from four primary studies with limited sample sizes. The results should be interpretated with caution, due to large CIs. Additionally, there might be an effect of publication year, with more recent publications reporting higher prevalence of type 2 diabetes in people with a binge eating disorder (see ESM Fig. 2).
In 44% of the included systematic reviews, comparisons with control groups were made, revealing an increased prevalence of type 2 diabetes in people with a psychiatric disorder. This increased prevalence of type 2 diabetes was detected for most of the investigated psychiatric disorders, suggesting a shared vulnerability in people with psychiatric disorders to the development of type 2 diabetes. In line with these findings, our meta-analysed type 2 diabetes prevalence estimates typically exceeded those for global prevalence estimates of type 2 diabetes [12, 13]. However, better understanding of these differences and explaining factors are still needed. The global prevalence estimates of 6.3% to 9.3% for type 2 diabetes is as reported in 2017 and 2019, respectively [12, 13], whereas the primary studies included in the meta-analyses were conducted between 1980 and 2020. The comparison of the global prevalence estimates with the findings from our meta-analyses suggest that people grouped across all the investigated psychiatric disorders more often have type 2 diabetes. However, more refined comparisons should be made between prevalence estimates in the future to better account for differences in populations groups, study settings and the broad range of years as well as methods used to ascertain type 2 diabetes.
In the general population, the prevalence of type 2 diabetes has increased considerably over the past decades [13, 60, 61] due to an increase in the population incidence of obesity and type 2 diabetes, a decrease in age-standardised mortality and a growing proportion of the ageing population [62]. However, with the exception of people with a binge eating disorder, the forest plots (ESM Fig. 2) show that when the primary studies are ranked according to publication year, there is no indication of increase in prevalence estimates of type 2 diabetes in people with a psychiatric disorder with publication year of the study over the past two or three decades. This might be explained by issues such as changes in prescription patterns of psychotropic drugs [63] and the high likelihood of undiagnosed type 2 diabetes in people with a psychiatric disorder [64]. These issues warrant further investigation.
Overall, this umbrella review highlights the importance of focusing on prevalent type 2 diabetes across different psychiatric disorders, as we see a general pattern of elevated type 2 diabetes prevalence rates in people with a psychiatric disorder. Much of previous research has focused on schizophrenia and depression [10, 65,66,67], but our findings suggest that the prevalence of type 2 diabetes is also high in several other psychiatric disorders, emphasising the need for future studies that cover the full range of psychiatric disorders. Future collaborations should follow the example of the initiative of the European Depression in Diabetes (EDID) Research Consortium [68], combining researchers from different fields and countries to collaborate with a focus on a psychiatric disorder and diabetes.
Strengths and limitations
To the best of our knowledge, this is the most comprehensive summary on type 2 diabetes in psychiatric disorders to date providing an overview across different psychiatric disorders in one and the same paper. We have summarised all existing systematic reviews in the field and included all primary studies to estimate the type 2 diabetes prevalence for each psychiatric disorder.
There are also several limitations that should be acknowledged. First, our umbrella review included studies published during an extended period of several decades, during which time the clinical context has changed considerably. Changes in treatment guidelines [69] and lifestyle factors such as physical activity [70], dietary habits [71] and smoking behaviours [72] will presumably have had an impact on prevalence estimates of type 2 diabetes in people with a psychiatric disorder. We have not explored effects of these developments in this umbrella review. Second, we have not included the most recent observational studies, which are not included in a systematic review. However, primary studies up to 2020 have been included in the umbrella review, and we therefore estimate that this gap is modest. Third, the prevalence of type 2 diabetes was not available for some common psychiatric disorders such as attention deficit hyperactivity disorder and autism. Fourth, most of the included systematic reviews had high risk of bias regarding the identification and selection of studies, and there were also concerns regarding data collection and study appraisal. Most of the systematic reviews rated as having high risk of bias were rated as such because no efforts were taken to minimise error during the conduction of the study (e.g. no description of two independent reviewers conducting the procedures). Last, we detected publication bias in several of the identified categories of psychiatric disorders. All conducted meta-analyses yielded wide CIs, and we found a high level of heterogeneity. This might be explained by different types of study populations due to different purposes of the included systematic reviews and primary studies. Some systematic reviews had no restrictions on the study population, whereas other reviews had a narrower focus on elderly populations or hospital inpatients. Furthermore, different assessment methods of psychiatric disorders and type 2 diabetes were used. More homogenous prevalence estimates could be expected if all primary studies used the gold standards for diagnosis of type 2 diabetes [73].
