Article Text

Abstract
Objective To describe patient characteristics and healthcare costs associated with uveitic macular oedema (UME) in US clinical practices from a commercial payer’s perspective.
Methods and analysis The IBM MarketScan Commercial Subset (1 October 2015–31 March 2020) was used to identify patients with non-infectious uveitis (NIU), with or without UME. Patients with UME at any time were further classified into subgroups of patients who received a UME diagnosis during the study period and those who received a UME diagnosis and local steroid injection (LSI) during the study period. Demographic and clinical characteristics, NIU-related treatments and healthcare costs were described for each cohort and subgroup during the most recent 12 months of continuous health plan enrolment. Healthcare costs were also described by vision status among all patients with NIU.
Results A total of 36 322 patients with NIU were identified, of whom 3 301 (9.1%) had UME and 33 021 (90.9%) had no UME. Patients with UME more frequently received NIU-related treatment compared with those without UME (64.6% vs 45.0%), particularly LSI treatment (12.5% vs 0.7%). Mean total all-cause healthcare costs per-patient-per-year (PPPY) were higher among patients with UME ($19 851) than patients without UME ($16 188) and were especially high among those with bilateral UME ($24 162). Further, vision loss was more commonly observed in those with UME versus those without UME (5.7% vs 2.2%) and a trend of increasing healthcare costs with increasing vision loss was observed.
Conclusion NIU is associated with substantial clinical and economic burden, particularly when UME is present.
- macula
- choroid
- drugs
- inflammation
Data availability statement
Data may be obtained from a third party and are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Uveitic macular oedema (UME) is the most common complication of non-infectious uveitis (NIU) and is associated with numerous clinical consequences, including vision loss, which may result in a substantial economic burden.
What are the new findings?
This retrospective cohort study of commercially insured patients suggested that UME was associated with increased vision loss and NIU-related treatment use compared with NIU alone, which resulted in higher costs among patients with UME.
How might these results change the focus of research or clinical practice?
With the lack of targeted and approved treatment for UME, these findings suggest an unmet need for appropriate and effective therapy that may help to alleviate the clinical and economic burden of UME.
Introduction
Non-infectious uveitis (NIU) is the most common type of uveitis in the US, with an adult prevalence of 121 cases per 100 000 persons in 2012.1 The ocular condition is characterised by inflammation of the uveal tract that may be idiopathic or associated with systemic autoimmune diseases.2 3 NIU can present as anterior, intermediate, posterior or panuveitic inflammation, affecting either one or both eyes.2 3
The most common complication of NIU is uveitic macular oedema (UME), which is caused by the breakdown of the blood-retinal barrier, resulting in accumulation of fluid and thickening of the retina.2 4 The prevalence of UME among patients with uveitis ranges from 9% to 70% depending on the anatomical location of uveitis,5 with one study reporting an overall frequency of 33%.6 As the main reason for vision loss (including blindness) in patients with NIU, UME is associated with significant and long-term clinical consequences.2 Indeed, NIU and its complications may lead to lower quality of life as well as work loss and disability.7 8 Additionally, NIU is associated with ocular comorbidities, such as optic nerve disease, glaucoma and cataracts, and patients with these comorbidities have been found to experience a lower quality of life than those without.9
Despite the large clinical burden of UME, there are currently no treatments approved by the US Food and Drug Administration (FDA) specifically for this condition. As such, management relies on the use of NIU therapies to indirectly treat UME and control inflammation.10 Frontline treatment typically consists of local (ie, topical and/or injection) corticosteroids, though systemic corticosteroids may be needed for patients with bilateral disease or associated systemic inflammatory disease.2 4 11 While effective at reducing inflammation, corticosteroids, especially their long-term use, are associated with numerous adverse reactions, including cataracts, glaucoma and increased intraocular pressure for local applications, or hypertension, diabetes, osteoporosis and atherosclerosis for systemic corticosteroids.11 Immunosuppressants and biological therapies may be considered for persistent UME (eg, after corticosteroid failure), but some recalcitrant cases may still require vitreoretinal surgery.11
The clinical consequences of UME, including vision loss and other ocular complications, paired with the large range of currently available treatments, may translate to a substantial economic burden. However, there is a paucity of real-world evidence describing the UME population as a standalone condition and quantifying the healthcare costs associated with the condition in the US. Therefore, the current study was conducted to provide a comprehensive characterisation of patient characteristics and healthcare costs associated with UME in US clinical practice from a commercial payer’s perspective.