Conclusions
For more than a decade, the importance of screening and adequate treatment of type 2 diabetes in people with psychiatric disorders has been highlighted [74]. By providing the most comprehensive review on this issue to date, this umbrella review confirms that type 2 diabetes is a common comorbidity in people with a psychiatric disorder, particularly a sleep disorder, a binge eating disorder, a substance use disorder or an anxiety disorder. Our review identified a need for future research to identify contributors to this comorbidity. Future research must determine whether underdiagnosis of type 2 diabetes in people with psychiatric disorders means that the present figures are lower-bound estimates. Reliable information about prevalence and a better understanding of biological and behavioural factors driving increased prevalence of type 2 diabetes in people with psychiatric disorders will be crucial to developing cost-effective strategies for the management of type 2 diabetes in people with psychiatric disorders.
Data availability
Application for datasets generated during and/or analysed during the current study may be considered by the corresponding author on reasonable request.
Abbreviations
- DSM:
-
Diagnostic and Statistical Manual of Mental Disorders
- LFK:
-
Luis Furuya-Kanamori
- ROBIS:
-
Risk of Bias in Systematic Reviews
References
Steel Z, Marnane C, Iranpour C et al (2014) The global prevalence of common mental disorders: a systematic review and meta-analysis 1980-2013. Int J Epidemiol 43(2):476–493. https://doi.org/10.1093/ije/dyu038
Connell J, Brazier J, O’Cathain A, Lloyd-Jones M, Paisley S (2012) Quality of life of people with mental health problems: a synthesis of qualitative research. Health Qual Life Outcomes 10(1):138. https://doi.org/10.1186/1477-7525-10-138
Walker ER, McGee RE, Druss BG (2015) Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiatry 72(4):334–341. https://doi.org/10.1001/jamapsychiatry.2014.2502
Chesney E, Goodwin GM, Fazel S (2014) Risks of all-cause and suicide mortality in mental disorders: a meta-review. World Psychiatry 13(2):153–160. https://doi.org/10.1002/wps.20128
Brown S, Kim M, Mitchell C, Inskip H (2010) Twenty-five year mortality of a community cohort with schizophrenia. Br J Psychiatry 196(2):116–121. https://doi.org/10.1192/bjp.bp.109.067512
McGrath J, Saha S, Chant D, Welham J (2008) Schizophrenia: a concise overview of incidence, prevalence, and mortality. Epidemiol Rev 30:67–76. https://doi.org/10.1093/epirev/mxn001
Saha S, Chant D, McGrath J (2007) A systematic review of mortality in schizophrenia: is the differential mortality gap worsening over time? Arch Gen Psychiatry 64(10):1123–1131. https://doi.org/10.1001/archpsyc.64.10.1123
Mensah GA, Collins PY (2015) Understanding mental health for the prevention and control of cardiovascular diseases. Glob Heart 10(3):221–224. https://doi.org/10.1016/j.gheart.2015.08.003
Vancampfort D, Mitchell AJ, De Hert M et al (2015) Prevalence and predictors of type 2 diabetes mellitus in people with bipolar disorder: a systematic review and meta-analysis. J Clin Psychiatry 76(11):1490–1499. https://doi.org/10.4088/JCP.14r09635
Stubbs B, Vancampfort D, De Hert M, Mitchell AJ (2015) The prevalence and predictors of type two diabetes mellitus in people with schizophrenia: a systematic review and comparative meta-analysis. Acta Psychiatr Scand 132(2):144–157. https://doi.org/10.1111/acps.12439
Vancampfort D, Mitchell AJ, De Hert M et al (2015) Type 2 diabetes in patients with major depressive disorder: a meta-analysis of prevalence estimates and predictors. Depress Anxiety 32(10):763–773. https://doi.org/10.1002/da.22387
Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al KJ (2020) Global burden of disease and forecasted trends. J Epidemiol Glob Health 10(1):107–111. https://doi.org/10.2991/jegh.k.191028.001
Saeedi P, Petersohn I, Salpea P et al (2019) Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the international diabetes federation diabetes atlas, 9(th) edition. Diabetes Res Clin Pract 157:107843. https://doi.org/10.1016/j.diabres.2019.107843
Lindekilde N, Scheuer S, Rutters F et al (2020) The prevalence of type 2 diabetes in people with psychiatric disorders: an umbrella review protocol. Sys Rev 9(1):101–101. https://doi.org/10.1186/s13643-020-01341-6
Moher D, Liberati A, Tetzlaff J, Altman DG, the PG, Group P (2009) Preferred reporting items for systematic reviews and Meta-analyses: the PRISMA statement. PLoS Med 6(7):e1000097. https://doi.org/10.1093/ptj/89.9.873
Stroup DF, Berlin JA, Morton SC et al (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. JAMA 283(15):2008–2012. https://doi.org/10.1001/jama.283.15.2008
American Psychiatric Association (2000) Diagnostic and statistical manual of mental disorders: DSM-IV-TR. American Psychiatric Association, Washington, DC
American Psychiatric Association (1980) Diagnostic and statistical manual of mental disorders: DSM-III. American Psychiatric Association, Washington, DC
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Association, Arlington, VA
World Health Organization (2009) The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. World Health Organization, Geneva. https://doi.org/10.1067/j.cpsurg.2009.04.002
Barendregt JJ, Doi SA, Lee YY, Norman RE, Vos T (2013) Meta-analysis of prevalence. J Epidemiol Community Health 67(11):974–978. https://doi.org/10.1136/jech-2013-203104
Cochran WG (1954) The combination of estimates from different experiments. Biometrics 10:101–129. https://doi.org/10.2307/3001666
Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21(11):1539–1558. https://doi.org/10.1002/sim.1186
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634. https://doi.org/10.1136/bmj.315.7109.629
Furuya-Kanamori L, Barendregt JJ, Doi SAR (2018) A new improved graphical and quantitative method for detecting bias in meta-analysis. Int J Evid Based Healthc 16(4):195–203. https://doi.org/10.1097/xeb.0000000000000141
EpiGear International Pty Ltd (2016) MetaXL: version 5.3. Available from https://www.epigear.com/indexfiles/metaxl.html. Accessed 1 Feb 2021
Whiting P, Savovic J, Higgins JP et al (2016) ROBIS: a new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol 69:225–234. https://doi.org/10.1016/j.jclinepi.2015.06.005
Mitchell AJ, Vancampfort D, De Herdt A, Yu W, De Hert M (2013) Is the prevalence of metabolic syndrome and metabolic abnormalities increased in early schizophrenia? A comparative Meta-analysis of first episode, untreated and treated patients. Schizophr Bull 39(2):295–305. https://doi.org/10.1093/schbul/sbs082
Mitchell AJ, Vancampfort D, Sweers K, van Winkel R, Yu W, De Hert M (2013) Prevalence of metabolic syndrome and metabolic abnormalities in schizophrenia and related disorders—a systematic review and Meta-analysis. Schizophr Bull 39(2):306–318. https://doi.org/10.1093/schbul/sbr148
Oud MJT, Meyboom-de Jong B (2009) Somatic diseases in patients with schizophrenia in general practice: their prevalence and health care. BMC Fam Pract 10(1):32–32. https://doi.org/10.1186/1471-2296-10-32
van den Brink AMA, Gerritsen DL, Voshaar RCO, Koopmans RTCM (2013) Residents with mental–physical multimorbidity living in long-term care facilities: prevalence and characteristics. A systematic review. Int Psychogeriatr 25(4):531–548. https://doi.org/10.1017/S1041610212002025
Ayano G (2019) Co-occurring medical and substance use disorders in patients with schizophrenia: a systematic review. Int J Ment Health 48(1):62–76. https://doi.org/10.1080/00207411.2019.1581047