Methods
Data source
The IBM MarketScan Commercial Subset was used (1 October 2015–31 March 2020). This database consists of employer-sourced and health plan-sourced data containing medical and pharmacy claims data for beneficiaries, comprising employees, their spouses and dependents who are covered by employer-sponsored private health-insurance. All US census regions are represented. The database includes the employer-paid portion of payments and any out-of-pocket expenses incurred by patients. The database also includes standard demographic variables such as year of birth and gender; however, information on race is not available.
Data are deidentified and comply with the requirements of the Health Insurance Portability and Accountability Act. Therefore, no institutional review board approval was needed.
Study design and sample selection
A retrospective cohort study design was used. Patients with NIU were classified into the following two mutually exclusive cohorts based on the presence or absence of UME: (1) UME cohort, comprising patients with NIU and an observed diagnosis of UME (ie, diagnosis of ME within 6 months before or any time after the first observed NIU diagnosis) at any time; and (2) NIU without UME cohort, comprising patients with NIU but no observed diagnosis of ME at any time. Patients in the UME cohort were further classified into subgroups based on whether they had (1) a recorded diagnosis of UME during the study period (defined below; ie, considered actively followed by a healthcare provider) or (2) a recorded diagnosis of UME during the study period AND a local steroid injection (LSI) during the study period. An LSI was defined based on the use of a subconjunctival injection, injection into the Tenon’s capsule, or intravitreal injection.
To capture a representative sample of patients with NIU in real-world clinical practice (ie, including patients with both a current or historical diagnosis of NIU), the most recent 12 months of continuous enrolment was used to define the study period, ending at the earliest of the end of data availability (31 March 2020), end of continuous health plan enrolment or start of Medicare supplemental enrolment. The index date was defined as the start date of the most recent 12 months of continuous enrolment and was required to occur on or after the first observed UME diagnosis (UME cohort) or NIU diagnosis (NIU without UME cohort). The baseline period comprised the 12-month period prior to the index date.
Sample selection
Patients were included in the study if they met the following criteria: (1) had ≥2 NIU diagnoses on distinct dates at any time (online supplemental table S1); (2) had no indicator of infectious uveitis (IU) at any time (ie, a diagnosis of IU or the administration of an LSI with an anti-infective agent); (3) had no indicator of diabetic macular oedema (DME) or retinal vein occlusion (RVO) at any time (ie, a diagnosis of DME or RVO or the use of an anti–vascular endothelial growth factor (anti-VEGF) treatment); (4) had ≥24 months of continuous health plan enrolment any time after their first observed UME diagnosis (UME cohort; online supplementary table S1) or their first NIU diagnosis (NIU without UME cohort) and (5) were aged between 18 and 64 years as of their index date. Anterior, intermediate, posterior or panuveitic NIU patients were included (not mutually exclusive), and classifications were determined in collaboration with clinical experts (online supplemental table S2).
Supplemental material
Study measures, outcomes and statistical analysis
All results were descriptively reported using means, standard deviations (SDs) and medians for continuous variables, and frequency counts and percentages for categorical variables. All results were described separately for the UME and NIU without UME cohorts and the UME subgroups. No statistical comparisons between cohorts were conducted; all differences reported in this study are numerical.
Patient characteristics were described and included demographic characteristics on the index date (ie, age, sex, region, health plan type), clinical characteristics (ie, Charlson Comorbidity Index and comorbidities during the baseline period; type of NIU, UME affected eye(s), and vision loss at any time), and NIU-related treatments during the study period (ie, vitreoretinal surgery, local treatments (ocular drops, LSI), systemic treatments (oral corticosteroids, immunosuppressants, biologicals)). Among patients in the UME cohort, UME-affected eye(s) was classified based on observed diagnoses using the following mutually exclusive hierarchy: bilateral, unilateral and unspecified eye. For example, using this hierarchy, a patient with diagnoses for both bilateral and unilateral UME was considered to have bilateral UME. Similarly, among all patients with NIU, vision loss status was classified based on observed diagnoses using the following mutually exclusive hierarchy: blindness, severe vision loss, moderate vision loss and no indicator of vision loss. For example, a patient with indicators of both blindness and severe vision loss was classified as a patient with blindness. Vision loss status was defined as previously described by Javitt et al12 and updated to International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) diagnosis codes.
Healthcare costs were described during the study period among patients with complete financial data available, adjusted to 2020 USD using the Bureau of Labor Statistics Medical Care Component,13 and reported from a payers’ perspective on a per-patient-per-year (PPPY) basis. Healthcare costs included medical (consisting of inpatient, outpatient and emergency department) and pharmacy (including NIU treatment-related) components. Among the UME cohort and subgroups, costs were also described separately by UME-affected eye(s).
Healthcare costs stratified by vision status
Additionally, healthcare costs were described by vision status (ie, blindness, severe vision loss, moderate vision loss and no indicator of vision loss) among a separate cohort of patients with ≥1 NIU diagnosis at any time, 12 months of continuous health plan enrolment at any time, complete financial data, and aged between 18 and 64 years as of their index date (ie, the start date of the most recent 12 months of continuous enrolment). Healthcare costs measured in the 12-month period (PPPY) included medical (ie, eye-related (inpatient, outpatient, emergency department) and non-eye-related, as defined by Javitt et al12) and pharmacy components.
Replication analysis
Sample selection (online supplemental figure S1) and analysis of healthcare costs stratified by vision status (online supplemental figure S2) were replicated among Medicare beneficiaries using the standard Medicare 5% analytic sample (1 October 2015–31 December 2018).
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Results
A total of 36 322 patients with NIU were identified, of whom 3 301 (9.1%) were classified in the UME cohort and 33 021 (90.9%) were classified in the NIU without UME cohort. Within the UME cohort, 1 577 (47.8%) had a diagnosis of UME during the study period, of whom 367 (23.3%) had an LSI during the study period.
Patient characteristics
Patients with UME had a mean age of 50.1 years, and 59.3% were female. Among patients with NIU without UME, mean age was 47.5 years and 58.5% were female. The mean Charlson Comorbidity Index score was 0.5 in both cohorts. The most frequent comorbidities observed during the baseline period included hypertension (34.5% among patients with UME and 30.9% among patients with NIU without UME), rheumatoid arthritis and collagen vascular diseases (13.0% and 15.9%), and obesity (14.9% and 14.2%; table 1).
Demographic and clinical characteristics
Among all patients with NIU, the most common type of NIU observed at any time was anterior (80.4% among patients with UME and 87.1% among patients with NIU without UME). Posterior NIU was more commonly observed among patients with UME (34.0%) than patients without UME (10.6%). Among patients with UME, bilateral UME was most common in those with UME and an LSI during the study period (50.1%). Furthermore, patients with UME more frequently experienced vision loss (5.7%) than those without UME (2.2%), particularly among patients with UME and LSI during the study period (7.9%; table 1).