Ma T, Mackinnon T, Dean K (2020) The prevalence of cardiometabolic disease in people with psychotic disorders in secure settings – a systematic review. J Forensic Psychiatry Psychol 1–27. https://doi.org/10.1080/14789949.2020.1859588
Charles EF, Lambert CG, Kerner B (2016) Bipolar disorder and diabetes mellitus: evidence for disease-modifying effects and treatment implications. Int J Bipolar Disord 4(1):1–11. https://doi.org/10.1186/s40345-016-0054-4
Lala SV, Sajatovic M (2012) Medical and psychiatric comorbidities among elderly individuals with bipolar disorder: a literature review. J Geriatr Psychiatry Neurol 25(1):20–25. https://doi.org/10.1177/0891988712436683
Ross GP, Falhammar H, Chen R, Barraclough H, Kleivenes O, Gallen I (2016) Relationship between depression and diabetes in pregnancy: a systematic review. World J Diabetes 7(19):554–571. https://doi.org/10.4239/wjd.v7.i19.554
Dam MJ, Meijel B, Postma A, Oudman E (2020) Health problems and care needs in patients with Korsakoff’s syndrome: a systematic review. J Psychiatr Ment Health Nurs 27(4):460–481. https://doi.org/10.1111/jpm.12587
Vancampfort D, Mugisha J, Hallgren M et al (2016) The prevalence of diabetes mellitus type 2 in people with alcohol use disorders: a systematic review and large scale meta-analysis. Psychiatry Res 246:394–400. https://doi.org/10.1016/j.psychres.2016.10.010
Vancampfort D, Rosenbaum S, Ward PB et al (2016) Type 2 diabetes among people with posttraumatic stress disorder: systematic review and Meta-analysis. Psychosom Med 78(4):465–473. https://doi.org/10.1097/psy.0000000000000297
Nieto-Martinez R, Gonzalez-Rivas JP, Medina-Inojosa JR, Florez H (2017) Are eating disorders risk factors for type 2 diabetes? A systematic review and Meta-analysis. Curr Diab Rep 17(12):138. https://doi.org/10.1007/s11892-017-0949-1
Olguin P, Fuentes M, Gabler G, Guerdjikova AI, Keck PE Jr, McElroy SL (2017) Medical comorbidity of binge eating disorder. Eat Weight Disord 22(1):13–26. https://doi.org/10.1007/s40519-016-0313-5
MacRae S, Brown M, Karatzias T et al (2015) Diabetes in people with intellectual disabilities: a systematic review of the literature. Res Dev Disabil 47:352–374. https://doi.org/10.1016/j.ridd.2015.10.003
McVilly K, McGillivray J, Curtis A, Lehmann J, Morrish L, Speight J (2014) Diabetes in people with an intellectual disability: a systematic review of prevalence, incidence and impact. Diabet Med 31(8):897–904. https://doi.org/10.1111/dme.12494
Chung J, Miller BJ (2020) Meta-analysis of comorbid diabetes and family history of diabetes in non-affective psychosis. Schizophr Res 216:41–47. https://doi.org/10.1016/j.schres.2019.10.062
Foley DL, Morley KI (2011) Systematic review of early Cardiometabolic outcomes of the first treated episode of psychosis. Arch Gen Psychiatry 68(6):609–616. https://doi.org/10.1001/archgenpsychiatry.2011.2
Guo J, Sun Y, Xue L-J et al (2016) Effect of CPAP therapy on cardiovascular events and mortality in patients with obstructive sleep apnea: a meta-analysis. Sleep Breath 20(3):965–974. https://doi.org/10.1007/s11325-016-1319-y
Puthenpura MM, Hansrivijit P, Ghahramani N, Thongprayoon C, Cheungpasitporn W (2020) Chronic kidney disease and concomitant sleep apnea are associated with increased overall mortality: a meta-analysis. Int Urol Nephrol 52(12):2337–2343. https://doi.org/10.1007/s11255-020-02583-y
Smith T, Maidment I, Hebding J et al (2014) Systematic review investigating the reporting of comorbidities and medication in randomized controlled trials of people with dementia. Age Ageing 43(6):868–872. https://doi.org/10.1093/ageing/afu100
Janssen EM, McGinty EE, Azrin ST, Juliano-Bult D, Daumit GL (2015) Review of the evidence: prevalence of medical conditions in the United States population with serious mental illness. Gen Hosp Psychiatry 37(3):199–222. https://doi.org/10.1016/j.genhosppsych.2015.03.004