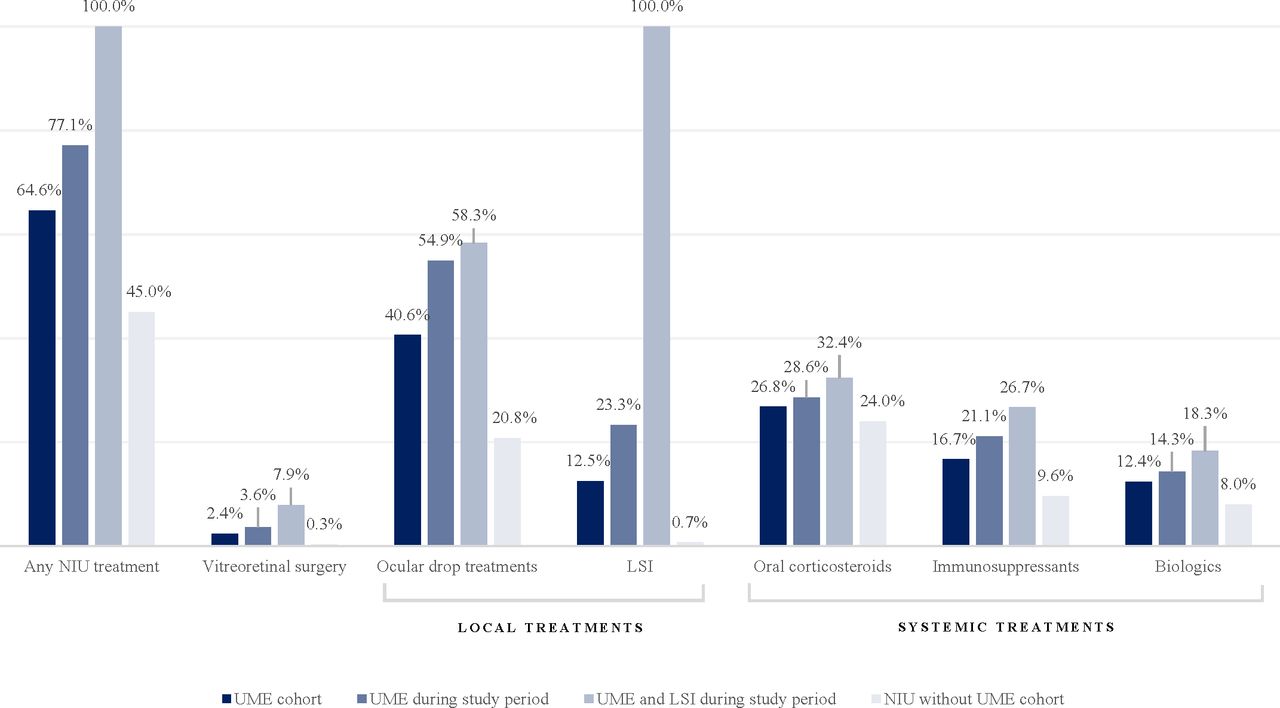
With regards to treatments, patients with UME more frequently received any NIU-related treatment (64.6%) compared with those without UME (45.0%; Figure 1). This difference was particularly pronounced for LSI treatment (12.5% vs 0.7%). In general, the higher rate of treatment among patients with UME was driven by those with UME and LSI during the study period.

NIU-related treatments. LSI, local steroid injection treatment; NIU, non-infectious uveitis; UME, uveitic macular oedema.
Healthcare costs
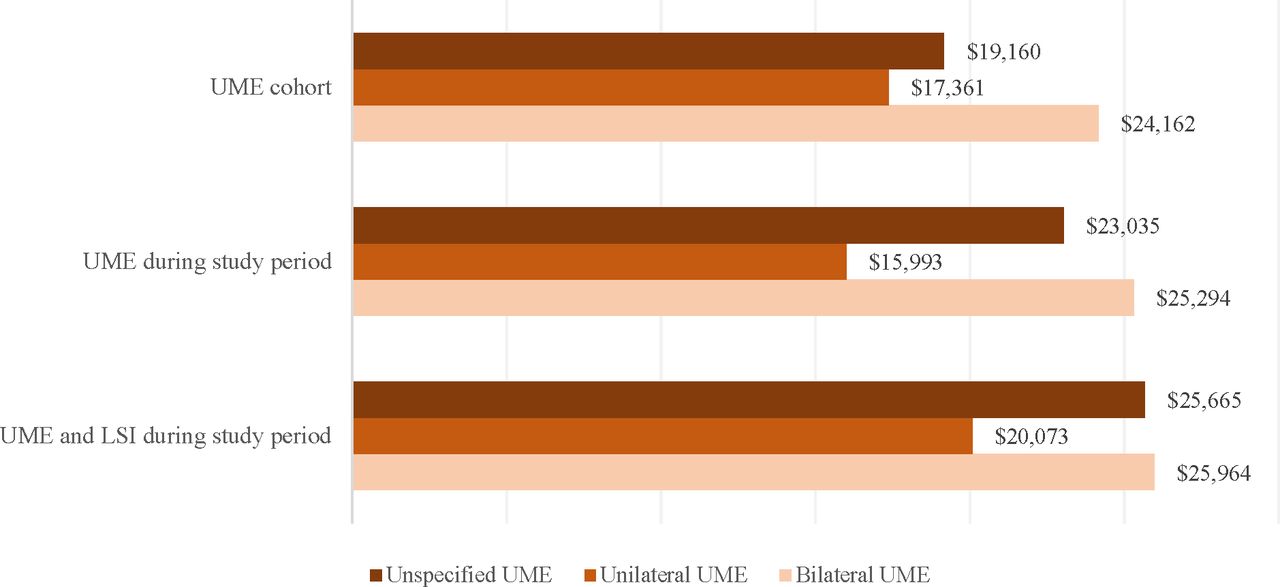
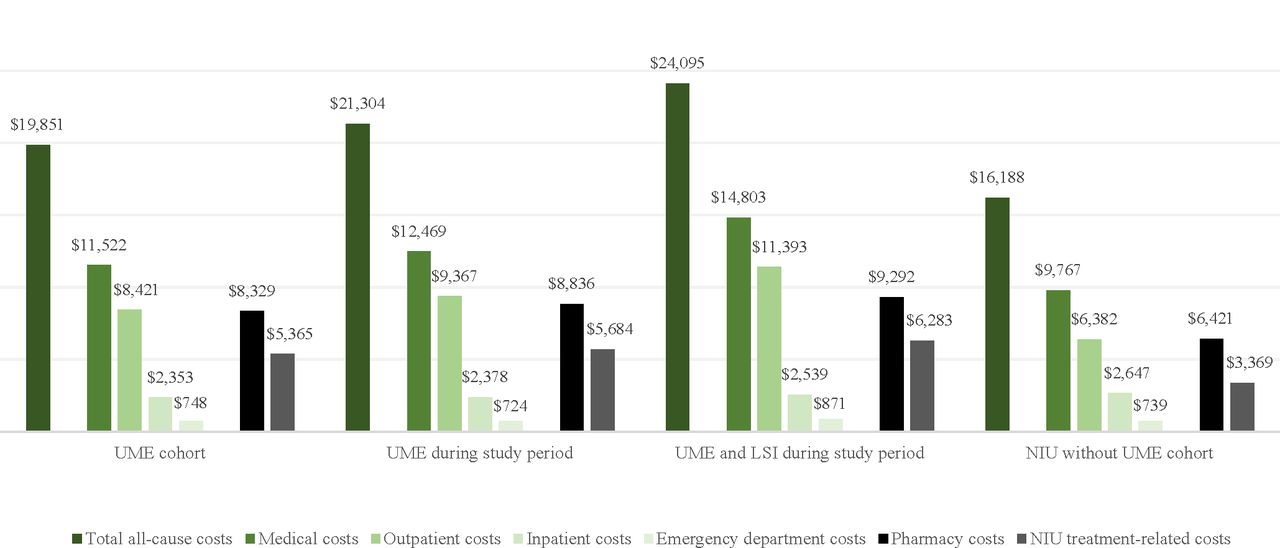
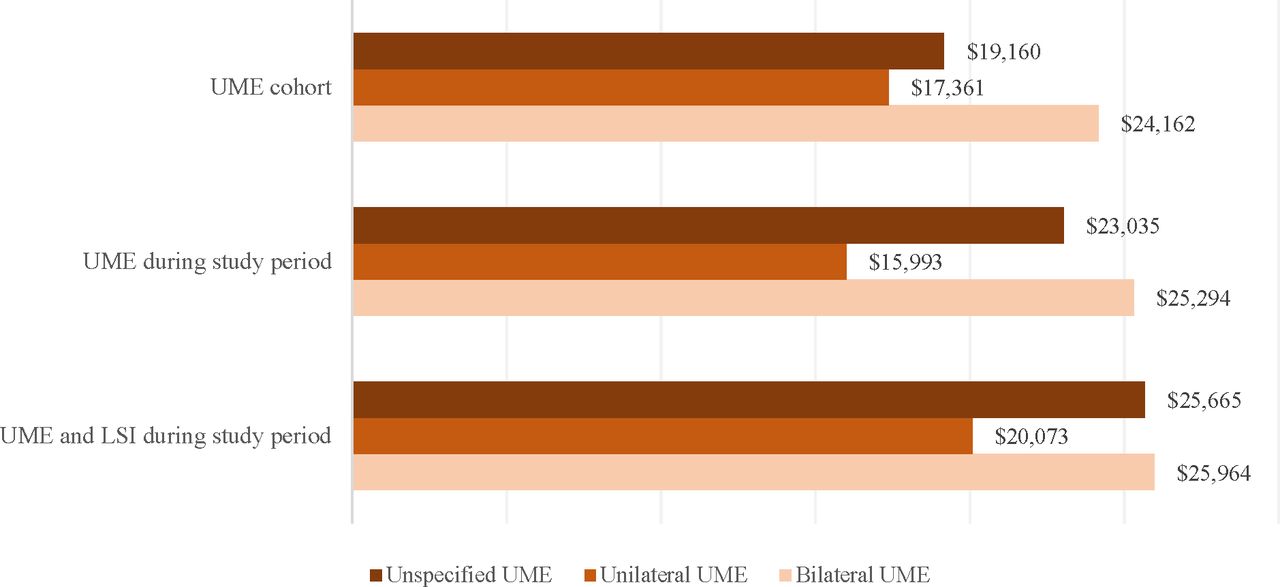
Total mean all-cause healthcare costs PPPY were higher among patients with UME ($19 851) than patients with NIU without UME ($16 188), with outpatient ($8 421 vs $6 382) and pharmacy costs ($8 329 vs $6 421) being the main drivers of the difference (figure 2). Among patients with UME, bilateral disease was associated with the highest mean healthcare costs PPPY ($24 162), which remained consistent across UME cohort subgroups (figure 3).

Mean annual healthcare costs by UME status. LSI, local steroid injection treatment; NIU, non-infectious uveitis; UME, uveitic macular oedema.
{kind=link}
{kind=link}
{kind=link}
Mean annual total all-cause healthcare costs by uveitic macular oedema (UME)-affected eye(s). LSI, local steroid injection.
Healthcare costs stratified by vision status
Among 90 974 patients with an ≥1 NIU diagnosis, vision loss was associated with increased all-cause healthcare costs, which were primarily driven by non-eye-related medical costs (table 2). There was a trend of increasing costs with increasing vision loss. Indeed, among patients with an indicator of blindness, mean medical costs PPPY totalled $53 767 ($48 560 non-eye-related) and mean pharmacy costs totalled $11 606.