Onyeka IN, Collier Høegh M, Eien EMN, Nwaru BI, Melle I (2019) Comorbidity of physical disorders among patients with severe mental illness with and without substance use disorders: a systematic review and Meta-analysis. J Dual Diagnosis 15(3):192–206. https://doi.org/10.1080/15504263.2019.1619007
Osborn DPJ, Wright CA, Levy G, King MB, Deo R, Nazareth I (2008) Relative risk of diabetes, dyslipidaemia, hypertension and the metabolic syndrome in people with severe mental illnesses: systematic review and metaanalysis. BMC Psychiatry 8(1):84–84. https://doi.org/10.1186/1471-244x-8-84
Rigal A, Colle R, El Asmar K et al (2018) Framingham coronary score in individuals with symptoms or diagnoses of mental disorders: a review and meta-analysis. Psychiatry Res 263:41–47. https://doi.org/10.1016/j.psychres.2018.02.035
Roberts E, Jones L, Blackman A et al (2017) The prevalence of diabetes mellitus and abnormal glucose metabolism in the inpatient psychiatric setting: a systematic review and meta-analysis. Gen Hosp Psychiatry 45:76–84. https://doi.org/10.1016/j.genhosppsych.2017.01.003
Vancampfort D, Correll CU, Galling B et al (2016) Diabetes mellitus in people with schizophrenia, bipolar disorder and major depressive disorder: a systematic review and large scale meta-analysis. World Psychiatry 15(2):166–174. https://doi.org/10.1002/wps.20309
Barnard K, Peveler RC, Holt RI (2013) Antidepressant medication as a risk factor for type 2 diabetes and impaired glucose regulation: systematic review. Diabetes Care 36(10):3337–3345. https://doi.org/10.2337/dc13-0560
Young SL, Taylor M, Lawrie SM (2014) “First do no harm.” a systematic review of the prevalence and management of antipsychotic adverse effects. J Psychopharmacol 29(4):353–362. https://doi.org/10.1177/0269881114562090
Bonsignore MR, Baiamonte P, Mazzuca E, Castrogiovanni A, Marrone O (2019) Obstructive sleep apnea and comorbidities: a dangerous liaison. Multidiscip Respir Med 14(1):8. https://doi.org/10.1186/s40248-019-0172-9
Jehan S, Zizi F, Pandi-Perumal SR et al (2017) Obstructive sleep apnea and obesity: implications for public health. Sleep Med Disord 1(4):00019
Barone MT, Menna-Barreto L (2011) Diabetes and sleep: a complex cause-and-effect relationship. Diabetes Res Clin Pract 91(2):129–137. https://doi.org/10.1016/j.diabres.2010.07.011
Wild S, Roglic G, Green A, Sicree R, King H (2004) Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 27(5):1047–1053. https://doi.org/10.2337/diacare.27.5.1047
Whiting DR, Guariguata L, Weil C, Shaw J (2011) IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract 94(3):311–321. https://doi.org/10.1016/j.diabres.2011.10.029
Carstensen B, Rønn PF, Jørgensen ME (2020) Components of diabetes prevalence in Denmark 1996–2016 and future trends until 2030. BMJ Open Diabetes Res Care 8(1):e001064. https://doi.org/10.1136/bmjdrc-2019-001064
Braslow JT, Marder SR (2019) History of psychopharmacology. Annu Rev Clin Psychol 15:25–50. https://doi.org/10.1146/annurev-clinpsy-050718-095514
Holt RI, Mitchell AJ (2015) Diabetes mellitus and severe mental illness: mechanisms and clinical implications. Nat Rev Endocrinol 11(2):79–89. https://doi.org/10.1038/nrendo.2014.203
Tabák AG, Akbaraly TN, Batty GD, Kivimäki M (2014) Depression and type 2 diabetes: a causal association? Lancet Diabetes Endocrinol 2(3):236–245. https://doi.org/10.1016/S2213-8587(13)70139-6
Moulton CD, Pickup JC, Ismail K (2015) The link between depression and diabetes: the search for shared mechanisms. Lancet Diabetes Endocrinol 3(6):461–471. https://doi.org/10.1016/S2213-8587(15)00134-5
Pillinger T, Beck K, Gobjila C, Donocik JG, Jauhar S, Howes OD (2017) Impaired glucose homeostasis in first-episode schizophrenia: a systematic review and Meta-analysis. JAMA Psychiatry 74(3):261–269. https://doi.org/10.1001/jamapsychiatry.2016.3803