Annual healthcare costs by vision status among patients with NIU
Discussion
This retrospective cohort study of commercially insured patients demonstrated that NIU is associated with substantial clinical and economic burden, particularly when UME is present. UME was associated with increased vision loss and NIU-related treatment use compared with NIU alone. This clinical burden translated to higher costs associated with UME compared with NIU alone, which were highest among patients with bilateral disease and those with blindness. Taken together, these findings suggest an unmet need for appropriate and effective management, particularly when UME is present.
NIU, and particularly UME, are not well-characterised in the real-world setting. One retrospective analysis of claims data estimated an annual NIU prevalence of 121 cases per 100 000 adults in the US, however, the prevalence of complications such as UME were not assessed.1 Other claims-based studies of NIU have omitted assessment of UME or its impact on real-world outcomes.7 14 Further, epidemiological literature has reported a wide range in the prevalence of UME among patients with uveitis, ranging from 9% to 70% depending on anatomical location.5 Of note, the 9.1% prevalence of UME found in the current study is expected to be under-reported, since current reimbursement practices may not include regular coding of UME based on the lack of FDA-approved treatments to manage UME. Therefore, consistent with previous studies, the number of patients identified with UME in the current study likely represents a lower bound estimate of the potential true NIU population affected by UME.
To our knowledge, this is the first study to evaluate the economic burden of UME specifically in the commercially insured US population. Patients with UME incurred $19 851 PPPY in mean all-cause healthcare costs compared with $16 188 PPPY among patients with NIU without UME, which is consistent with two prior cost estimates of NIU among privately insured patients in the US.7 14 Thorne et al estimated total direct healthcare costs of $12 940 (2012 USD) during a 1-year study period for patients with intermediate or posterior NIU or panuveitis,7 which, when inflated to 2020 USD ($16 182), is very similar to the current estimate for the NIU population. In a separate study by Chu et al, total monthly healthcare costs totalled $1 144–$2 689 (ie, $13 728–$32 268 annually; 2009 USD) for patients with chronic NIU treated with corticosteroids, immunosuppressants or biologicals.14 These costs are higher than the current estimates likely due to the fact that Chu et al focused only on treated patients. Of note, neither of these studies identified the proportion of patients with UME in their populations, which limits comparability with the current study. Based on the literature, the annual healthcare costs of UME observed in this study are within the range of or higher than those of other eye conditions, including DME ($11 290–$29 959 depending on insurance coverage),15 16 RVO ($3 285–$11 587 depending on type and insurance coverage)17 18 and macular degeneration ($334–$4 030 depending on type and treatment),19 emphasising the importance of the large economic burden of UME in the US.
The high healthcare costs observed in this study may have been driven by several factors, including the high frequency of bilateral disease among patients with UME (27.4%), especially among the subgroup with UME and LSI during the study period (50.1%). Indeed, bilateral disease was associated with the highest costs PPPY ($24 162) compared with unilateral ($17 361) or unspecified disease ($19 160). Additionally, increasing vision loss resulted in progressively higher medical costs, ranging from $11 054 among patients with no indicator of visual loss to $53 767 among those with blindness. Not only does vision loss result in substantial medical costs, it also negatively affects quality of life,20 21 increases the risk of physical and mental health comorbidities (eg, depression, stroke, premature death),22 and decreases work productivity,23 all of which contribute to the large burden of eye conditions like UME.
Pharmacy costs were also a driver of the high costs associated with UME, reflecting the increased rate of treatment among patients with UME compared with those with NIU without UME (64.6% vs 45.0%). Of note, from a clinical standpoint, all patients with active UME or NIU would be expected to be treated, however, treatment rates were measured among a representative sample of patients with UME or NIU at any time, which included both patients with active and resolved disease during the study period, who may or may not require treatment. The high rates of NIU treatment in addition to increased medical costs among patients with UME suggests a potential unmet need for targeted management of the condition in this patient population. Indeed, guidelines for the treatment of UME currently do not exist, and within existing guidelines for NIU, there is limited guidance regarding the management of UME.24 25 This observation reveals a lack of differentiation of UME in coding as a distinct entity by eye specialists, possibly due to the fact that no UME treatment is currently FDA-approved. Additionally, there is evidence that current NIU treatment options are suboptimal for UME. In a retrospective analysis of patients with UME from tertiary academic ocular inflammation centres in the US, the rate of improvement of UME-induced visual impairment was only 41% after 3 months of care, and nearly 50% of patients were still experiencing decreased visual acuity after 6 months despite treatment per best medical judgement at the time of the study period (1978–2007).26 Moreover, current systemic NIU treatment options are associated with systemic adverse events like diabetes, osteoporosis and hypertension, while local treatments are associated with a high risk of ocular complications (eg, cataracts, increased ocular pressure, glaucoma),2 27 which may further contribute to clinical burden and costs. Of note, a cross-sectional study of patients with NIU found that treatment with oral corticosteroids or immunosuppressants was associated with worse quality of life, emphasising the far-reaching clinical implications of these therapies.9 Taken together, these findings highlight the limitations of current treatment options for UME (none of which are approved by the FDA) and the need for more effective and safe therapies that specifically target UME and that may help to alleviate the associated clinical and economic burden.
Limitations
The findings of this study should be interpreted in the context of some limitations. Indicators of vision loss may be under-reported in claims data; however, it was assumed that these indicators were missing at random. Similarly, as there are currently no treatments approved for UME, recorded diagnoses of UME were expected to be under-reported in claims data; however, it was assumed that recorded UME diagnoses were missing at random. Due to the expected under-reporting of UME in claims data, it is possible that some patients with UME were classified in the NIU without UME cohort as it was not possible to identify these patients in the absence of a recorded UME diagnosis. This may have led to an underestimation of the cost difference observed between patients with and without UME found in this study. In addition, this analysis reflected the burden of NIU and UME from October 2015 to March 2020, which may change as the treatment landscape evolves. Further, since this study was conducted in a commercially insured population, the results may not be generalisable to those with other types of insurance (eg, Medicare, Medicaid) or no insurance coverage. Finally, as with all claims-based studies, there may have been billing inaccuracies or omissions in coded procedures, diagnoses and pharmacy claims.
Conclusion
The substantial burden of UME observed in the current study, particularly associated with bilateral NIU and vision loss, goes beyond the existing burden of NIU and highlights the need for increased awareness and effective and timely management of the condition. Future studies are warranted to determine if the development of targeted therapy for UME may help to reduce the considerable clinical and economic burden.
Data availability statement
Data may be obtained from a third party and are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
Data are de-identified and comply with the requirements of the Health Insurance Portability and Accountability Act. Therefore, no institutional review board approval was needed.
Acknowledgments
Certain data used in this study were supplied by International Business Machines Corporation as part of one or more IBM MarketScan Research Databases. Any analysis, interpretation, or conclusion based on these data is solely that of the authors and not International Business Machines Corporation.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors PG-S, ES, JB and AG contributed to study conception and design, collection and assembly of data, and data analysis and interpretation. SMH, GJ, SB and TAA contributed to study conception and design, data analysis and interpretation. AG was responsible for the overall content as the guarantor. All authors reviewed and approved the final content of this manuscript.
Funding This study was funded by Bausch Health US, LLC.
Competing interests SMH is a consultant or on the speakers bureau for Allergan; Bausch Health US; Novartis Pharmaceuticals Corporation; Biogen; EyePoint Pharmaceuticals; Alimera Sciences; Spark Therapeutics and Regeneron Pharmaceuticals. GJ is an employee of Bausch Health US, which funded the development and conduct of this study and manuscript. PG-S, ES, JB and AG are employees of Analysis Group, a consulting company that has provided paid consulting services to Bausch Health US. TAA is consultant for Adverum Biothechnologies; Allergan; Genentech; Novartis Pharmaceuticals Corporation; Beaver-Visitec International; EyePoint Pharmaceuticals; Bausch Health US and NGM Biopharmaceuticals.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.