Nouwen A, Winkley K, Twisk J et al (2010) Type 2 diabetes mellitus as a risk factor for the onset of depression: a systematic review and meta-analysis. Diabetologia 53(12):2480–2486. https://doi.org/10.1007/s00125-010-1874-x
Blaslov K, Naranđa FS, Kruljac I, Renar IP (2018) Treatment approach to type 2 diabetes: past, present and future. World J Diabetes 9(12):209–219. https://doi.org/10.4239/wjd.v9.i12.209
Borodulin K, Laatikainen T, Juolevi A, Jousilahti P (2007) Thirty-year trends of physical activity in relation to age, calendar time and birth cohort in Finnish adults. Eur J Pub Health 18(3):339–344. https://doi.org/10.1093/eurpub/ckm092
Bentley J (2017) U.S. Trends in Food Availability and a Dietary Assessment of Loss-Adjusted Food Availability, 1970–2014. In: EIB-166, U.S. Department of Agriculture, Washington, D.C., Economic Research Service
Cummings KM, Proctor RN (2014) The changing public image of smoking in the United States: 1964-2014. Cancer Epidemiol Biomark Prev 23(1):32–36. https://doi.org/10.1158/1055-9965.EPI-13-0798
American Diabetes A (2018) 2. Classification and diagnosis of diabetes: standards of medical Care in Diabetes—2019. Diabetes Care 42(Supplement 1):S13–S28. https://doi.org/10.2337/dc19-s002
De Hert M, Dekker JM, Wood D, Kahl KG, Holt RI, Moller HJ (2009) Cardiovascular disease and diabetes in people with severe mental illness position statement from the European psychiatric association (EPA), supported by the European Association for the Study of diabetes (EASD) and the European Society of Cardiology (ESC). European Psychiatry 24(6):412–424. https://doi.org/10.1016/j.eurpsy.2009.01.005
Authors’ relationships and activities
GSA own shares in Novo Nordisk A/S. FR is an associate editor at Diabetologia. All other authors declare that there are no relationships or activities that might bias, or be perceived to bias, their work.
Funding
This work is supported by an unrestricted grant for research (PhD Fellowship) from the Department of Psychology, Faculty of Health Sciences, University of Southern Denmark to FP. MK was supported by NordForsk (the Nordic Research Programme on Health and Welfare), the UK Medical Research Council (K013351 and R024227), the National Institute on Aging (National Institutes of Health, R01AG056477 and R01AG062553), the Academy of Finland (329202) and Helsinki Institute of Life Science during the conduct of this study. The study sponsor/funder was not involved in the design of the study, the collection, analysis and interpretation of data, writing the report, and did not impose any restrictions regarding publication of the report.
Author information
Authors and Affiliations
Contributions
All authors have contributed in a meaningful way. NL and FP had the original idea for the study and NL completed the searches. NL, SS and LK conducted the screening for relevant papers, extracted data and assessed risk of bias. NL conducted the analyses and made the first draft of the manuscript. All authors (NL, SS, FR, LK, ML, KHR, JEH, GSA, MK and FP) contributed substantially to the analyses and interpretation of the findings, commented on the manuscript and all authors read and approved the final manuscript. FP is the guarantor of this work.
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM
(PDF 811 kb)
Rights and permissions
About this article

Cite this article
Lindekilde, N., Scheuer, S.H., Rutters, F. et al. Prevalence of type 2 diabetes in psychiatric disorders: an umbrella review with meta-analysis of 245 observational studies from 32 systematic reviews. Diabetologia 65, 440–456 (2022). https://doi.org/10.1007/s00125-021-05609-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-021-05609-x